Dilated rectum in anomaly scan
Reading File
Finding Sources
Finding Sources
Searching PubMed
fetal dilated rectum ultrasound prenatal
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
fetal dilated rectum imperforate anus prenatal
Reading File
Loading Image
Loading Image
I now have comprehensive information. Let me compile a thorough, well-structured answer.
Dilated Rectum on Fetal Anomaly Scan
Normal Reference Values
The fetal rectum gradually enlarges with gestation. A useful rule of thumb from Creasy & Resnik's is that bowel loops >7 mm are suggestive of obstruction. The table below gives normal colon and rectal diameters:
| GA (weeks) | Descending Colon mean (mm) | 95% CI | Rectal mean (mm) | 95% CI |
|---|---|---|---|---|
| 19–20 | 3.52 | 0.79–6.26 | 3.64 | 1.45–5.82 |
| 22 | 3.69 | 0.96–6.41 | 3.95 | 1.78–6.13 |
| 25 | 4.18 | 1.46–6.90 | 4.57 | 2.40–6.74 |
| 28 | 5.04 | 2.32–7.76 | 5.38 | 3.20–7.55 |
| 32 | 6.86 | 4.13–9.58 | 6.80 | 4.63–8.98 |
| 36 | 9.44 | 6.71–12.17 | 8.73 | 6.50–10.96 |
| 38–40 | 10.84 | 8.12–13.56 | 9.58 | 7.35–11.81 |
Importantly, dilated colon/rectum may not become apparent until the third trimester, even when obstruction is present earlier.
— Creasy & Resnik's Maternal-Fetal Medicine, Table 24-1
Sonographic Appearances & Differential Diagnosis
Key Pattern: Dilated Rectum with Echogenic Meconium
Imperforate anus / anorectal atresia is the most important cause:
- Produces a dilated rectum filled with echogenic meconium (meconium cannot exit → accumulates and becomes progressively echogenic)
- At 20 weeks: diameter of ≥1.3 cm (4.3 cm length) raises strong suspicion
- May appear as a V-shaped segment of dilated bowel measuring ~10 mm in diameter
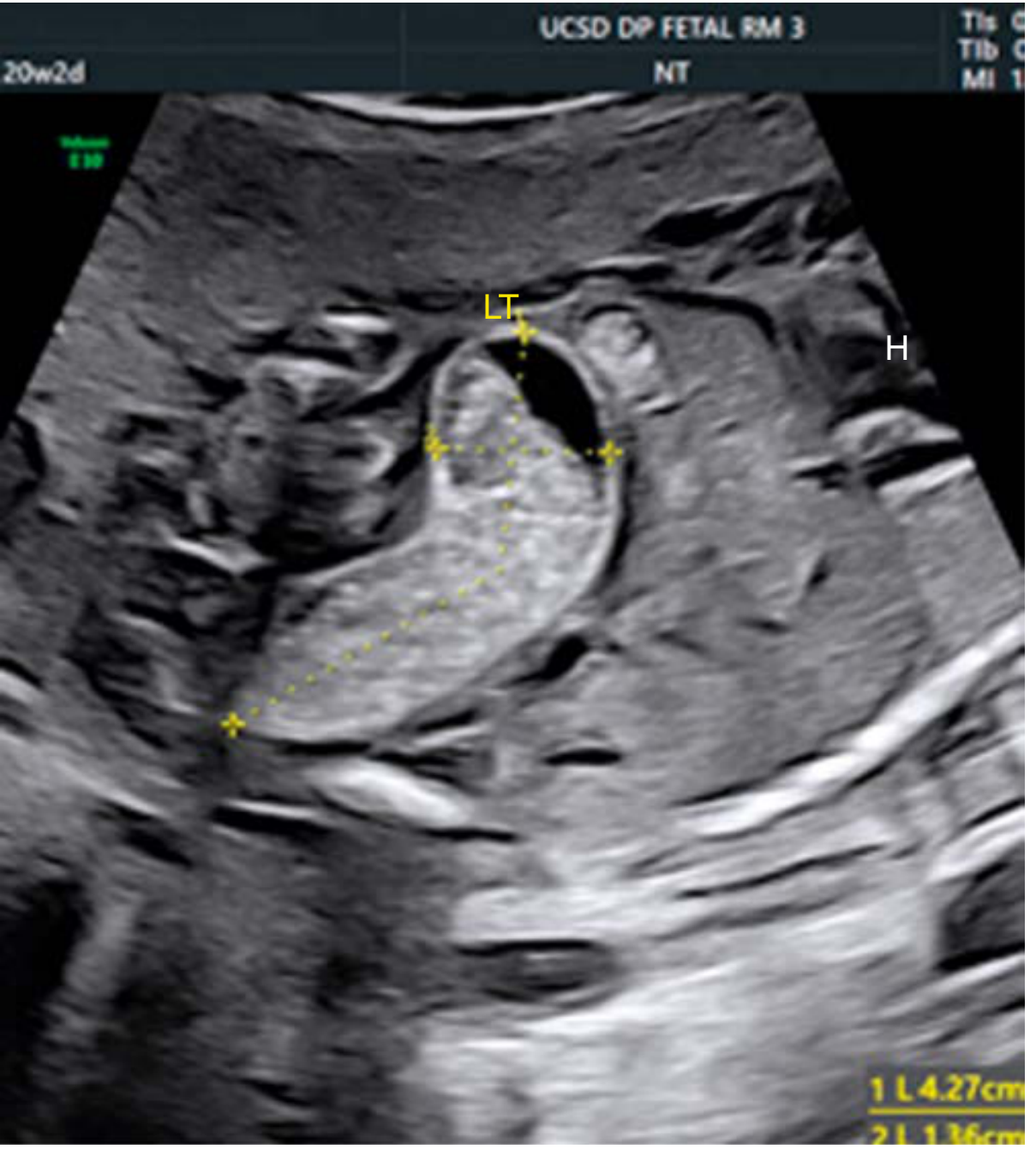
Fig. 24.15: Dilated rectum in a 20-week fetus with imperforate anus — echogenic meconium contents, 1.3 cm diameter, 4.3 cm length. — Creasy & Resnik's
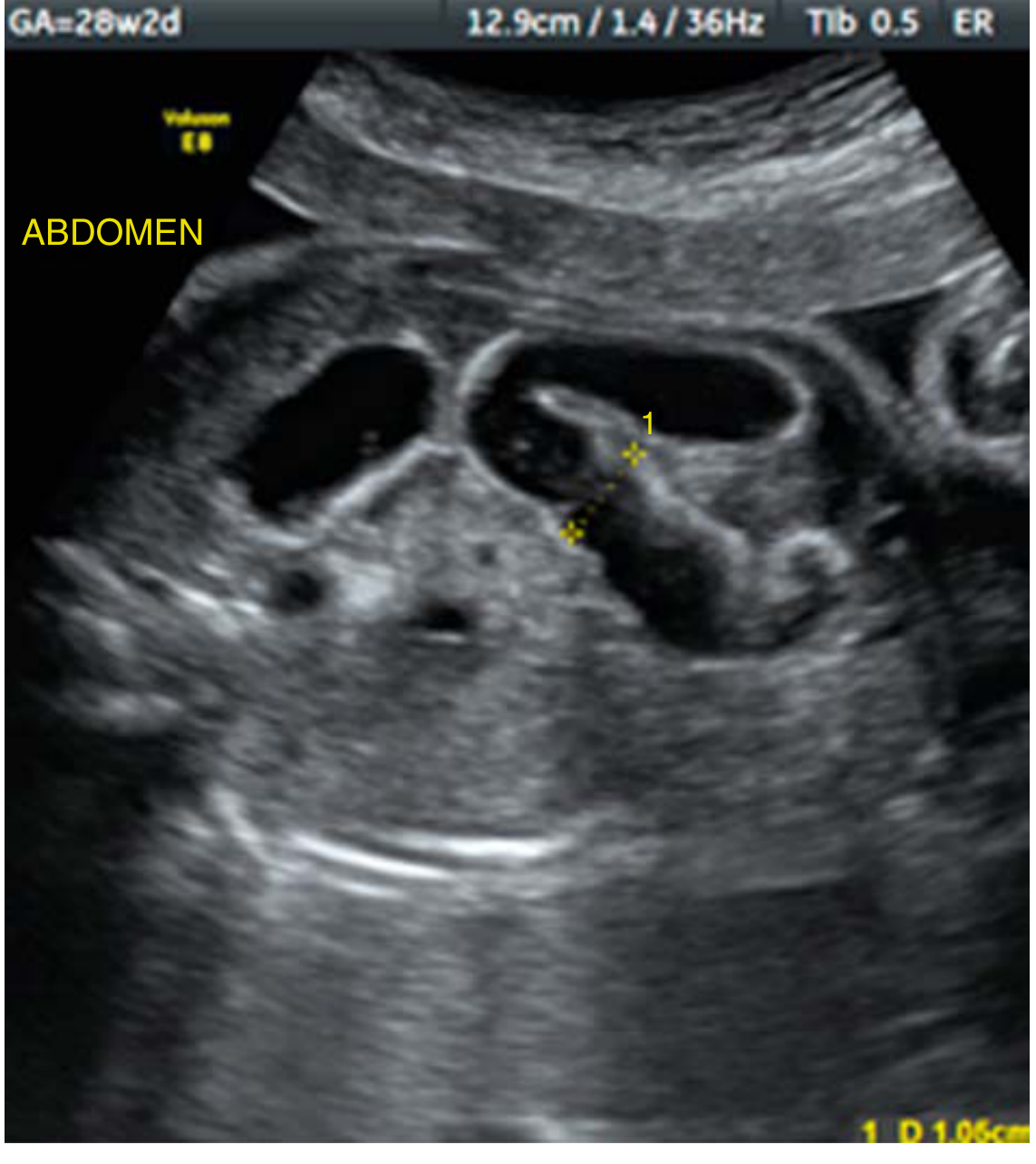
Fig. 24.14: V-shaped segment of dilated bowel measuring 10 mm in diameter, suggestive of anorectal atresia. — Creasy & Resnik's
Differential Diagnoses
When a dilated rectum is seen on anomaly scan, consider:
| Diagnosis | Key Features |
|---|---|
| Imperforate anus / anal atresia | Dilated rectum with echogenic meconium; most common cause |
| Anorectal atresia | V-shaped dilated bowel; echogenic contents |
| Cloacal anomaly / rectourinary fistula | Dilated colon with echogenic "bag of marbles" pattern; meconium in urinary tract |
| Hirschsprung disease | Aganglionosis of distal colon/rectum; may not be visible prenatally |
| Colonic atresia | More proximal distension; rectum may appear dilated secondarily |
| Meconium ileus (cystic fibrosis) | Echogenic bowel; multiple dilated loops |
| Meconium plug syndrome | Transient; may resolve postnatally |
| Mildly dilated normal colon | Within 95th centile for GA; no associated features |
| Intestinal malrotation | Variable appearance |
| Congenital chloride diarrhea | Rare; polyhydramnios |
| Mimics: hydrocolpos, ovarian/mesenteric/duplication cysts | Location, walls, no echogenic meconium contents |
Associated Anomalies to Search For
Anorectal malformations are strongly associated with several syndromes — a thorough anatomic survey is mandatory:
- VACTERL association: Vertebral defects, Anal atresia, Cardiac defect, Tracheo-Esophageal fistula, Renal agenesis, Limb defects
- VATER syndrome: Vertebral, imperforate Anus, Tracheo-Esophageal fistula, Renal defects
- OEIS complex: Omphalocele, Exstrophy of bladder, Imperforate anus, Spinal deformities
- Caudal regression syndrome
- Trisomy 21 (especially in duodenal atresia — present in ~30%)
- Congenital heart defects (ASD, VSD)
- Genitourinary anomalies, ventral wall defects, skeletal defects
Antenatal Management
Once a dilated rectum / lower bowel obstruction is suspected:
- Amniocentesis for chromosomal microarray ± NIPT — assess karyotype and cystic fibrosis gene status
- Fetal echocardiogram — cardiac defects common in VACTERL
- Targeted anatomic survey — spine, kidneys, limbs, sacrum
- Fetal MRI — can better define the level of obstruction and anatomy of the anorectal region
- Serial sonographic surveillance — monitor:
- Fetal growth
- Amniotic fluid (polyhydramnios risk with proximal obstruction)
- Progressive bowel distention
- Meconium peritonitis (bowel perforation)
- Third-trimester BPP / NST
- Pediatric surgery consultation antenatally
- Delivery at a tertiary centre — neonatal surgical team must be present
- Therapeutic amnioreduction if marked polyhydramnios threatens preterm labour
- Caesarean delivery only for obstetric indications (not indicated for bowel anomaly alone)
Prognosis
- Depends on level of obstruction and associated anomalies
- Isolated imperforate anus (low type): generally good prognosis with surgery
- Complex anorectal malformations with sacral agenesis or VACTERL: worse functional outcomes (continence, renal function)
- Survival for surgically repaired intestinal atresia has improved to 90–100% in modern series
- Long-term risk: short bowel syndrome (jejunoileal atresia), fecal continence issues (high anorectal malformations)
Bottom line: A dilated rectum on anomaly scan — especially containing echogenic meconium — is the hallmark sonographic sign of imperforate anus/anorectal atresia. It mandates a complete anatomic survey for VACTERL/OEIS features, fetal karyotyping, CF gene testing, fetal echo, and MRI for anatomical delineation. Delivery should be planned at a centre with neonatal surgery capability.
— Creasy & Resnik's Maternal-Fetal Medicine, Principles and Practice, Chapter 24
This is a shared conversation. Sign in to Orris to start your own chat.