Give detail about dka,it's diagnostic criteria, it's sign and symptoms,it's management, how to check recovery , answer all the questions thos can be arose
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive DKA response. Let me compile the full detailed answer.
Diabetic Ketoacidosis (DKA) - Complete Clinical Guide
1. DEFINITION & OVERVIEW
DKA is an acute, life-threatening metabolic emergency defined by a triad of:
- Hyperglycemia ("D" - diabetes/elevated glucose)
- Ketosis ("K" - urinary ketones ≥2+ or β-hydroxybutyrate ≥3.0 mmol/L)
- Metabolic Acidosis ("A" - arterial or venous pH < 7.3)
It results from absolute or relative insulin deficiency combined with excess of counter-regulatory hormones (glucagon, cortisol, catecholamines, growth hormone).
- Goldman-Cecil Medicine, p. 2484
2. PATHOPHYSIOLOGY
The flowchart below illustrates the three parallel mechanisms that converge to produce DKA:
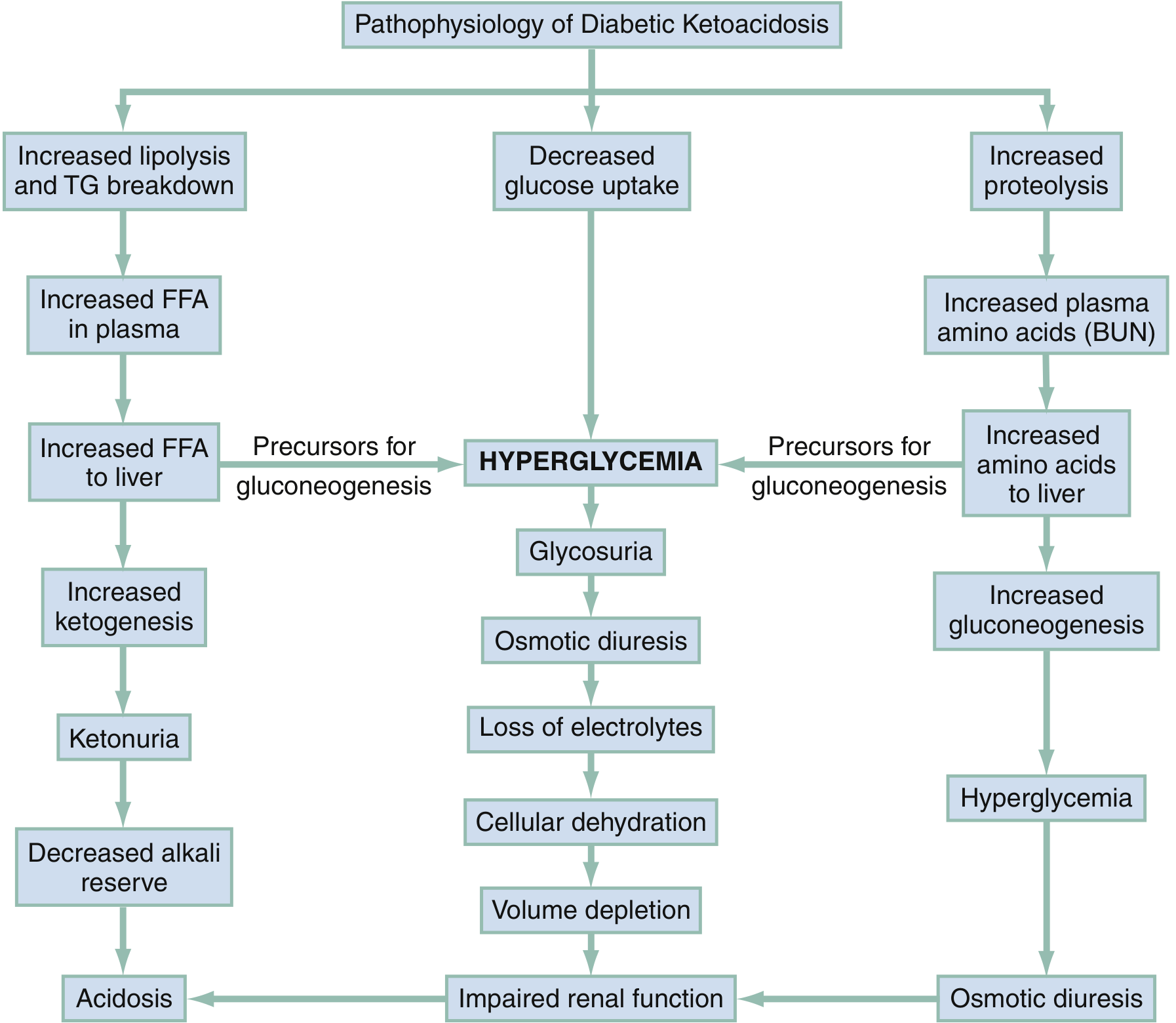
Three key pathways:
A. Lipolysis Pathway (left column)
- Insulin deficiency → increased lipolysis and triglyceride breakdown
- Elevated free fatty acids (FFA) flood the liver
- Liver converts FFA to ketone bodies (β-hydroxybutyrate, acetoacetate, acetone)
- Ketone bodies accumulate → ketonuria → decreased alkali reserve → Acidosis
B. Hyperglycemia Pathway (center)
- Decreased glucose uptake by peripheral cells
- Glycosuria → osmotic diuresis → massive loss of water, Na⁺, K⁺, Mg²⁺, Ca²⁺, PO₄³⁻
- Cellular dehydration → volume depletion → impaired renal function (worsens acidosis)
C. Proteolysis Pathway (right column)
- Muscle breakdown releases amino acids to liver
- Liver uses amino acids for gluconeogenesis → more hyperglycemia → more osmotic diuresis
The net result: profound dehydration (fluid deficit 3-5 L in adults), electrolyte imbalances, and anion gap metabolic acidosis.
- Rosen's Emergency Medicine, p. 2540-2543
3. PRECIPITATING FACTORS
| Most Common | Other Precipitants |
|---|---|
| Infections (pneumonia, UTI, sepsis) | Cerebrovascular accident |
| Inadequate insulin / nonadherence | Acute pulmonary embolism |
| New-onset diabetes (~25% of cases) | Acute pancreatitis |
| Acute coronary syndrome | Alcohol intoxication |
| Unknown | Cushing syndrome, thyrotoxicosis, acromegaly |
| Drugs: corticosteroids, clozapine, olanzapine, cocaine, SGLT2 inhibitors, thiazides |
Key point: ~25% of all DKA episodes occur in patients with previously undiagnosed diabetes.
- Goldman-Cecil Medicine, p. 2483; Rosen's Emergency Medicine, p. 2543
4. SIGNS & SYMPTOMS
History / Symptoms
| Symptom | Mechanism |
|---|---|
| Polyuria | Osmotic diuresis from glycosuria |
| Polydipsia | Compensatory response to fluid loss |
| Polyphagia (early) | Cells starved of glucose |
| Nausea, vomiting | Acidosis + gastric dysmotility |
| Abdominal pain | In 50% of patients (especially children); may mimic acute abdomen; usually idiopathic, resolves with treatment. In adults - always investigate for a real abdominal trigger. |
| Weakness, lethargy | Dehydration + metabolic derangement |
| Weight loss | Fluid loss + catabolism |
| Visual blurring | Hyperosmolarity affecting lens |
| Gradual onset | Hours to days of deterioration |
Physical Examination Findings
| Finding | Mechanism |
|---|---|
| Kussmaul breathing (deep, rapid respirations) | Respiratory compensation for metabolic acidosis; attempt to blow off CO₂ |
| Fruity/acetone odor on breath | Exhaled acetone (a ketone body) |
| Tachycardia | Dehydration + compensatory response |
| Hypotension / orthostatic changes | Volume depletion |
| Dry skin and mucous membranes | Dehydration |
| Reduced jugular venous pressure | Hypovolemia |
| Depressed mental status / coma | Hyperosmolarity + acidosis; correlates with severity |
| Elevated temperature | Rarely from DKA itself - suggests underlying infection |
| Tachypnea | Respiratory compensation |
Remember: Fever is NOT a feature of DKA itself. Its presence strongly suggests an infectious precipitant.
- Rosen's Emergency Medicine, p. 2541; Goldman-Cecil Medicine, p. 2484
5. DIAGNOSTIC CRITERIA
ADA Classification of DKA Severity
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Blood Glucose | >250 mg/dL | >250 mg/dL | >250 mg/dL |
| Arterial pH | 7.25 - 7.30 | 7.00 - 7.24 | < 7.00 |
| Serum HCO₃⁻ | 15 - 18 mEq/L | 10 - 14 mEq/L | < 10 mEq/L |
| Urine Ketones | Positive | Positive | Positive |
| Serum Ketones | Positive | Positive | Positive |
| Anion Gap | > 10 | > 12 | > 12 |
| Mental Status | Alert | Alert/Drowsy | Stupor/Coma |
The Three Fundamental Features (Goldman-Cecil Criteria)
- Hyperglycemia OR history of diabetes
- Urinary ketones ≥ 2+ OR β-hydroxybutyrate ≥ 3.0 mmol/L
- Arterial or venous pH < 7.3, serum HCO₃⁻ < 18 mEq/L
Typical Lab Values in DKA vs HHS
| Lab Test | DKA | HHS |
|---|---|---|
| Glucose (mg/dL) | >350 | >700 |
| Sodium (mEq/L) | Low 130s | 140s |
| Potassium (mEq/L) | ~4.5-6.0 (initially) | ~5 |
| Bicarbonate (mEq/L) | <10 | >15 |
| BUN (mg/dL) | 25-50 | >50 |
| Serum Ketones | Present | Absent |
- Rosen's Emergency Medicine, p. 2543; Goldman-Cecil Medicine, p. 2484
Important Electrolyte Nuances
- Potassium: May appear normal or even HIGH initially (due to acidosis driving K⁺ extracellularly), but total body K⁺ is always depleted. Will drop precipitously once insulin is given.
- Sodium: Measured sodium is falsely LOW due to osmotic dilution; corrected Na = measured Na + 1.6 × [(glucose - 100) / 100]
- WBC: Elevated even without infection (due to metabolic acidosis itself); not reliable for diagnosing infection
- Anion Gap: AG = Na⁺ - (Cl⁻ + HCO₃⁻); normal 8-12 mEq/L; in DKA typically elevated
Acid-Base Analysis Tools
- Winter's formula: Expected PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2 → confirms appropriate respiratory compensation
- Delta gap: (Delta AG - Delta HCO₃⁻) > +6 = coexisting metabolic alkalosis; < -6 = coexisting hyperchloremic acidosis
Note on Euglycemic DKA
Blood glucose can be ≤ 300 mg/dL ("euglycemic DKA") in up to 18% of cases - seen especially with SGLT2 inhibitor use, pregnancy, or fasting. Do not exclude DKA based on "normal" glucose alone.
6. MANAGEMENT
Step-by-step approach: Fluids → Electrolytes → Insulin → Treat Precipitant
A. FLUID REPLACEMENT
- Adults typically have a 3-5 L fluid deficit
- If in hypovolemic shock: 0.9% NS bolus as fast as possible (adults); or 20 mL/kg boluses in children until systolic BP ≥ 80 mmHg
- Standard initial rate: 1 L/hr of 0.9% NS or Lactated Ringer's (LR) for first 1-2 hours
- After initial resuscitation: Switch to 0.45% NS at 250-500 mL/hr
- When glucose drops to ≤ 250-300 mg/dL: Switch IV fluid to D5W/0.45% NS to prevent hypoglycemia while continuing insulin to clear ketones
Avoid overhydration - risk of pulmonary edema and cerebral edema (especially in children)
B. INSULIN THERAPY
- Do NOT start insulin until potassium is confirmed ≥ 3.5 mEq/L (risk of fatal hypokalemia)
- Dose: 0.1 units/kg/hr Regular insulin IV (no bolus needed in most guidelines)
- Continue insulin infusion until DKA resolution criteria are met
- Do NOT stop insulin when glucose normalizes - continue until ketoacidosis is cleared
- Switch to subcutaneous insulin 1-2 hours before stopping IV infusion (to prevent rebound)
C. POTASSIUM REPLACEMENT
| Serum K⁺ | Action |
|---|---|
| < 3.5 mEq/L | Hold insulin; give K⁺ 20-40 mEq/hr until ≥ 3.5, THEN start insulin |
| 3.5 - 5.5 mEq/L | Give K⁺ 20-30 mEq/L in IV fluids; start insulin |
| > 5.5 mEq/L | Hold K⁺; check every 2 hours |
D. PHOSPHATE REPLACEMENT
- Total body phosphate depleted due to osmotic diuresis
- Routine replacement not clearly beneficial; consider if serum PO₄ < 1.0 mg/dL, respiratory distress, hemolytic anemia, or cardiac dysfunction
E. MAGNESIUM REPLACEMENT
- Common in DKA; can worsen hypokalemia and hypocalcemia, cause cardiac dysrhythmia
- Dose: 1-3 g MgSO₄ IV if deficient
F. SODIUM BICARBONATE - NOT routinely recommended
- Previously used for pH < 7.0, but research shows worse outcomes with bicarbonate:
- Worsens hypokalemia
- Delays clearance of ketosis
- Paradoxical CSF acidosis (CO₂ crosses blood-brain barrier more freely than HCO₃⁻)
- Exacerbates cerebral edema
- Exception: May use in imminent cardiac arrest; pre-intubation in severely acidemic patients (to prevent cardiovascular collapse)
G. TREATING THE PRECIPITANT
- Cultures, antibiotics if infection suspected
- ECG, troponin if ACS suspected
- Do not dismiss abdominal pain as DKA-related in adults
H. MONITORING (Flow Sheet)
Monitor every 1-2 hours:
- Vital signs, urine output
- Blood glucose
- Serum K⁺, Na⁺, Cl⁻, HCO₃⁻, pH
- Insulin infusion rate
- Fluid intake/output balance
I. INTUBATION NOTE
- Avoid intubation in DKA when possible - patients have tremendous respiratory drive compensating for acidosis; matching that minute ventilation on a ventilator is very challenging
- If intubation required (comatose, vomiting): maintain hyperventilation on vent; use pre-intubation bicarbonate bolus to prevent cardiovascular collapse from acute pH drop
7. CRITERIA FOR DKA RESOLUTION (Recovery Monitoring)
DKA is considered resolved when ALL THREE of the following are met:
| Criterion | Target |
|---|---|
| Blood glucose | < 200-250 mg/dL |
| Serum bicarbonate | ≥ 18 mEq/L |
| Venous pH | ≥ 7.30 |
| (Anion gap normalized) | < 12 mEq/L |
Critical Note: Glucose normalizes BEFORE ketoacidosis resolves. Never stop insulin early just because glucose is normal. Always add dextrose to IV fluids instead and continue insulin until all three criteria above are met.
β-Hydroxybutyrate as Recovery Marker
Serial β-hydroxybutyrate measurement provides the best tool to monitor ketosis resolution. It is more reliable than urine ketones in the presence of a coexisting acid-base abnormality. As DKA resolves, β-hydroxybutyrate converts to acetoacetate - which can falsely make urine ketone strips appear "worse" during recovery.
Transition to Subcutaneous Insulin
- Patient must be able to tolerate oral fluids before switching
- Overlap IV insulin with subcutaneous injection by 1-2 hours before stopping the infusion
- Choose subcutaneous insulin regimen based on whether patient has known vs new-onset diabetes
8. COMPLICATIONS OF DKA
| Complication | Details |
|---|---|
| Cerebral edema | Most feared; occurs 6-10 hours after therapy starts; 90% mortality; mainly in children < 5 years; treat with mannitol |
| Hypokalemia | Iatrogenic if inadequate K⁺ replacement; can cause fatal arrhythmia |
| Hypoglycemia | Inadequate glucose monitoring; failure to add dextrose when glucose < 250-300 mg/dL |
| Pulmonary edema | Overaggressive fluid resuscitation |
| Metabolic alkalosis | Overaggressive bicarbonate administration |
| Aspiration pneumonia | In obtunded/vomiting patients |
| Arterial thrombosis | Hypercoagulable state from dehydration and hyperosmolarity |
| Infection | Leading cause of death; especially pneumonia |
9. DIFFERENTIAL DIAGNOSIS
| Condition | Key Distinguishing Feature |
|---|---|
| Alcoholic ketoacidosis | Euglycemic or hypoglycemic; alkalemia more common; recent alcohol cessation |
| Starvation ketosis | Mild; glucose normal/low; no acidosis |
| HHS (Hyperosmolar Hyperglycemic State) | Glucose >700, HCO₃⁻ >15, no significant ketones; Type 2 DM; older patients |
| Lactic acidosis | High lactate; no ketonemia |
| Uremic acidosis | High creatinine; ketonemia absent |
| Salicylate poisoning | Mixed AG metabolic acidosis + respiratory alkalosis |
| Acute abdomen | In adults with DKA and abdominal pain - must rule out true surgical abdomen |
10. SPECIAL POPULATIONS
Pregnancy
- DKA can occur at lower blood glucose levels (as low as 200 mg/dL)
- Higher risk due to insulin resistance of pregnancy
- All pregnant DKA patients: admit to ICU + consult endocrinologist + high-risk obstetrician
Children
- ~50% present with abdominal pain (usually resolves with treatment)
- Cerebral edema far more common in young children (< 5 years)
- Outpatient management possible only if: initial pH ≥ 7.35, HCO₃⁻ ≥ 20 mEq/L, tolerating oral fluids, symptoms resolving, no precipitant requiring hospitalization
New-Onset Diabetes
- 25% of all DKA; need diabetes education, supplies training, insulin titration planning
11. PROGNOSIS & PREVENTION
- Treated DKA mortality: ~4-5% overall; primary causes of death are infection, arterial thrombosis, and shock
- Mortality is higher in: extremes of age, severe precipitating illness, delayed presentation
Prevention (Sick-Day Rules)
-
Frequent blood glucose monitoring during illness
-
Never omit insulin during illness even if not eating
-
Check urine/serum ketones when glucose > 250
-
Drink small frequent carbohydrate-containing fluids
-
Early medical contact if unable to manage at home
-
Hospital admission after DKA: see diabetes educator before discharge
-
Goldman-Cecil Medicine, p. 2485; Rosen's Emergency Medicine, p. 2541-2545
QUICK REFERENCE SUMMARY
DKA TRIAD: Glucose >250 + Ketones + pH <7.3 / HCO₃⁻ <18
MANAGEMENT SEQUENCE:
1. IV Fluids → 0.9% NS 1L/hr (shock: bolus 20mL/kg)
2. Check K⁺ → if <3.5, replace FIRST before insulin
3. Insulin → 0.1 units/kg/hr Regular IV
4. When glucose <250-300 → Add D5W to prevent hypoglycemia
5. Replace K⁺, Mg²⁺, PO₄ as needed
6. Find and treat precipitant
7. Monitor q1-2h: glucose, pH, HCO₃⁻, electrolytes
RESOLUTION CRITERIA (all three):
✓ Glucose <250
✓ pH ≥7.30
✓ HCO₃⁻ ≥18 mEq/L
This is a shared conversation. Sign in to Orris to start your own chat.