Small cell cancer of lung from robbin
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I have all the content needed. Here is the complete Robbins-based overview of Small Cell Lung Carcinoma:
Small Cell Lung Carcinoma (SCLC) - Robbins & Kumar Basic Pathology
Overview & Epidemiology
SCLC is classified under neuroendocrine carcinomas in the 2021 WHO classification of malignant epithelial lung tumors. It has the strongest association with smoking among all lung cancer subtypes. It accounts for roughly 15% of lung carcinomas. The peak incidence is in the 50s-60s, and more than 50% of patients already have distant metastases at diagnosis.
- Robbins & Kumar Basic Pathology, p. 485
Pathogenesis & Molecular Features
SCLC arises from neuroendocrine cells (Kulchitsky cells) of the bronchial epithelium. Its molecular landscape is dominated by loss-of-function mutations rather than activating oncogene mutations:
| Molecular Alteration | SCLC | NSCLC |
|---|---|---|
| 3p deletions | ~90% | ~80% |
| RB mutations | ~90% | ~20% |
| TP53 mutations | ~90% | ~50% |
| p16/CDKN2A mutations | ~10% | ~50% |
| KRAS mutations | Rare | ~30% (adenocarcinoma) |
| EGFR mutations | Absent | ~20% (adenocarcinoma) |
| ALK fusions | Absent | 4-6% (adenocarcinoma) |
Key points:
- The near-universal loss of RB (retinoblastoma gene) allows unrestrained cell cycle progression.
- 3p deletions are the most common chromosomal abnormality in lung cancer overall, but especially pronounced in SCLC.
- EGFR and ALK mutations - the major targetable alterations in NSCLC - are absent in SCLC, explaining the lack of targeted therapy options.
Morphology
Gross
- Typically arises as a central (hilar/perihilar) mass, often near the main bronchi.
- Usually a pale gray-white tumor that can encase and compress major bronchi.
- Often shows extensive necrosis.
Microscopic (Fig. 11.44F)
- Small cells (~2x the size of a lymphocyte) with scant cytoplasm
- Small, hyperchromatic nuclei with fine ("salt-and-pepper") chromatin pattern
- Indistinct or absent nucleoli
- Cells grow in diffuse sheets - no glandular or squamous architecture
- Prominent areas of necrosis (top left in the image)
- Azzopardi effect - basophilic encrustation of vascular walls by DNA from necrotic tumor cells (pathognomonic)
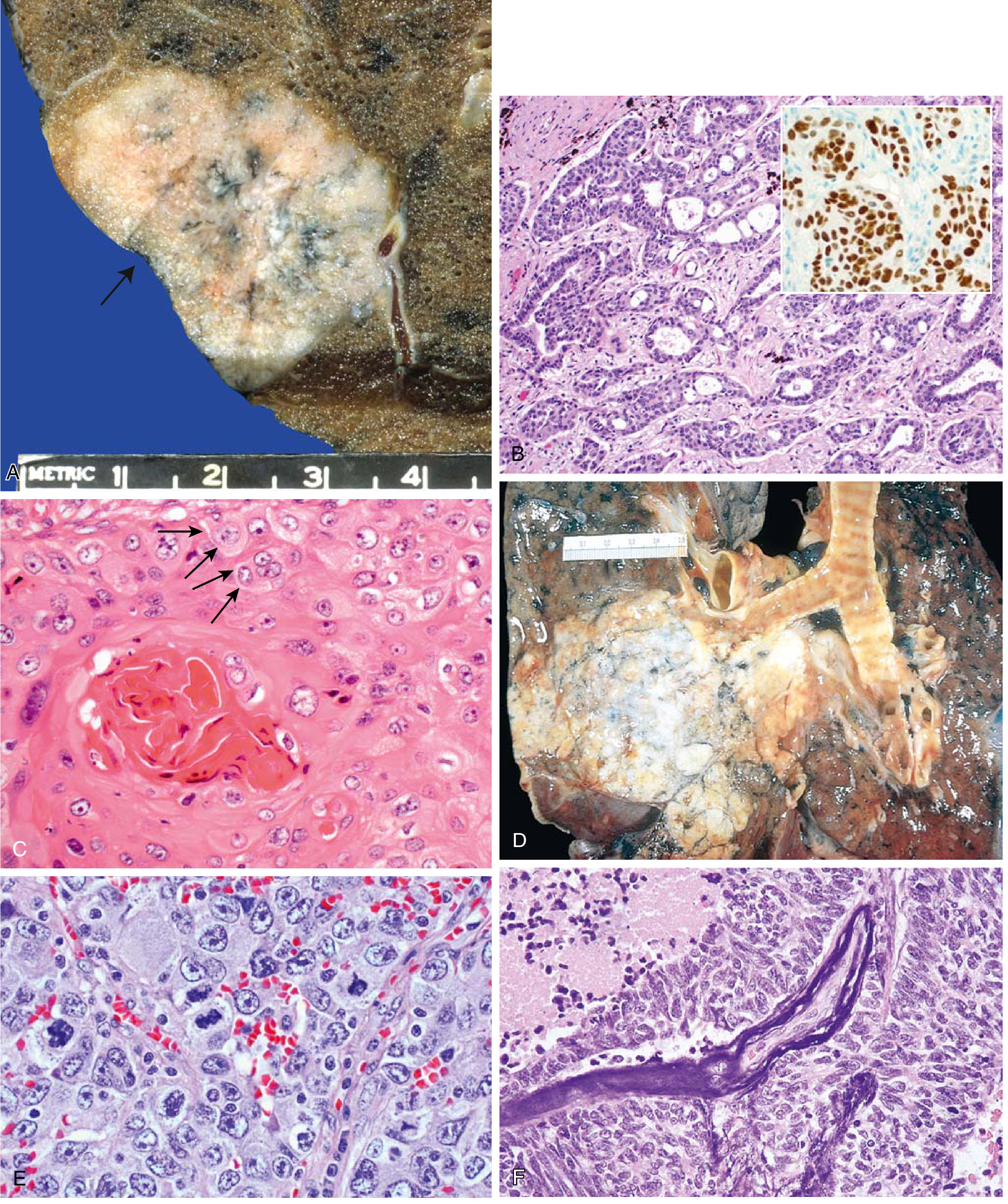
(Panel F, bottom right, shows SCLC; Panel E shows large cell carcinoma for comparison)
Immunohistochemistry / Neuroendocrine Markers
SCLC expresses both neuroendocrine and epithelial markers:
| Marker | SCLC | NSCLC |
|---|---|---|
| Chromogranin | + | - |
| Synaptophysin | + | - |
| CD56 (NCAM) | + | - |
| Dense-core granules (EM) | + | - |
| Epithelial membrane antigen (EMA) | + | + |
| Carcinoembryonic antigen (CEA) | + | + |
| Cytokeratin (dot-like pattern) | + | + |
| Mucin | Absent | Present (adenocarcinoma) |
Peptide Hormone Production & Paraneoplastic Syndromes
SCLC is the prototype for paraneoplastic syndromes due to its neuroendocrine origin and ectopic hormone secretion:
| Hormone Produced | Clinical Syndrome |
|---|---|
| ACTH | Cushing syndrome (ectopic) |
| ADH | SIADH - hyponatremia |
| Gastrin-releasing peptide (GRP/bombesin) | Growth factor / autocrine stimulation |
| Calcitonin | Hypocalcemia (rare) |
Other neurologic paraneoplastic syndromes (Lambert-Eaton myasthenic syndrome, encephalomyelitis) are most characteristic of SCLC among all lung tumor types.
Hypercalcemia is most often seen with squamous cell carcinoma (via PTH-rP), hematologic syndromes with adenocarcinoma, and neurologic syndromes with small cell carcinoma. - Robbins, p. 488
Spread & Staging
- Virtually always widely disseminated at diagnosis, even when the primary tumor appears small and localized.
- Spreads to mediastinal and hilar lymph nodes, then to liver, brain, bone, and adrenal glands.
- May cause SVC syndrome by compressing the superior vena cava.
- Can extend into pleural and pericardial spaces causing effusions.
Clinical Features & Prognosis
- SCLC is not surgically resectable - metastatic spread is invariable even at early apparent stages.
- Very sensitive to chemotherapy and radiotherapy - often a complete initial response.
- However, it invariably recurs - response is not durable.
- No targeted therapies available (no EGFR/ALK mutations).
- Unresponsive to immune checkpoint inhibitors despite having a very high mutation burden.
- Median survival with treatment: ~1 year
- 5-year survival: only ~5%
"Small cell carcinoma has invariably spread by the time it is detected, even when the primary tumor is small and appears to be localized. Thus, surgical resection is not curative... The median survival with treatment is only 1 year and only 5% of patients are alive at 10 years." - Robbins & Kumar Basic Pathology, p. 487
SCLC vs. NSCLC - Summary Comparison (Table 11.6)
| Feature | SCLC | NSCLC |
|---|---|---|
| Cell size | Small, scant cytoplasm | Large, abundant cytoplasm |
| Nuclei | Hyperchromatic, fine chromatin, indistinct nucleoli | Pleomorphic, coarse chromatin, prominent nucleoli |
| Architecture | Diffuse sheets | Glandular or squamous |
| Neuroendocrine markers | Present | Absent |
| Mucin | Absent | Present (adenocarcinoma) |
| RB mutations | ~90% | ~20% |
| EGFR/ALK | Absent | Present (subset) |
| Response to chemo/RT | Often complete but invariably recurs | Incomplete |
| Response to checkpoint inhibitors | Unresponsive | Responsive |
| Surgery | Not curative | Potentially curative (early stage) |
Neuroendocrine Spectrum (Robbins)
Robbins describes pulmonary neuroendocrine tumors as a continuum of increasing aggressiveness:
Typical carcinoid → Atypical carcinoid → Large cell neuroendocrine carcinoma → Small cell carcinoma (most aggressive)
- Robbins & Kumar Basic Pathology, p. 489
This is a shared conversation. Sign in to Orris to start your own chat.