43 day old male baby Incessant cry for past 5 days Baby given drops para Drops gastica Drops cpm Well for some time and again cries Doesn't crt during urination and ear clear Tenderness and guarding present on palpating abdomen B/L testes present inside scrotum Baby sent for USG abdomen
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Searching Images
intussusception ultrasound target sign bull's eye infant
Finding Sources
Loading Image
This is a classic clinical scenario. Let me now synthesize the full analysis.
Clinical Analysis: 43-Day-Old Male, Incessant Crying × 5 Days
The Critical Finding That Changes Everything
This is NOT simple infantile colic. The presence of abdominal tenderness and guarding is an organic red flag that demands urgent surgical evaluation.
Why This Is NOT Colic
Infantile colic (Wessel criteria: crying >3 hrs/day, >3 days/week, >3 weeks) is a diagnosis of exclusion. Per textbook criteria, organic causes must be ruled out first, especially:
- Abdominal tenderness and guarding → peritoneal irritation — never present in colic
- 5 days of incessant (not intermittent) crying — colic is intermittent, typically peaking in evening
- Age 43 days falls within the colic window (3 weeks–3 months), which can create diagnostic confusion
The drops given (paracetamol, simethicone/gastica, chlorphenamine) providing temporary relief then recurrence is consistent with an organic cause cycling through — not reassuring.
Top Differential Diagnoses
🔴 1. Intussusception (Most Urgent — Fits the Picture)
Classic triad: colicky abdominal pain + vomiting + bloody/currant-jelly stool
This baby's features matching intussusception:
- Intermittent severe crying (colicky pain) → baby is calm between episodes
- Abdominal tenderness and guarding ✓
- Male sex (3:2 male predominance) ✓
- Age 43 days — though peak is 5–12 months, neonatal/young infant intussusception occurs and is more often missed
On exam: a palpable mass in the right abdomen can be found in 80–90% of cases. Did you feel for a sausage-shaped mass in the RIF/RUQ?
USG findings to look for:
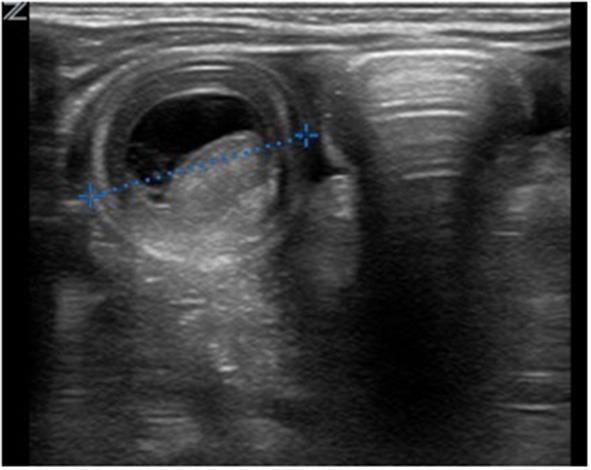
Target sign / bull's eye on USG — pathognomonic for intussusception
- Target sign (transverse): concentric rings (bowel-within-bowel)
- Pseudokidney sign (longitudinal): elongated layered mass
- Free fluid between layers suggests vascular compromise
🟠 2. Incarcerated Inguinal Hernia
- Testes confirmed bilateral in scrotum — but an indirect inguinal hernia can still be present without scrotal involvement
- At 43 days, indirect inguinal hernia incarceration is actually more common than intussusception at this age
- Check the inguinal canals bilaterally — a tender, irreducible lump in the groin?
- USG inguinal region should also be requested
🟡 3. Malrotation with Midgut Volvulus
- Can present in the first weeks of life with intermittent pain, bilious vomiting
- Guarding would indicate ischemia — surgical emergency
- USG: reversed SMA/SMV relationship; upper GI contrast is definitive
🟡 4. Meckel's Diverticulum Complication
- Lead point for intussusception in this age group
- Can cause obstruction or bleeding
🟢 5. Cow's Milk Protein Allergy / GERD
- Would NOT cause tenderness/guarding — these are peritoneal signs
- Less likely given the physical examination findings
What the USG Should Report
| Finding | What It Means |
|---|---|
| Target/Bull's eye sign | Intussusception |
| Pseudokidney sign | Intussusception |
| Dilated bowel loops + absent peristalsis | Obstruction |
| Free fluid/ascites | Peritonitis/ischemia |
| Hernial contents in inguinal canal | Incarcerated hernia |
| SMV to left of SMA | Malrotation |
Immediate Management
- Do NOT wait for USG results to act if the child deteriorates — get IV access now
- Keep NBM (nil by mouth)
- IV fluids for resuscitation
- Surgical team involvement — this baby needs a paediatric surgeon now
- If USG confirms intussusception without peritonitis: pneumatic/hydrostatic enema reduction (60–90% success, but time-dependent — efficacy drops after 24 hours of symptoms; this baby has had 5 days)
- At 5 days duration, operative reduction is more likely to be needed — success of enema reduction diminishes substantially after 24 hours of symptoms
- If peritonitis/perforation: direct to theatre without enema attempt
Bottom Line
Abdominal tenderness + guarding in a 43-day-old with incessant crying = surgical abdomen until proven otherwise.
The most dangerous diagnosis not to miss is intussusception/malrotation with volvulus. The USG is the right next step, but surgical consultation should happen simultaneously, not after the report.
Mulholland & Greenfield's Surgery, p. 5550–5553 | Swanson's Family Medicine Review, p. 535
This is a shared conversation. Sign in to Orris to start your own chat.