Rheumatoid arthritis
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND treatment
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Rheumatoid Arthritis based on Goldman-Cecil Medicine and the Textbook of Family Medicine.
Rheumatoid Arthritis (RA)
Definition and Overview
Rheumatoid arthritis is a chronic inflammatory systemic disease in which cellular and autoimmune mechanisms cause destruction of tissues, primarily the synovium. Disease manifestations range from mild, self-limited polyarthritis to multi-organ destruction and premature death. Patients with active, polyarticular, RF-positive RA have >70% chance of developing joint damage or erosion within 2 years without treatment.
The underlying pathogenesis involves an early breach of tolerance to post-translationally modified self-proteins (typically citrullination, acetylation, or carbamylation), leading to autoantibody production, cytokine/chemokine release, and dysregulated metabolism - sometimes up to 10 years before clinically detectable disease.
Epidemiology
- Prevalence: 1-2% of adults
- Sex ratio: Women affected ~3:1 over men
- Peak onset: Ages 20-50 years, but occurs at all ages
- Genetics: Higher concordance in monozygotic vs. dizygotic twins; linked to HLA-DR (MHC class II). The "shared epitope" on DRβ1 chains is particularly important for antigen recognition. Other risk genes include PTPN22, CTLA4, CD28, CD40, and PAD (peptidyl arginine deiminase - the enzyme that converts arginine to citrulline, generating a key RA autoantigen).
Pathogenesis
The sequence of events:
- Genetic predisposition (HLA shared epitope + other SNPs) creates susceptibility
- Post-translationally modified peptides (citrullinated proteins) bind abnormally to HLA molecules on dendritic cells or B cells
- Altered HLA-TCR interactions cause loss of self-tolerance in auto-reactive T cells
- Autoantibodies are produced (RF targets IgG Fc fragment; ACPA/anti-CCP targets citrullinated proteins)
- The synovial lining proliferates, forming pannus - an invasive tissue of activated leukocytes and stromal cells
- Inflammatory cytokines (TNF, IL-6) drive local cartilage and bone destruction via proteases
Clinical Features
Joint Manifestations
- Hallmark: Symmetric synovitis with morning stiffness ≥1 hour
- Early joints: Small joints of hands (PIP, MCP) and feet (MTP) - DIP joints are typically spared
- Later involvement: Wrists, knees, elbows, ankles, hips, shoulders
- Characteristic deformities (advanced disease):
- Ulnar deviation at MCPs
- Swan-neck deformity
- Boutonniere deformity
- Hallux valgus / forefoot deformities

Cervical Spine
The C1-C2 articulation is commonly involved. Bony erosions and ligament damage can cause atlantoaxial subluxation. Minor subluxation is usually asymptomatic, but severe cases cause cervical cord compression with neurologic symptoms or death. Patients should avoid forced neck flexion.
Baker Cyst
Excess synovial fluid from the knee accumulates in the popliteal fossa. These cysts can compress popliteal neurovascular structures, dissect into the calf, or rupture - mimicking DVT (pseudothrombophlebitis syndrome).
Other Joints
Temporomandibular, cricoarytenoid (hoarseness, throat fullness, rarely acute stridor), and sternoclavicular joints may be involved.
Extra-Articular Manifestations
More common in RF- or ACPA-positive patients:
| System | Manifestation |
|---|---|
| Systemic | Fatigue, weight loss, low-grade fever |
| Skin | Subcutaneous nodules (~20%, on extensor surfaces) - almost exclusively in seropositive patients |
| Cardiovascular | Pericarditis, accelerated atherosclerosis |
| Pulmonary | Pleuritis, interstitial lung disease, nodules |
| Eye | Scleritis, episcleritis, keratoconjunctivitis sicca |
| Hematologic | Anemia of chronic disease (proportional to disease activity); Felty syndrome (RA + splenomegaly + neutropenia) |
| Neurologic | Peripheral neuropathy, cervical myelopathy from C1-C2 subluxation |
Diagnosis
RA has no single pathognomonic finding. It is a clinical diagnosis requiring a combination of features. Inflammatory changes may be confirmed by ultrasound or MRI in early disease.
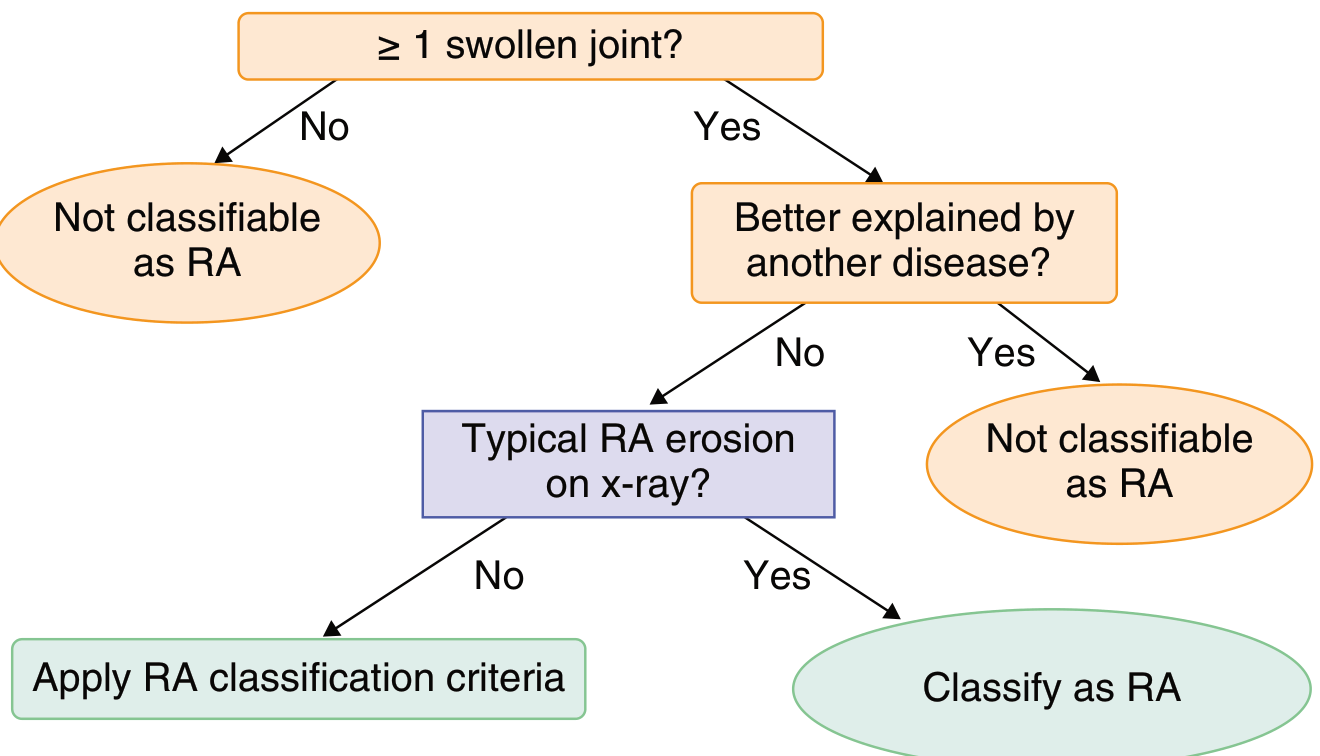
ACR/EULAR 2010 Classification Criteria (score ≥6 = RA)
| Domain | Score |
|---|---|
| Joint involvement | 1 medium-large joint = 0; 2-10 medium-large = 1; 1-3 small joints = 2; 4-10 small joints = 3; >10 joints (including ≥1 small) = 5 |
| Serology | Negative RF and ACPA = 0; Low-positive = 2; High-positive (>3× ULN) = 3 |
| Acute phase reactants | Normal CRP and ESR = 0; Abnormal = 1 |
| Duration | <6 weeks = 0; ≥6 weeks = 1 |
A score ≥6/10 classifies a patient as having RA. Additionally, if typical RA erosions are present on X-ray, the patient can be directly classified as RA without applying the scoring system.
Laboratory Findings
- Rheumatoid factor (RF): Positive in ~75%; associated with more severe articular and extra-articular disease; not specific (also seen in SBE, hepatitis, Sjogren's, normal elderly)
- Anti-CCP (ACPA): Positive in ~70%; high specificity 93-98%; may appear years before clinical disease; marker of aggressive erosive disease
- Seronegative RA: ~15% negative for both RF and ACPA
- ANA: Positive in ~30%
- Anemia of chronic disease: Common; severity proportional to disease activity
- ESR/CRP: Elevated in active disease
- Synovial fluid: >2,000 WBC/mm³ without crystals
Treatment
Early, aggressive treatment is essential. The goal is remission or lowest possible disease activity ("treat-to-target" strategy).
Treatment Pyramid
1. NSAIDs - Symptomatic relief only; no disease modification
2. Glucocorticoids - Used as bridge therapy until DMARDs take effect (typically 2-6 months). Prednisone >10 mg/day is rarely indicated for articular disease; taper to lowest effective dose; always prophylax against osteoporosis. Toxic risk associated with average dose >8 mg/day.
3. Conventional synthetic DMARDs (csDMARDs)
- Methotrexate (MTX) - First-line anchor drug for most patients; monitor LFTs, CBC, renal function
- Hydroxychloroquine - Least toxic DMARD; 200 mg once or twice daily; requires ophthalmologic follow-up every 6 months; best for mild RA
- Sulfasalazine - 2-3 g/day in divided doses; check CBC and LFTs; limited to patients without poor prognostic factors
- Leflunomide - Alternative to MTX
- Others: azathioprine, gold (historical)
4. Biologic DMARDs (bDMARDs) - Used when csDMARDs are insufficient
| Agent | Class | Dosing |
|---|---|---|
| Etanercept | TNF inhibitor | 50 mg SQ weekly |
| Adalimumab | TNF inhibitor | 40 mg SQ every 2 weeks |
| Infliximab | TNF inhibitor | 3-5 mg/kg IV at 0, 2, 6 weeks then q4-8 weeks (with MTX) |
| Certolizumab | TNF inhibitor | 400 mg SQ at wks 0, 2, 4 then 200 mg q2 weeks |
| Golimumab | TNF inhibitor | 50 mg SQ monthly |
| Tocilizumab | IL-6R inhibitor | 4-8 mg/kg IV q4 weeks |
| Abatacept | T-cell co-stimulation blocker | 500-1000 mg IV at 0, 2, 4 weeks then q4 weeks |
| Rituximab | Anti-CD20 (B-cell depletion) | 2 × 1000 mg IV, 2 weeks apart; repeat q16-24 weeks (with MTX) |
5. Targeted synthetic DMARDs (tsDMARDs) - JAK inhibitors
- Tofacitinib - 5 mg PO twice daily
- Baricitinib - 2 or 4 mg PO once daily
- Upadacitinib - 15 mg PO once daily
ACR Adverse Prognostic Factors (favor early DMARD use)
- Functional limitation
- Extra-articular disease
- RF positivity or anti-CCP antibodies
- Bony erosions on radiograph
Non-Pharmacologic
- Physical and occupational therapy for joint protection during exacerbations
- Exercise to improve function and range of motion
- Patient and family education on DMARD compliance
- Early rheumatology consultation is generally recommended
Poor Prognostic Factors
- High-titer RF or ACPA positivity
- Radiographic erosions within first 2 years
- Active polyarticular disease
- Extra-articular manifestations
- Elevated ESR/CRP
- Functional disability at presentation
Comorbidities
RA carries substantial comorbidities: cardiovascular disease (major cause of excess mortality), psychological disease, malignancy (especially lymphoma), and systemic osteoporosis. Cardiovascular risk management is a parallel priority in RA care.
Sources: Goldman-Cecil Medicine International Edition (2 Vol Set) | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.