55 yr old male with Rt hypochondrial pain * 2 hrs, sense of passing feces, no vomiting diarhoea, fever, burning micturition, jaundice
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information to construct a thorough clinical analysis. Let me compose the full response.
Clinical Analysis: 55-Year-Old Male, Right Hypochondrial Pain x 2 Hours
Quick summary: The most likely diagnosis is biliary colic (or early acute cholecystitis), given the location, age, and absence of fever, jaundice, vomiting, or urinary symptoms. The "sense of passing feces" is a recognized visceral pain phenomenon in biliary disease. A structured differential is essential.
Searching sources... done.
1. Symptom Interpretation
| Feature | Clinical Relevance |
|---|---|
| RUQ pain x 2 hours | Classic biliary colic/cholecystitis territory |
| "Sense of passing feces" | Visceral referred sensation - common with gallbladder/colonic pathology |
| No fever | Argues against established acute cholecystitis or cholangitis |
| No jaundice | Common bile duct likely not obstructed - argues against choledocholithiasis or cholangitis |
| No vomiting/diarrhea | Less suggestive of gastroenteritis or pancreatitis |
| No burning micturition | Renal/ureteral cause less likely, though not excluded |
| 55-year-old male | Risk age for gallstones, hepatic pathology, colonic disease |
The "sense of passing feces" without actual diarrhea is a visceral pain phenomenon - patients with gallbladder or colonic pathology frequently report this because of the shared autonomic innervation between the biliary tree, hepatic flexure of the colon, and splanchnic nerves.
2. Top Differential Diagnoses
Priority 1 - Biliary Colic (Most Likely)
Uncomplicated biliary colic from cholelithiasis obstructing the cystic duct. Key features:
- RUQ or epigastric pain, typically dull and constant (not truly "colic"), lasting 1-5 hours
- Often postprandial (fatty meal trigger)
- Can radiate to right shoulder or back
- Murphy's sign usually negative (no gallbladder wall inflammation yet)
- Labs often normal
"In the absence of gallbladder wall inflammation, the pain is totally visceral and often dull, with a negative Murphy's sign during deep inspiration." - Yamada's Textbook of Gastroenterology
Priority 2 - Acute Cholecystitis (Must Rule Out)
2-hour duration is short for established cholecystitis, but the distinction is critical:
- Pain severe and constant, lasting >4-6 hours
- Murphy's sign positive (sensitivity 65-95%, specificity 30-87%)
- Leukocytosis in 52-63% of patients
- Fever and tachycardia
- In this patient - no fever yet, which is reassuring, but 2 hours is too early to exclude
"Cholecystitis is a clinical diagnosis. Even in cases with normal labs or equivocal imaging studies, history and examination consistent with cholecystitis should be treated as such." - Fischer's Mastery of Surgery
Priority 3 - Acute Biliary Pancreatitis
If a gallstone impacts at the ampulla of Vater:
- Steady, severe epigastric/RUQ pain radiating to the back
- Nausea/vomiting common (absent here, less likely)
- Serum lipase markedly elevated
- The absence of vomiting makes this less likely but serum lipase is mandatory
Priority 4 - Hepatic Pathology
- Hepatic abscess: gradual onset, usually fever present; less likely at 2 hours
- Hepatitis (viral/alcoholic): diffuse liver tenderness, elevated transaminases
- Hepatic mass/malignancy: insidious, not usually acute
Priority 5 - Colonic/Retroperitoneal
- Hepatic flexure colonic pathology (carcinoma, colitis): explains the "sense of passing feces"
- Retroperitoneal/right kidney: no burning micturition here, but ureteric colic can present with RUQ pain
- Right-sided diverticulitis (rare in Westerners, more common in Asians)
Priority 6 - Other to Consider
- Subphrenic pathology / right lower lobe pneumonia (referred diaphragmatic pain)
- Peptic ulcer disease (epigastric, not typically lateral)
- Myocardial ischemia - in a 55-year-old male, never forget this - atypical MI can present as RUQ/epigastric discomfort
3. Examination Priorities
On clinical examination, assess:
- Vital signs - fever (>38°C), tachycardia, hypotension (sepsis/shock)
- Murphy's Sign - examiner's hand in RUQ + deep inspiration; arrest of inspiration on palpation = positive
- Boas' sign - hyperesthesia below right scapula (cholecystitis)
- Rebound/guarding - suggests peritoneal involvement (perforation)
- Hepatomegaly/jaundice - look carefully even if patient denies
- Bowel sounds - ileus in pancreatitis
- Chest auscultation - right basal pneumonia
4. Investigations
Immediate (Bedside/Emergency)
| Investigation | Purpose |
|---|---|
| ECG | Exclude acute MI (mandatory in 55-year-old male) |
| Blood glucose, vitals | Emphysematous cholecystitis risk in diabetics |
Blood Tests
| Test | Rationale |
|---|---|
| FBC (CBC) | Leukocytosis in cholecystitis/cholangitis |
| LFTs (AST, ALT, ALP, GGT, bilirubin) | Biliary obstruction, hepatitis |
| Serum amylase + lipase | Exclude pancreatitis |
| Urea, creatinine, electrolytes | Baseline renal function |
| Urine analysis (dipstick + microscopy) | Renal/ureteric cause despite no dysuria |
| Blood cultures | If fever develops |
| CRP | Inflammatory marker |
Imaging
| Modality | Role |
|---|---|
| RUQ Ultrasound (First Line) | Gallstones (sensitivity ~100%), gallbladder wall thickening (>3 mm = cholecystitis), pericholecystic fluid, sonographic Murphy sign, CBD dilatation (>7 mm suggests choledocholithiasis), ascites |
| CT Abdomen (if USS equivocal) | Pericholecystic stranding, gallbladder fundus sign (sensitivity 75%, specificity >90%), emphysematous cholecystitis (gas in wall), hepatic abscess, colonic pathology |
| MRCP (if CBD involvement suspected) | Best for CBD stones, strictures |
| HIDA scan | If clinical/USS discordant; non-visualization = cystic duct obstruction (sensitivity 96%, specificity 90%) |
| Chest X-ray | Right basal pneumonia, pneumoperitoneum |
5. Tokyo Guidelines Severity Grading (if Cholecystitis Confirmed)
(Current Surgical Therapy, 14e)
| Grade | Definition |
|---|---|
| I (Mild) | No organ dysfunction; symptoms <72 hrs; cholecystectomy is low risk |
| II (Moderate) | WBC >18,000/mm³; palpable tender RUQ mass; symptoms >72 hrs; marked local inflammation (gangrenous cholecystitis, pericholecystic abscess, emphysematous cholecystitis) |
| III (Severe) | Organ dysfunction: circulatory failure, neurological disturbance, respiratory failure (PaO2/FiO2 <300), renal failure (creatinine >2.0 mg/dL), hepatic failure (INR >1.5), thrombocytopenia (<100,000/mm³) |
6. Management Algorithm
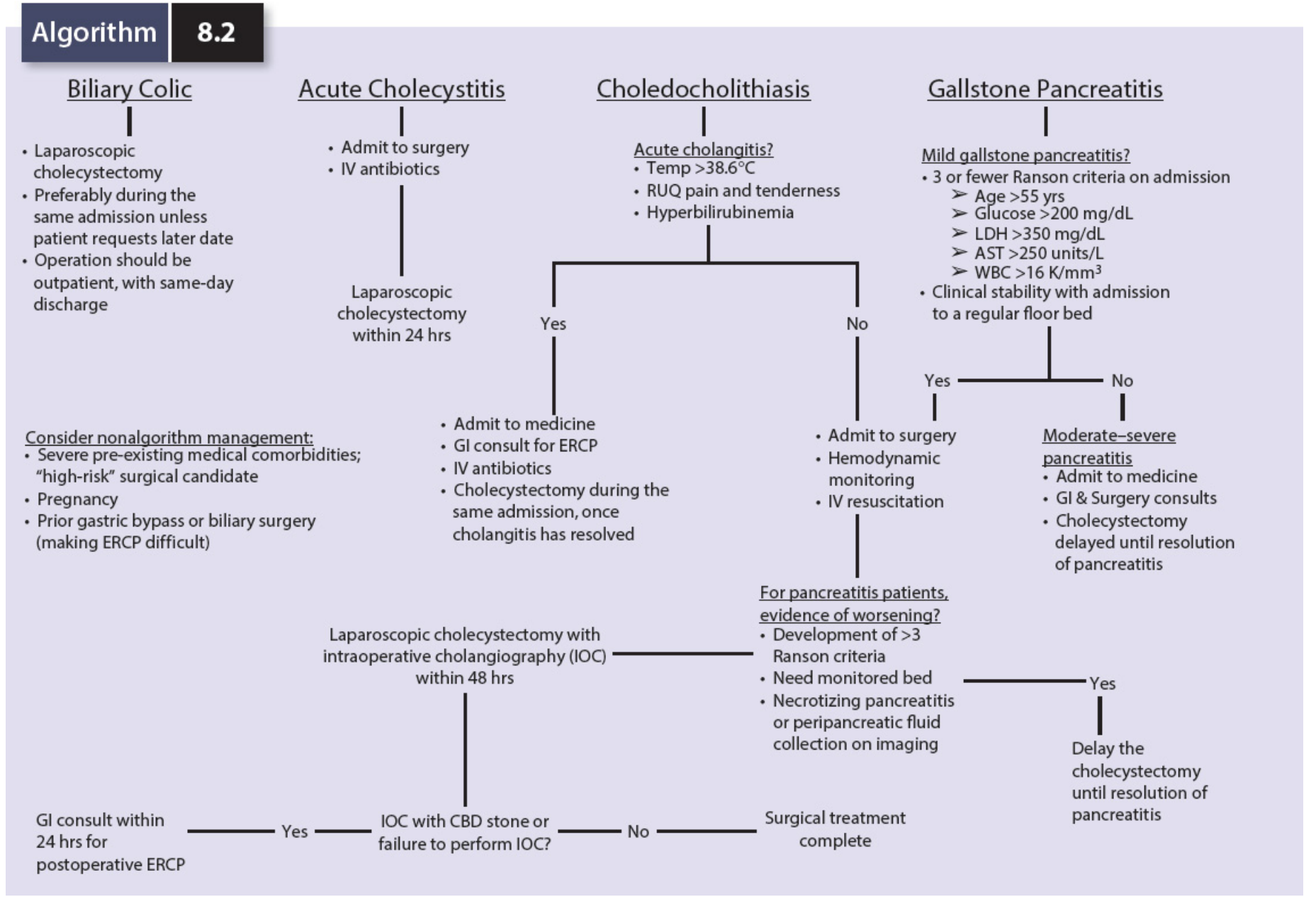
Algorithm 8.2 - Biliary infections and management (Mulholland & Greenfield's Surgery, 7e)
If Biliary Colic (uncomplicated):
- Analgesia (NSAIDs first-line, opioids if needed)
- NBM initially; IV fluids
- Elective laparoscopic cholecystectomy - preferably same admission
- Outpatient follow-up if discharged
If Acute Cholecystitis:
- Admit to surgery
- IV fluids + electrolyte correction
- IV antibiotics: cover gram-negative enteric bacilli (E. coli, Klebsiella, Enterobacter), gram-positive (Enterococcus), anaerobes (~15%)
- Suitable regimens: piperacillin-tazobactam, cefuroxime + metronidazole, or ampicillin-sulbactam
- Laparoscopic cholecystectomy within 24-48 hours (early surgery is now standard of care)
- If Grade II/III or high surgical risk - percutaneous cholecystostomy tube as bridge
If Choledocholithiasis/Cholangitis (Charcot's Triad = jaundice + fever + RUQ pain):
- GI consult for ERCP
- IV antibiotics + cholecystectomy after cholangitis resolves
If Gallstone Pancreatitis:
- Conservative management + cholecystectomy delayed until pancreatitis resolves (unless mild)
7. Red Flags Requiring Urgent Escalation
- Development of fever - suggests progression to acute cholecystitis or cholangitis
- Jaundice appearing - CBD obstruction, cholangitis (Charcot's triad/Reynolds pentad)
- Hypotension - septic shock from cholangitis or perforation
- Peritoneal signs (guarding, rigidity, rebound) - perforation
- ECG changes / chest pain radiation - don't miss inferior MI presenting as RUQ pain
Bottom Line: At 2 hours with no fever, no jaundice, and no vomiting, this patient most likely has biliary colic from cholelithiasis. However, acute cholecystitis, biliary pancreatitis, and atypical MI must be actively excluded with ECG, labs (FBC, LFTs, lipase), and RUQ ultrasound. If USS confirms gallstones with wall thickening or sonographic Murphy sign, treat as Grade I cholecystitis and proceed to early laparoscopic cholecystectomy.
Sources: Mulholland & Greenfield's Surgery 7e; Fischer's Mastery of Surgery 8e; Yamada's Textbook of Gastroenterology 7e; Current Surgical Therapy 14e; Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.