Mechanism of action of torsemide and spironolacfone in reducing swelling
Reading File
Finding Sources
Finding Sources
Searching PubMed
torsemide spironolactone edema mechanism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have everything needed to write a complete, well-sourced answer.
Mechanism of Action of Torsemide and Spironolactone in Reducing Swelling (Edema)
Edema results from excess fluid accumulating in the interstitial space, usually driven by sodium and water retention. Both torsemide and spironolactone reduce edema by promoting urinary sodium (and therefore water) excretion, but they act at completely different sites in the nephron.
1. Torsemide - Loop Diuretic
Target Site
The thick ascending limb (TAL) of the loop of Henle.
Molecular Target: NKCC2 Cotransporter
Torsemide, like all loop diuretics (furosemide, bumetanide, ethacrynic acid), selectively blocks the Na⁺/K⁺/2Cl⁻ cotransporter type 2 (NKCC2) located on the luminal (apical) membrane of TAL cells. This transporter normally moves 1 Na⁺, 1 K⁺, and 2 Cl⁻ ions together from the tubular lumen into the cell.
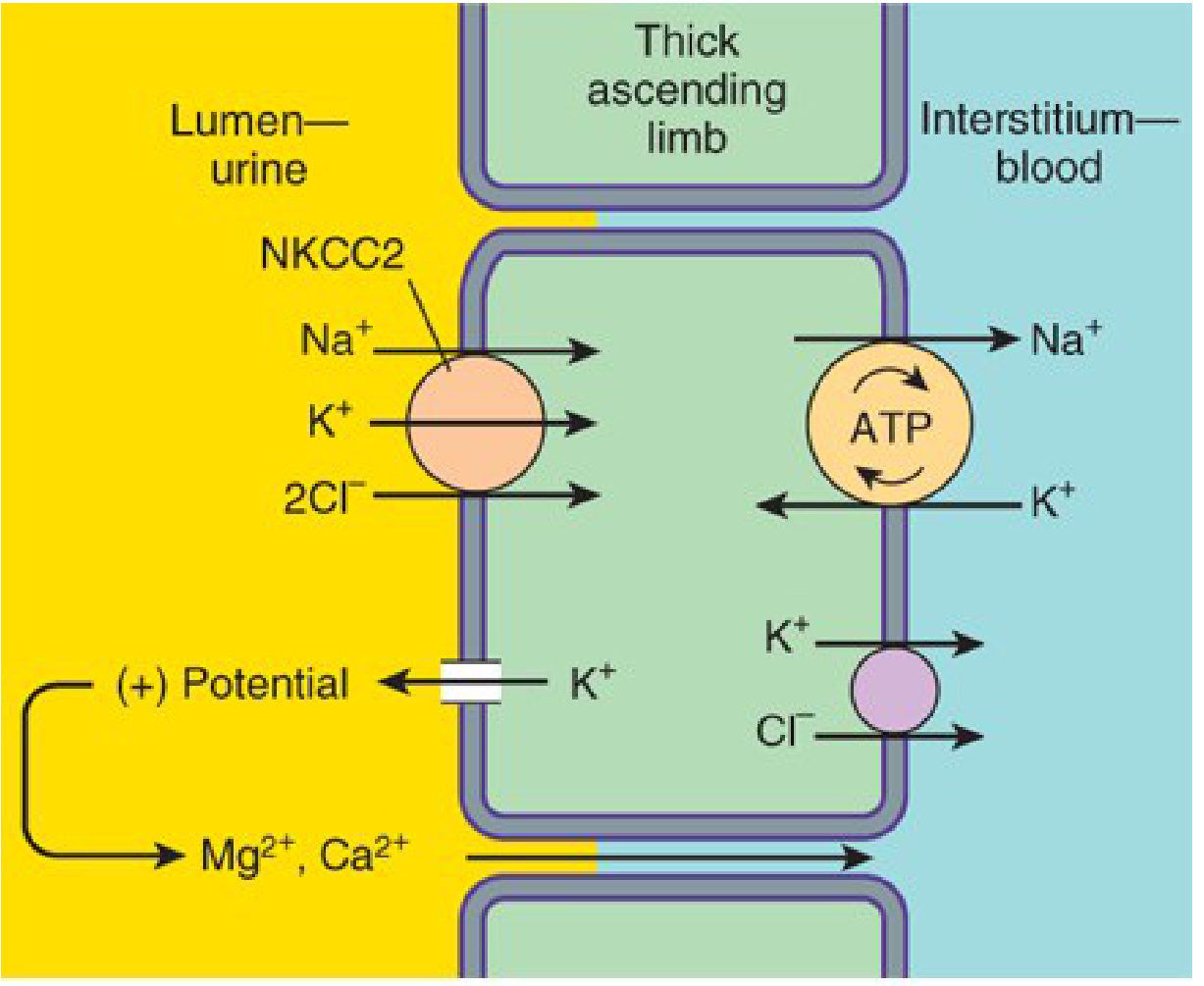
Thick ascending limb ion transport - Katzung's Basic and Clinical Pharmacology, 16th Ed.
How Blocking NKCC2 Reduces Swelling
-
Reduced NaCl reabsorption - The TAL normally reabsorbs ~25-30% of filtered NaCl. When torsemide blocks NKCC2, this reabsorption is prevented. This is the largest single-segment contribution to sodium reabsorption, which is why loop diuretics are the most potent diuretics available.
-
Reduced medullary hypertonicity - The TAL builds up the concentrated medullary interstitium that drives water reabsorption in downstream segments. When NKCC2 is blocked, medullary osmolality falls, so less water is passively extracted from the descending limb and collecting duct.
-
Massive natriuresis → osmotic water loss - The excess NaCl reaching the collecting duct draws water with it into the urine by osmosis, producing copious, dilute urine.
-
Reduced plasma volume - The net result is reduced circulating volume and decreased capillary hydrostatic pressure, which reverses the Starling forces driving fluid into the interstitium, shrinking the edema.
Why Torsemide Over Furosemide?
- Oral bioavailability of torsemide is ~80-100% vs. ~50% (and highly variable) for furosemide.
- Torsemide is mainly eliminated hepatically (not renally), so its absorption is more predictable in heart failure patients who often have gut edema.
- Its longer duration of action (half-life ~3-4 hrs vs. ~1.5 hrs for furosemide) reduces "post-diuretic sodium retention," making it preferred for chronic heart failure and CKD. (Brenner and Rector's The Kidney; Katzung's, 16th Ed.)
Dose-Response Pattern
Loop diuretics show a sigmoidal ("S"-shaped) dose-response curve: below the threshold, no effect; above the ceiling, no additional diuresis regardless of dose. Clinicians must identify the effective threshold dose, then adjust frequency rather than dose to modulate total daily diuresis. (Lippincott Illustrated Reviews: Pharmacology)
2. Spironolactone - Aldosterone Antagonist (Potassium-Sparing Diuretic)
Target Site
The collecting tubule (cortical collecting duct).
Molecular Target: Mineralocorticoid (Aldosterone) Receptor
Spironolactone is a synthetic steroid that competitively antagonizes the aldosterone (mineralocorticoid) receptor. Here is the step-by-step mechanism:
-
Normal aldosterone action: Aldosterone enters collecting duct principal cells, binds its cytoplasmic mineralocorticoid receptor, and the receptor-hormone complex translocates into the nucleus. There it transcribes genes that produce:
- Apical ENaC (epithelial Na⁺ channels) - increase sodium entry from lumen
- Basolateral Na⁺/K⁺-ATPase - pump Na⁺ into blood, draw K⁺ in
- This creates a lumen-negative electrical gradient that drives K⁺ and H⁺ secretion into urine.
-
Spironolactone blocks the receptor: By occupying the aldosterone receptor, spironolactone prevents the receptor complex from translocating to the nucleus, so the stimulatory proteins (ENaC, Na⁺/K⁺-ATPase) are not produced.
-
Result: Na⁺ is NOT reabsorbed in the collecting duct, and K⁺/H⁺ are NOT secreted. This produces mild natriuresis and diuresis while sparing potassium (hence "K⁺-sparing" diuretic). (Lippincott Illustrated Reviews: Pharmacology, p. 343)
How This Reduces Swelling
| Mechanism | Effect on Edema |
|---|---|
| Blocks aldosterone-driven Na⁺ retention | Less sodium (and water) retained in body |
| Reduces plasma volume | Lower capillary hydrostatic pressure |
| Anti-fibrotic cardiac/vascular effects | Reduces aldosterone-driven tissue remodeling that worsens edema in heart failure |
| Blocks aldosterone-induced endothelial dysfunction | Improves vascular tone, reduces capillary leak |
Key Clinical Contexts for Spironolactone in Edema
- Cirrhotic ascites - Ascites results from portal hypertension AND secondary hyperaldosteronism (the kidney retains sodium because it "thinks" volume is low). Spironolactone directly counters the hyperaldosteronism, making it the drug of choice for cirrhotic ascites (100 mg/day, often combined with furosemide at 40 mg/day in a 2.5:1 ratio). (Frameworks for Internal Medicine; Goldman-Cecil Medicine)
- Heart failure with reduced EF - At lower doses (25-50 mg/day), spironolactone reduces morbidity and mortality by blocking the direct myocardial fibrotic and pro-arrhythmic effects of aldosterone.
- Nephrotic syndrome - Less effective here because aldosterone levels are not consistently elevated.
- Idiopathic edema - Can be used, though sodium restriction alone is preferred when possible. (Katzung's, 16th Ed.)
Comparison Table: Torsemide vs. Spironolactone
| Feature | Torsemide | Spironolactone |
|---|---|---|
| Drug class | Loop diuretic | Aldosterone antagonist (K⁺-sparing) |
| Site of action | Thick ascending limb (TAL) | Collecting tubule |
| Molecular target | NKCC2 cotransporter (blocked) | Mineralocorticoid receptor (blocked) |
| Potency | Very high (25-30% NaCl reabsorption blocked) | Mild (only ~2% NaCl load at this segment) |
| Effect on K⁺ | Hypokalemia (K⁺ wasted) | Hyperkalemia (K⁺ spared) |
| Onset of action | Rapid (1-2 hrs oral) | Slow (2-3 days; requires new protein synthesis) |
| Best edema type | Acute decompensated HF, pulmonary edema, renal edema | Cirrhotic ascites, chronic HF, hyperaldosteronism |
| Unique advantage | Highest diuretic efficacy; works even in poor renal function | Counters RAAS-driven sodium retention; anti-fibrotic |
Why They Are Often Combined
Torsemide + spironolactone is a classic pairing because:
- Complementary sites - Together they block two separate sodium reabsorption segments.
- Potassium balance - Torsemide causes hypokalemia; spironolactone causes hyperkalemia. Together they tend to normalize serum K⁺.
- RAAS counteraction - Torsemide activates the RAAS as a compensatory response (volume depletion → renin → angiotensin II → aldosterone → sodium reabsorption). Spironolactone directly blocks this aldosterone-driven counter-response.
Sources: Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th Ed.; Brenner and Rector's The Kidney; Frameworks for Internal Medicine; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.