Laryngeal muscles,nerve supply and sequence due to nerve or blood supply damage
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
Laryngeal Muscles: Anatomy, Nerve Supply, and Consequences of Nerve/Blood Supply Damage
1. Overview of Laryngeal Nerve Supply
All motor and sensory nerves of the larynx arise from the vagus nerve (CN X) via two branches:
| Nerve | Origin | Course |
|---|---|---|
| Superior Laryngeal Nerve (SLN) | Inferior ganglion of vagus | Descends lateral to pharynx, divides at level of greater horn of hyoid |
| Recurrent Laryngeal Nerve (RLN) | Vagus in thorax | Right: loops under right subclavian artery. Left: loops under aortic arch and ligamentum arteriosum |
SLN Branches:
- External branch (motor) - supplies cricothyroid muscle (the only intrinsic muscle NOT supplied by RLN)
- Internal branch (sensory + secretomotor) - pierces thyrohyoid membrane with superior laryngeal artery; supplies mucosa above the vocal folds (epiglottis, vallecula, aryepiglottic fold, vestibule)
RLN:
- Ascends in the tracheoesophageal groove accompanied by the inferior laryngeal artery
- Enters larynx behind the cricothyroid joint
- Divides into motor branch (supplies ALL intrinsic muscles except cricothyroid; motor fibres derived from cranial root of accessory nerve CN XI via the vagus) and sensory branch (mucosa below vocal folds)
Note: Galen's anastomosis connects the internal SLN with an ascending branch of the RLN - this is purely sensory. Variable anastomoses between these nerves explain inconsistent clinical presentations after laryngeal nerve injuries.
2. Intrinsic Laryngeal Muscles and Nerve Supply
All intrinsic muscles are supplied by the RLN, except the cricothyroid (external branch of SLN).
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Posterior Cricoarytenoid (PCA) | Posterior cricoid lamina | Muscular process of arytenoid | Sole abductor of vocal folds (pulls muscular process posteriorly/inferiorly, rotates vocal process outward) | RLN |
| Lateral Cricoarytenoid (LCA) | Lateral cricoid arch | Muscular process of arytenoid | Vocal fold adduction (pulls muscular process forward, rotates vocal process inward/inferiorly) | RLN |
| Thyroarytenoid (TA) | Anterior inner surface of thyroid cartilage | Vocal process and anterior arytenoid | Adducts vocal fold; medial part = vocalis (controls length, tension, stiffness) | RLN |
| Interarytenoid (IA) | One arytenoid | Other arytenoid | Closes posterior glottis (transverse fibers); constricts laryngeal inlet (oblique fibers). Primary adductor of vocal fold | RLN - receives bilateral innervation (the only unpaired laryngeal muscle) |
| Aryepiglottic muscle | Arytenoid | Epiglottis (aryepiglottic fold) | Constricts laryngeal inlet | RLN |
| Cricothyroid (CT) | Anterior arch of cricoid | Thyroid cartilage | Closes cricothyroid space; tenses/lengthens vocal fold (pitch control); minor adduction | External branch of SLN |
3. Extrinsic Laryngeal Muscles and Nerve Supply
Depressors (infrahyoid "strap" muscles):
| Muscle | Nerve |
|---|---|
| Sternohyoid | Ansa cervicalis (C2, C3) |
| Omohyoid | Ansa cervicalis (C2, C3) |
| Thyrohyoid | C1 (via hypoglossal nerve) |
Elevators (suprahyoid muscles):
| Muscle | Nerve |
|---|---|
| Geniohyoid | C1 (via hypoglossal) |
| Mylohyoid | Mylohyoid branch of V3 (trigeminal) |
| Digastric - anterior belly | V3 (trigeminal) |
| Digastric - posterior belly | CN VII (facial) |
| Stylohyoid | CN VII (facial) |
Pharyngeal constrictors (relevant to larynx):
- Inferior constrictor + Cricopharyngeus - Pharyngeal plexus (CN IX + X)
4. Blood Supply of the Larynx
| Artery | Source | Area Supplied |
|---|---|---|
| Superior laryngeal artery | Superior thyroid artery | Supraglottic larynx; enters via thyrohyoid membrane alongside internal branch of SLN |
| Cricothyroid artery | Superior thyroid artery | Cricothyroid region; crosses the upper cricothyroid ligament (up to 5 branches) |
| Inferior laryngeal artery | Inferior thyroid artery | Subglottic/infraglottic larynx; ascends on trachea with RLN |
The three arteries form a communicating plexus in the paraglottic space. Venous drainage is via companion veins into the internal jugular vein.
5. Sequence of Events Following Nerve Damage
A. Unilateral RLN Injury
Semon's Law: With progressive/partial RLN injury, the abductor (PCA) is paralyzed first, before the adductors. During recovery, the adductors recover first.
- Paralyzed cord lies in the paramedian (adducted) position - adductors dominate.
- Symptoms: Hoarseness, flaccid dysphonia (breathy + harsh voice), short phrases, reduced loudness, mild inspiratory stridor on speech, possible diplophonia (two pitch levels due to unequal cord vibration).
- Voice quality usually improves over time; the normal cord crosses the midline to compensate.
- On laryngoscopy: affected cord near midline; normal cord crosses to meet it during phonation.
- Adductor muscles affected first with peripheral RLN injury (Seimon law).
B. Bilateral RLN Injury (e.g., after total thyroidectomy)
- Acute: Both PCAs (abductors) paralyzed; unopposed cricothyroid tension (SLN intact) → vocal folds meet at midline → stridor, severe respiratory distress, may require emergency tracheostomy.
- Chronic: Laryngeal musculature atrophies over time → various compensatory mechanisms → airway problems less severe, but aphonia may result when cords cannot contact each other.
C. Unilateral SLN (External Branch) Injury
- Loss of cricothyroid function (tensor of vocal fold) ipsilaterally.
- Symptoms: Minimal if unilateral - mild hoarseness, loss of high-pitched phonation, fatigue of voice.
- The anterior commissure may rotate slightly toward the affected side.
D. Bilateral SLN (External Branch) Injury
- Symptoms: Hoarseness, tiring of voice, loss of high notes - significant voice fatigue. Risk of aspiration (loss of tension and sensory input).
E. Unilateral Vagus Nerve Injury (above origin of SLN)
- Affects both SLN and RLN on that side.
- Symptoms: Hoarseness (same as unilateral RLN palsy) - the vocal cord adopts a more lateral/abducted ("cadaveric") position because cricothyroid is also paralyzed.
F. Bilateral Vagus Nerve Injury
- Affects both SLN + RLN bilaterally.
- Vocal folds: Flaccid, midpositioned ("cadaveric" position) - similar to succinylcholine effect.
- Symptoms: Severe aphonia, but paradoxically airway control is rarely a problem (cords are not tightly adducted because the adductors are also paralyzed).
| Nerve Injured | Unilateral Effect | Bilateral Effect |
|---|---|---|
| External SLN | Minimal (loss of high pitch) | Hoarseness, voice tiring |
| RLN | Hoarseness, cord in paramedian position | Acute: stridor/respiratory distress; Chronic: aphonia |
| Vagus (CN X) | Hoarseness (cord in lateral/cadaveric position) | Aphonia; airway relatively preserved |
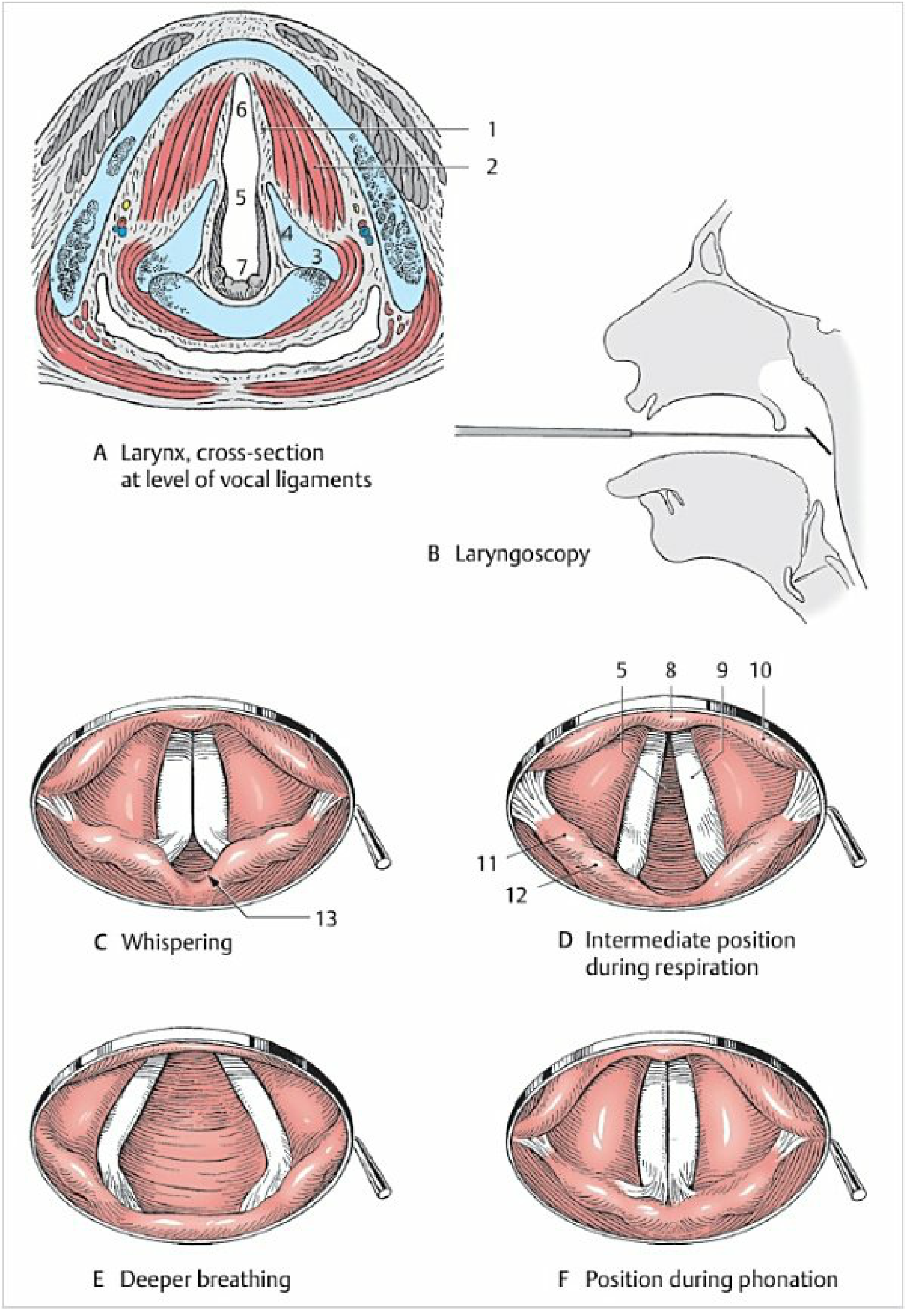
6. Summary of Vocal Cord Positions
| Situation | Cord Position |
|---|---|
| Normal quiet breathing | Intermediate (slightly abducted) |
| Deep breathing | Widely abducted (PCA active) |
| Phonation | Adducted (midline) |
| Whispering | Anterior cords adducted, posterior triangular gap open |
| Unilateral RLN palsy | Affected cord paramedian (adducted) |
| Bilateral RLN palsy | Both cords adducted at midline = respiratory emergency |
| Bilateral vagal palsy | Both cords in midposition (cadaveric) - flaccid |
7. Clinical Correlates of Blood Supply Damage
- Superior laryngeal artery enters the paraglottic space at the anterior end of the aryepiglottic fold - risk of injury during supraglottic endoscopic laser surgery; meticulous hemostasis required.
- Cricothyroid artery (up to 5 branches) crosses the upper cricothyroid ligament - at risk during cricothyroidotomy and endoscopic resection of anterior commissure cancers.
- Inferior laryngeal artery ascends with the RLN - injury during thyroid surgery may simultaneously compromise both vascular supply and nerve function.
Key Mnemonics:
- "ABDUCTOR is alone" (PCA) - the only abductor; paralyzed first in RLN palsy (Semon's law).
- "Cricothyroid is Superior" - the only intrinsic laryngeal muscle supplied by the external branch of the Superior laryngeal nerve.
- Bilateral RLN palsy = Emergency (cords adduct); Bilateral vagal palsy = Airway safer (cords midpositioned/flaccid).
Sources: K.J. Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Localization in Clinical Neurology 8e; Morgan & Mikhail's Clinical Anesthesiology 7e; Color Atlas of Human Anatomy Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.