Using millers anaesthesia and Morgan anaesthesia books teach me from basics to advance with easy to read and understand format about Pulmonary function tests
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I now have rich, comprehensive content from both Miller's and Morgan's textbooks. Let me compile the complete, well-structured educational guide.
Pulmonary Function Tests (PFTs) - A Complete Guide
From Basics to Advanced Anaesthetic Applications
Sources: Miller's Anesthesia 10e & Morgan and Mikhail's Clinical Anesthesiology 7e
📘 PART 1: WHY PFTs MATTER IN ANAESTHESIA
Postoperative pulmonary complications (PPCs) are among the most common sources of perioperative morbidity and healthcare cost after major surgery. A thorough history and physical exam remain the cornerstone of preoperative pulmonary assessment - but PFTs add critical objective data when:
- The patient has known lung disease (COPD, asthma, ILD)
- Surgery involves the thorax (lung resection especially)
- There are unexplained symptoms - dyspnoea, exercise intolerance
- ICU/critical care decision-making is needed
"In patients with known risk factors, preexisting lung diseases, and thoracic surgery candidates, pulmonary function tests complement preoperative evaluation and risk stratification." - Miller's Anesthesia 10e
📘 PART 2: LUNG VOLUMES - THE FOUNDATION
Before understanding PFTs, you must know lung volumes. This is the map of the respiratory system:
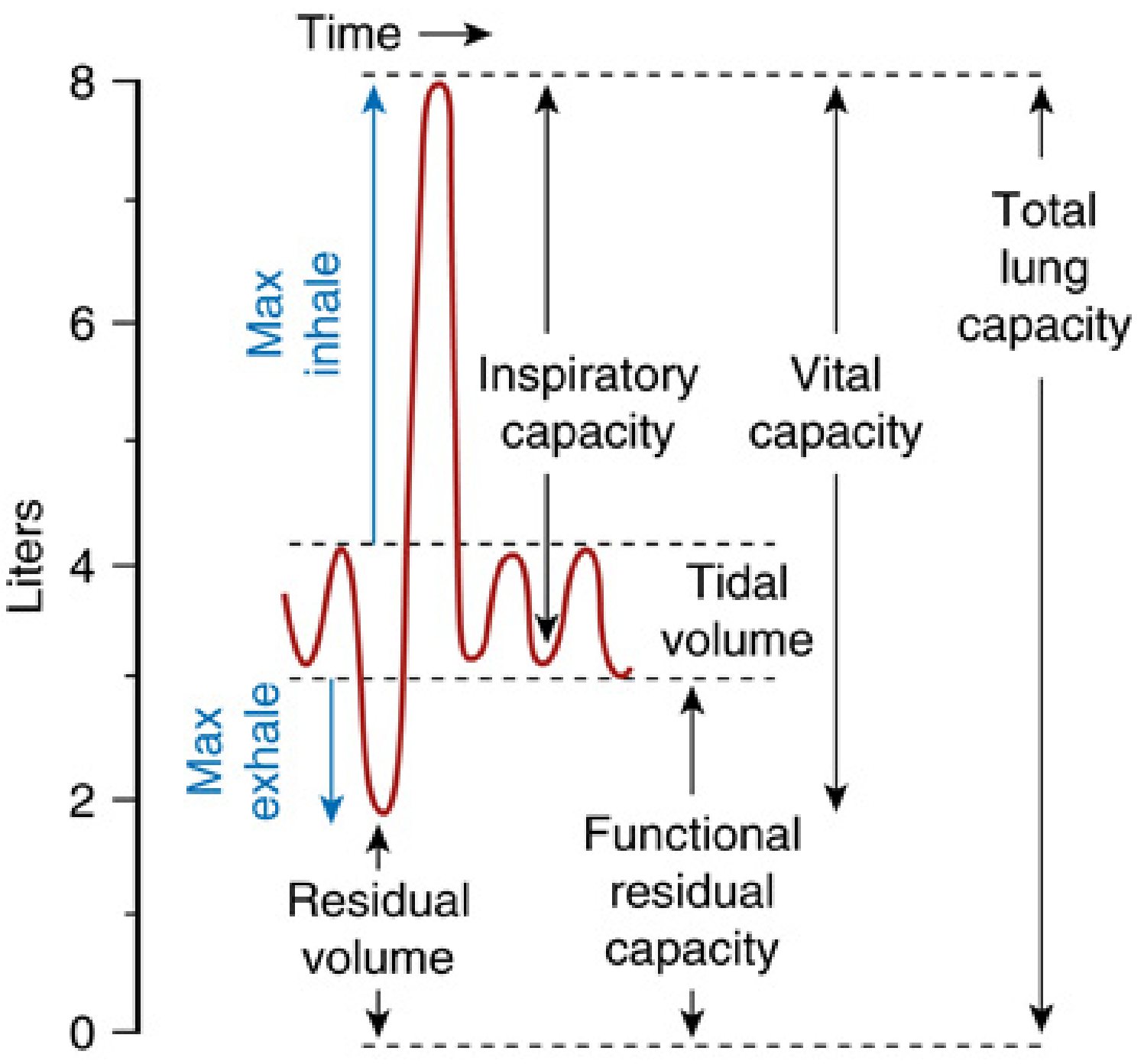
Fig. 12.23 - Lung Volumes (Miller's Anesthesia 10e, p.1306)
| Volume/Capacity | Definition | Normal Value |
|---|---|---|
| Tidal Volume (VT) | Air moved in/out with each normal breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Extra air you can inhale beyond VT | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Extra air you can exhale beyond VT | ~1100 mL |
| Residual Volume (RV) | Air remaining after maximal exhalation - cannot be measured by spirometry | ~1200 mL |
| Total Lung Capacity (TLC) | All air in the lungs at maximum inspiration | ~6000 mL |
| Vital Capacity (VC) | Maximum volume exhaled after maximum inhalation | ~4800 mL |
| Functional Residual Capacity (FRC) | Volume remaining after normal exhalation (= ERV + RV) | ~2300 mL |
| Inspiratory Capacity (IC) | Maximum air inhaled from FRC | ~3500 mL |
The Special Importance of FRC
Morgan's (Ch. 23) describes FRC beautifully: "The lung volume at the end of a normal exhalation is called functional residual capacity. At this volume, the inward elastic recoil of the lung approximates the outward elastic recoil of the chest wall - thus defining the point from which normal breathing takes place."
Factors that REDUCE FRC (important for anaesthetists!):
- Obesity - reduced chest wall compliance + increased abdominal pressure on diaphragm
- Female sex - ~10% lower than males
- Supine position - abdominal contents push up against diaphragm (greatest change 0° to 60°)
- Laparoscopy/Pregnancy/Ascites - increased intraabdominal pressure
- Restrictive lung disease - reduced lung/chest wall compliance
FRC and General Anaesthesia
Miller's (p.1308-1309) highlights a critical point every anaesthetist must know:
"Resting lung volume (FRC) is reduced by almost 1 L by moving from upright to supine position; induction of anesthesia further decreases the FRC by approximately 0.5 L. This reduces the FRC from approximately 3.5 L to 2 L, a value close to RV."
This ~20% fall in FRC under general anaesthesia (whether IV or inhalational, controlled or spontaneous) is a major cause of intraoperative hypoxaemia - because it promotes airway closure and atelectasis.
📘 PART 3: SPIROMETRY - THE WORKHORSE TEST
Spirometry is the single most important and commonly used PFT. It is the preferred diagnostic test for both COPD and asthma.
How It Is Performed
- Patient inhales to Total Lung Capacity (TLC)
- Exhales as forcefully and completely as possible into the spirometer
- Measurements are taken from the volume-time curve
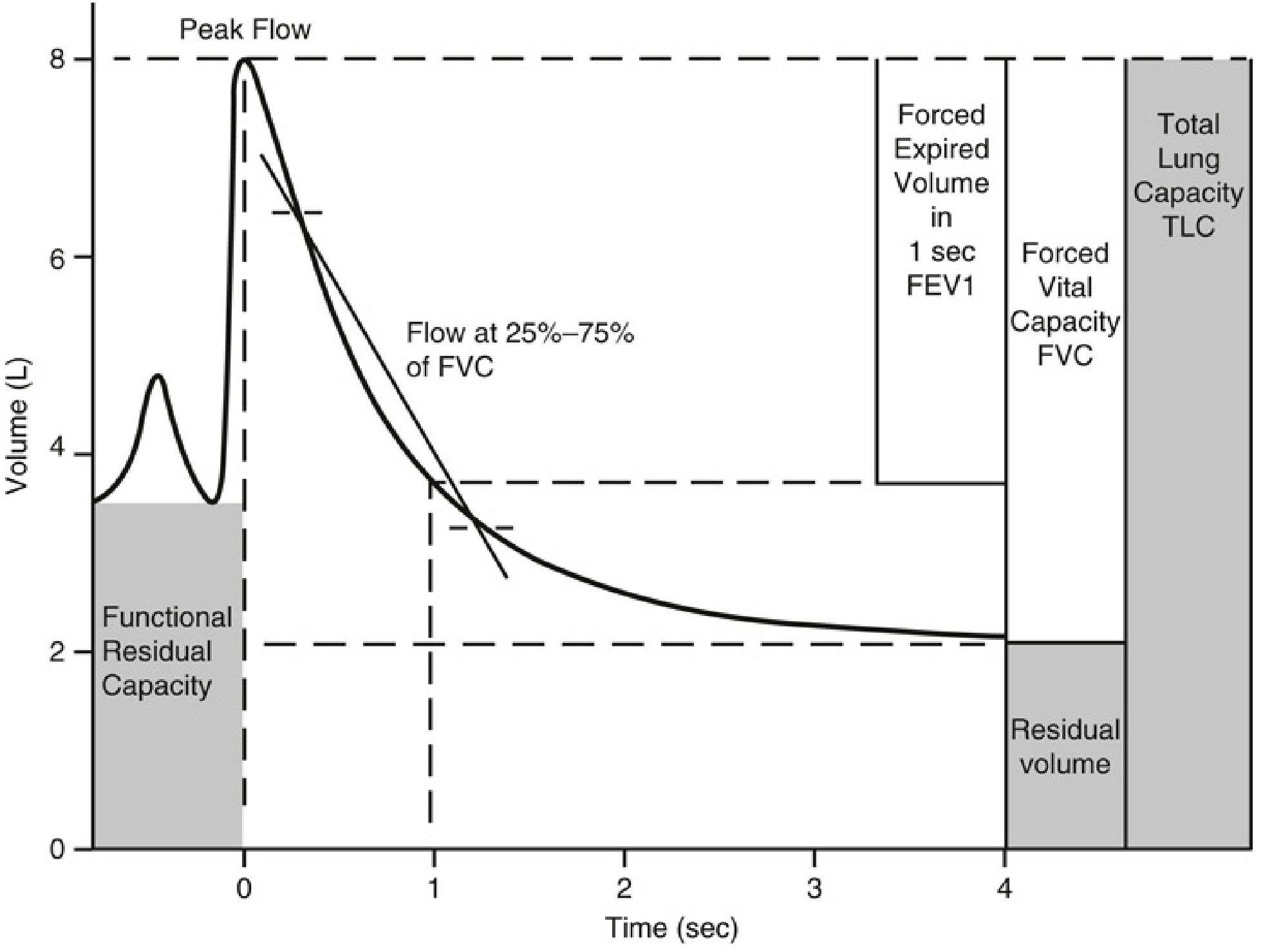
Fig. 12.21 - Spirometry Tracing (Miller's Anesthesia 10e, p.1305) - Note: shaded areas (FRC and RV) cannot be measured by spirometry alone.
Key Spirometry Parameters
| Parameter | Definition | Significance |
|---|---|---|
| FVC (Forced Vital Capacity) | Total volume exhaled forcefully | Reduced in both obstruction AND restriction |
| FEV₁ (Forced Expiratory Volume in 1 sec) | Volume exhaled in the first second | Most important single value |
| FEV₁/FVC ratio | Proportion of FVC exhaled in 1 second | KEY ratio to distinguish obstruction vs restriction |
| FEF 25-75% | Mean flow during middle half of FVC | Sensitive indicator of small airway disease |
| Peak Expiratory Flow (PEF) | Maximum flow rate during forced expiration | Used for asthma monitoring |
Interpreting Spirometry - The Golden Rules
STEP 1: Look at FEV₁/FVC ratio
- < 0.70 (post-bronchodilator) = OBSTRUCTIVE pattern
- ≥ 0.70 with reduced FVC = RESTRICTIVE pattern (confirm with lung volumes)
STEP 2: If Obstructive - grade severity by FEV₁ % predicted:
- FEV₁ ≥ 80% → Mild (GOLD 1)
- FEV₁ 50-79% → Moderate (GOLD 2)
- FEV₁ 30-49% → Severe (GOLD 3)
- FEV₁ < 30% → Very Severe (GOLD 4)
STEP 3: Check bronchodilator reversibility
- Improvement in FEV₁ > 12% AND > 200 mL = reversible = suggests ASTHMA
- No significant reversibility = COPD
📘 PART 4: OBSTRUCTIVE vs RESTRICTIVE PATTERNS
Obstructive Pattern (e.g., COPD, Asthma)
- FEV₁/FVC < 0.70
- FEV₁ reduced
- FVC may be normal or reduced
- TLC increased (air trapping/hyperinflation)
- RV increased
Miller's (p.3823-3826): "A diagnosis of COPD is determined by spirometry with FEV₁/FVC ratio <0.7 post-bronchodilator (confirming non-reversibility of airway obstruction)."
For Asthma: Miller's (p.3945) - "Typical findings are a reduction in FEV₁/FVC - with a ratio below 0.7 indicative of airflow obstruction. Importantly, normal initial PFT results do not necessarily exclude asthma." In this case, a methacholine challenge test or trial of bronchodilator therapy should be performed.
Restrictive Pattern (e.g., Pulmonary Fibrosis, Obesity, NMD)
- FEV₁/FVC preserved (≥ 0.70)
- FVC reduced
- TLC reduced (confirmed by full lung volume testing)
- Both FEV₁ and FVC proportionally reduced
📘 PART 5: FLOW-VOLUME LOOPS - READING THE CURVE
The flow-volume loop plots flow (y-axis) against volume (x-axis) and gives information that a simple time-volume curve cannot.
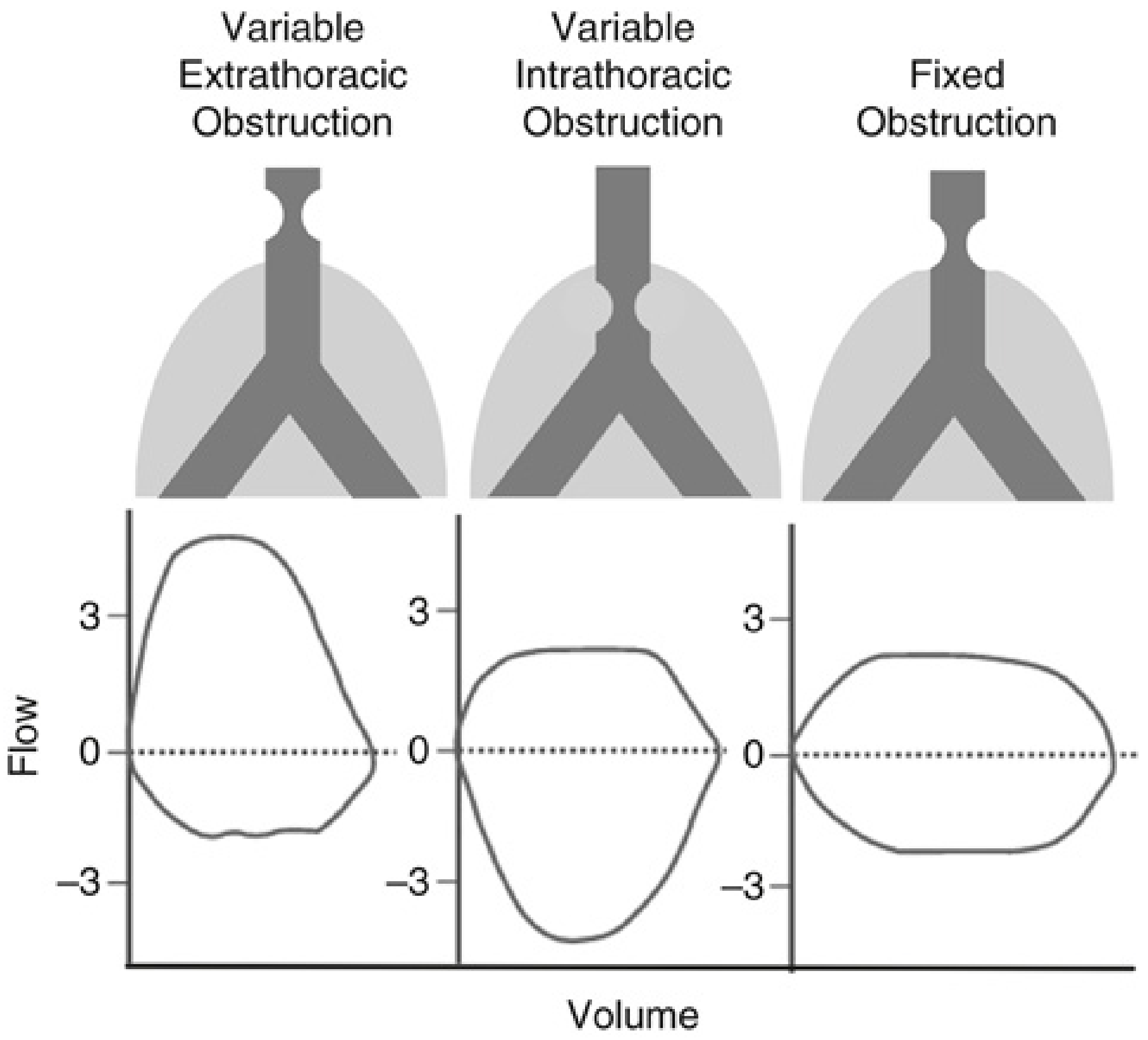
Fig. 12.22 - Flow-Volume Loop Patterns (Miller's Anesthesia 10e, p.1305)
| Pattern | Inspiratory Limb | Expiratory Limb | Cause |
|---|---|---|---|
| Variable Extrathoracic | Flattened (truncated) | Normal | Vocal cord dysfunction, tracheal stenosis above thoracic inlet |
| Variable Intrathoracic | Normal | Flattened | Tracheomalacia, intrathoracic tracheal mass |
| Fixed Obstruction | Flattened both | Flattened both | Rigid tracheal stenosis (e.g., post-intubation) |
| Obstructive (COPD/Asthma) | Normal | Scooped-out/concave shape | Small airway collapse on expiration |
| Restrictive | Normal shape, smaller loop | Normal shape, smaller loop | Reduced lung volume |
Anaesthetic pearl: A flattened inspiratory limb suggests a difficult airway or tracheal pathology - important pre-induction consideration!
📘 PART 6: LUNG VOLUME MEASUREMENT
RV and FRC cannot be measured by spirometry alone. Three methods exist:
1. Body Plethysmography (Most Accurate)
- Patient sits in airtight, constant-volume "body box"
- Makes inspiratory efforts against a closed shutter
- Applies Boyle's Law: P₁V₁ = P₂V₂
- As thoracic volume expands, box pressure rises - allowing calculation of FRC/RV
- Most accurate - includes all gas (even trapped/non-communicating areas)
2. Nitrogen Washout
- Patient breathes 100% oxygen
- Nitrogen is washed out of lungs and measured in exhaled air
- N₂ = 80% of lung gas - so total lung gas = measured N₂ volume ÷ 0.80
- Limitation: underestimates in patients with poorly-communicating lung units (emphysema, bullae)
3. Helium Dilution
- Based on conservation of mass of inert helium gas
- Limitation: same as nitrogen washout - misses poorly-communicating zones
Clinical tip: In emphysema with bullae, there can be a large discrepancy between plethysmography (larger, more accurate) and helium dilution (underestimates) - this discrepancy itself is diagnostically useful. (Miller's block20)
📘 PART 7: DIFFUSING CAPACITY (DLCO)
What Is DLCO?
DLCO (Diffusing Capacity for Carbon Monoxide) measures the functional capillary surface area available for gas exchange.
Miller's (p.1303-1304) explains the principle: "Because of the high affinity of CO for haemoglobin, the partial pressure of dissolved CO in the blood remains very low, so CO transfer is not limited by pulmonary blood flow, but only by membrane thickness."
What DLCO Tells You
DLCO is governed by:
- Surface area of the alveolar-capillary membrane
- Thickness of the membrane (inverse relationship)
- Pressure gradient across the membrane
- Solubility of the gas
| DLCO Result | Interpretation | Common Causes |
|---|---|---|
| Reduced | Emphysema, ILD/Fibrosis, Pulmonary HTN, Anaemia | Gas exchange surface lost or membrane thickened |
| Normal | Simple airways disease (asthma) | Membrane intact |
| Elevated | Pulmonary haemorrhage, Polycythaemia, Exercise | Increased RBC available for CO binding |
DLCO Anaesthetic Thresholds (Miller's p.1304)
- DLCO < 60% of predicted - associated with increased risk of postoperative pulmonary complications and is an indication for further preoperative risk assessment using exercise testing
- DLCO (ppoDLCO) < 30-40% predicted - threshold for increased risk in thoracic surgery
📘 PART 8: CLOSING CAPACITY - A UNIQUE ANAESTHETIC CONCEPT
Morgan's (p.924-926) explains this concept which is essential for anaesthetists:
Closing capacity = the lung volume at which small, non-cartilaginous airways in dependent lung zones begin to collapse during expiration.
Nitrogen Single-Breath Test (Morgan's Fig. 23-6)
- Inhale 100% O₂ from RV to TLC
- Exhale slowly - measure expired N₂ concentration
- Phase I: 0% N₂ (anatomic dead space)
- Phase II: Mixed gas
- Phase III: "Alveolar plateau" - should be flat; steep slope = non-uniform distribution
- Phase IV: N₂ concentration rises sharply = closing volume - dependent airways starting to close
Why This Matters
Closing capacity is normally below FRC (airways stay open). But:
- In elderly patients and obese patients, closing capacity rises above FRC - even while awake
- Under general anaesthesia, FRC falls ~0.5 L - this may bring FRC below closing capacity
- Result: airway closure during normal tidal breathing → V/Q mismatch → hypoxaemia
Morgan's summarizes: "At lower lung volumes, alveoli in dependent areas continue to be perfused but are no longer ventilated; the resulting intrapulmonary shunting of deoxygenated blood (venous admixture) promotes hypoxaemia."
📘 PART 9: CARDIOPULMONARY EXERCISE TESTING (CPET)
CPET is the gold standard for integrating all three systems: respiratory, cardiovascular, and musculoskeletal.
Miller's (p.1307): "CPET involves brief incremental exercise (treadmill or bike) with continuous monitoring of ECG, pulse oximetry, respiratory rate, exhaled gases, airflow, and volume."
Key CPET Parameters
| Parameter | Definition | Risk Threshold |
|---|---|---|
| VO₂max | Maximum oxygen consumption at peak exercise - overall cardiorespiratory fitness | < 15 mL/kg/min = increased PPC risk |
| Anaerobic Threshold (AT) | VO₂ above which VCO₂ rises disproportionately - sustainable exercise capacity | < 10 mL/kg/min = increased risk |
| VE/VCO₂ ratio | Efficiency of gas exchange; reflects V/Q matching and dead space | Elevated ratio predicts PPCs more accurately than VO₂max |
📘 PART 10: PREOPERATIVE PFT RISK STRATIFICATION
General Surgery
Miller's (p.3868): "PFTs may be indicated for diagnosis or management decisions but have NOT been shown to predict postoperative pulmonary complications (PPCs) except for patients having lung resections."
Key thresholds for general surgical risk:
- FEV₁ < 60% predicted - associated with increased risk of serious PPCs
- DLCO < 60% predicted - triggers referral for exercise testing
- Baseline PaCO₂ > 45 mmHg - higher risk for postoperative morbidity
Thoracic Surgery: The "Three-Legged Stool"
For lung resection surgery, Miller's (p.3444) describes the framework:
"No single test of respiratory function has shown adequate validity as a sole preoperative assessment. Prior to surgery, an estimate of respiratory function in all three areas - lung mechanics, parenchymal function, and cardiopulmonary interaction - should be made."
The Three Legs:
| Leg | Best Test | Risk Threshold |
|---|---|---|
| Respiratory Mechanics | ppoFEV₁ (predicted postoperative FEV₁) | < 30-40% predicted |
| Lung Parenchymal Function | ppoDLCO (predicted postoperative DLCO) | < 30-40% predicted |
| Cardiopulmonary Interaction | VO₂max (CPET) | < 15 mL/kg/min |
Predicted Postoperative Values (ppo)
The ppo value estimates function remaining after resection. The formula accounts for how much functioning lung is being removed.
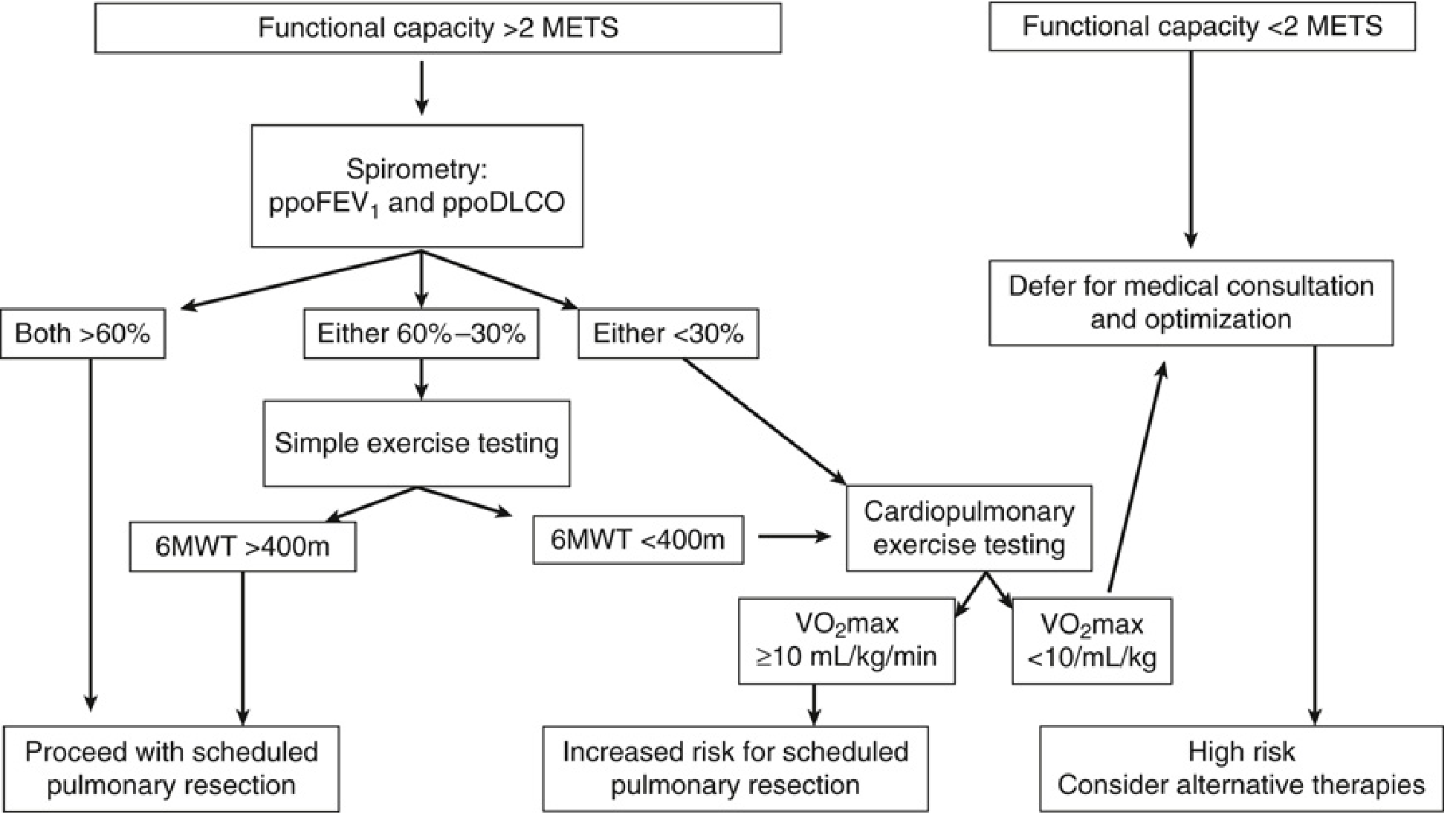
Fig. 49.2 - Preoperative Respiratory Investigation Algorithm for Pulmonary Resection (Miller's Anesthesia 10e, p.7080)
Reading the Algorithm:
- Functional capacity > 2 METs?
- Yes → proceed to spirometry: ppoFEV₁ and ppoDLCO
- No → defer for medical consultation and optimization
- Both ppoFEV₁ AND ppoDLCO > 60% → Proceed safely
- Either value 30-60% → Simple exercise testing (6-minute walk test)
- 6MWT > 400 m → Proceed (increased risk, acceptable)
- 6MWT < 400 m → Full CPET
- Either value < 30% → Full CPET directly
- VO₂max ≥ 10 mL/kg/min → Increased risk, proceed with caution
- VO₂max < 10 mL/kg/min → High risk - consider alternative therapies
VATS vs Open Thoracotomy: Shifting Thresholds
Miller's (p.3466): "The threshold for increased risk in ppoFEV₁ for lobectomy appears to have shifted from < 40% for open thoracotomy to < 30% for VATS."
This means patients previously deemed too high-risk for open surgery may be acceptable for minimally invasive resection.
📘 PART 11: EXTUBATION DECISIONS AFTER PULMONARY RESECTION
Miller's (p.3491) provides clear guidance:
| ppoFEV₁ | Criteria for OR Extubation |
|---|---|
| > 40% | Can usually extubate in OR if patient is "AWaC" (Alert, Warm, and Comfortable) |
| 30-40% | Extubate in OR if exercise tolerance AND lung parenchymal function above risk thresholds |
| 20-30% | Consider early extubation if thoracic epidural analgesia used OR if VATS performed |
| < 20% | Staged weaning from mechanical ventilation postoperatively |
📘 PART 12: DISEASE-SPECIFIC PFT PATTERNS SUMMARY
| Disease | FEV₁/FVC | FEV₁ | FVC | TLC | DLCO | Key Feature |
|---|---|---|---|---|---|---|
| COPD | ↓ (<0.70) | ↓↓ | ↓ or N | ↑ (hyperinflation) | ↓ (emphysema) | Irreversible obstruction |
| Asthma | ↓ | ↓ | N | N | N | Reversible with bronchodilator |
| Pulmonary Fibrosis | N or ↑ | ↓ | ↓↓ | ↓↓ | ↓↓ | Restrictive + impaired diffusion |
| Emphysema | ↓ | ↓ | N or ↓ | ↑↑ | ↓↓ | Air trapping, loss of alveolar surface |
| Neuromuscular Disease | N | ↓ | ↓↓ | ↓ | N | Restrictive, normal diffusion |
| Obesity | N | ↓ | ↓ | ↓ | N | Restrictive, ↓ FRC, ↑ closing capacity |
| Pulmonary Hypertension | N | N | N | N | ↓ | Isolated DLCO reduction |
📘 PART 13: PRACTICAL ANAESTHETIC IMPLICATIONS SUMMARY
| Situation | What PFTs Tell You | Anaesthetic Action |
|---|---|---|
| COPD patient for surgery | Severity of obstruction | Optimize bronchodilators, plan for possible ICU postop |
| Lung resection candidate | ppoFEV₁, ppoDLCO | Use three-legged stool; may need CPET |
| Unexplained dyspnoea | Obstructive vs restrictive pattern | Tailor further workup |
| Upper airway mass | Flow-volume loop shape | Anticipate difficult airway; have plan for obstruction |
| Pre-induction in obese patient | ↓ FRC, ↑ closing capacity | Pre-oxygenation in head-up position; PEEP titration |
| Post-op respiratory failure | Baseline FEV₁, DLCO | Guides weaning decisions, extubation readiness |
| Bullous disease | Plethysmography vs dilution discrepancy | Avoid N₂O; cautious with high airway pressures |
| Asthma | Reversibility testing | PFTs have limited perioperative prognostic value in well-controlled asthma |
📘 PART 14: QUICK-REFERENCE MEMORY TABLES
Critical PFT Thresholds for Anaesthesia
| Test | Threshold | Meaning |
|---|---|---|
| FEV₁ | < 60% predicted | Increased risk of PPCs |
| FEV₁/FVC | < 0.70 | Obstructive disease |
| DLCO | < 60% predicted | Refer for exercise testing |
| ppoFEV₁ | < 30-40% | High risk for lung resection |
| ppoDLCO | < 30-40% | High risk for lung resection |
| VO₂max | < 15 mL/kg/min | Increased PPC risk |
| VO₂max | < 10 mL/kg/min | Very high risk - consider alternatives |
| AT | < 10 mL/kg/min | Increased surgical risk |
| PaCO₂ | > 45 mmHg | Higher postoperative morbidity risk |
Methods to Measure FRC (Cannot Use Spirometry)
| Method | Principle | Accuracy in Emphysema |
|---|---|---|
| Body Plethysmography | Boyle's Law | Best - includes trapped gas |
| Nitrogen Washout | Conservation of N₂ mass | Underestimates (misses trapped gas) |
| Helium Dilution | Conservation of He mass | Underestimates (misses trapped gas) |
Sources
- Miller's Anesthesia, 2-Volume Set, 10e - Chapters 12 (Respiratory Physiology), 29 (Preoperative Assessment), 49 (Thoracic Surgery), 52 (Vascular Surgery)
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Chapter 23 (Respiratory Physiology and Anesthesia)
Using millers, Morgan and barasch discuss in detail about Acute post operative pain, Fluid management in major abdominal surgery, anaesthetic management in Colles fracture and Peripheral vascular diseases. Use the sources that I’ve shared for the formatting of the answers. Use millers, Morgan and barasch anaesthesia books and discuss all the important aspects
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Complete Anaesthesia Guide
Acute Postoperative Pain | Fluid Management in Major Abdominal Surgery | Colles Fracture | Peripheral Vascular Disease
Sources: Miller's Anesthesia 10e | Morgan and Mikhail's Clinical Anesthesiology 7e | Barash Clinical Anesthesia 9e
🔴 TOPIC 1: ACUTE POSTOPERATIVE PAIN
📘 PART 1: WHY POSTOPERATIVE PAIN MATTERS
Globally, over 300 million surgical procedures are performed each year. Despite significant advances in knowledge and treatment of acute pain, the management of acute postoperative pain remains less than optimal.
"Inadequate relief of postoperative pain has adverse physiologic effects that can contribute to significant morbidity and mortality, resulting in the delay of patient recovery and return to daily activities." - Barash 9e, Ch. 55
In 2016, a multisociety collaborative (ASA + ASRA + APS) published treatment guidelines for acute postoperative pain. A further update in 2021 established 7 guiding principles (Barash 9e, Table 55-1):
- Conduct a preoperative evaluation including psychologic conditions, history of chronic pain, substance abuse, and previous pain treatment responses
- Use a validated pain assessment tool to track responses and adjust plans
- Offer multimodal analgesia - medications + nonpharmacologic interventions
- Provide patient- and family-centred education on treatment options
- Educate on proper storage and disposal of opioids and tapering
- Adjust the plan based on adequacy of pain relief and presence of adverse events
- Have access to appropriate resources
📘 PART 2: NEUROBIOLOGY OF PAIN - THE BASICS
Understanding pain mechanisms is essential for targeted multimodal therapy.
The Four Elements of Pain Processing (Barash 9e, Fig. 55-6)
1. TRANSDUCTION
Noxious thermal / chemical / mechanical stimulus
→ converted to action potential at nociceptors (Aδ and C fibers)
2. TRANSMISSION
Action potential conducted via:
→ 1st-order neuron: periphery to dorsal horn (DRG)
→ 2nd-order neuron: dorsal horn to thalamus
→ 3rd-order neuron: thalamus to cortex
3. MODULATION
Dorsal horn is the KEY site
↓ Inhibition: GABA, glycine, descending norepinephrine/serotonin/endorphins
↑ Augmentation: Central sensitization ("wind-up")
4. PERCEPTION
Integration in somatosensory and limbic cortices
"Traditional analgesic therapies have only targeted pain perception. A multimodal approach should target all four elements of the pain-processing pathway." - Barash 9e, p.4645
Peripheral Sensitization
Tissue damage activates:
- Macrophages, mast cells, lymphocytes, platelets
- Antidromic release of substance P and glutamate from C fibers
- Chemical milieu: prostaglandins, bradykinin, serotonin, histamine, cytokines
- Result: primary hyperalgesia (exaggerated response at the injury site)
Central Sensitization
- "Wind-up" phenomenon: repetitive C-fiber stimulation of WDR neurons in dorsal horn
- Hyperalgesia: exaggerated response to a normally painful stimulus
- Allodynia: painful response to a normally non-painful stimulus
📘 PART 3: ACUTE EFFECTS OF UNCONTROLLED POSTOPERATIVE PAIN
Miller's (Ch. 77) provides a comprehensive breakdown:
1. Neuroendocrine Stress Response
Nociceptive stimuli → hypothalamic-pituitary-adrenocortical + sympathoadrenal activation:
- ↑ Catecholamines, cortisol, ACTH, ADH, glucagon, aldosterone, renin, angiotensin II
- ↓ Anabolic hormones
- Result: Na/water retention, hyperglycaemia, free fatty acids, negative nitrogen balance, hypermetabolic/catabolic state
2. Cardiovascular Effects
- ↑ Sympathetic tone → tachycardia, hypertension, increased myocardial O₂ demand
- Hypercoagulability: ↓ natural anticoagulants, ↑ procoagulants, ↑ platelet reactivity
- Risk of: DVT, vascular graft failure, myocardial ischaemia
3. Respiratory Effects
- Inhibitory spinal reflex on phrenic nerve → reduced diaphragmatic function
- ↓ Tidal volumes, inadequate cough
- Especially harmful after upper abdominal and thoracic surgery
- Risk of: postoperative pulmonary complications, atelectasis, pneumonia
4. Gastrointestinal Effects
- Spinal reflex inhibition of GI motility
- Postoperative ileus - delayed return of bowel function
5. Immunological Effects
- Postoperative immunosuppression correlates with severity of surgical injury
- Hyperglycaemia from stress response → poor wound healing + depression of immune function
6. Psychological Effects
- Patient dissatisfaction with surgical experience
- Adverse psychological consequences
📘 PART 4: CHRONIC PERSISTENT POSTSURGICAL PAIN (CPSP)
Miller's (p.11692) highlights this under-recognised problem:
- Incidence: 10% to 65% of postoperative patients (depending on surgery type)
- Severe CPSP: 2% to 10%
| Surgery | CPSP Incidence |
|---|---|
| Limb amputation | 30-83% |
| Thoracotomy | 22-67% |
| Sternotomy | 27% |
| Breast surgery | 11-57% |
| Gallbladder surgery | Up to 56% |
"Poorly controlled acute postoperative pain is an important predictive factor in the development of CPSP. The transition from acute to chronic pain occurs very quickly, and long-term behavioural and neurobiological changes occur much sooner than was previously thought." - Miller's Anesthesia 10e, p.11692
Key point: Noxious stimuli can express new genes in the dorsal horn within 1 hour - sufficient to alter behaviour within the same timeframe. The intensity of acute postoperative pain is a significant predictor of CPSP.
📘 PART 5: PREVENTIVE ANALGESIA
Miller's (p.11693) clarifies the evolution of terminology:
- Preemptive analgesia: the older concept - intervention before surgical incision prevents central sensitization from incisional injury only
- Preventive analgesia: the broader, current concept - encompasses the entire perioperative period to prevent central sensitization from incisional AND inflammatory injury
The idea: reduce or eliminate the peripheral nociceptive barrage reaching the CNS throughout the perioperative period to blunt central sensitization.
📘 PART 6: MULTIMODAL ANALGESIA - THE CORNERSTONE
"Multimodal analgesia combines different classes of medications with different pharmacological mechanisms of action, resulting in additive or synergistic effects to reduce postoperative pain while reducing analgesic dosage and associated side effects." - Morgan's 7e, Ch. 48
The Components
1. NSAIDs / COX-2 Inhibitors
- Inhibit cyclooxygenase (COX) → ↓ prostaglandin synthesis
- Both peripheral (sensitization) and spinal COX inhibition
- Benefits: ↓ pain intensity, ↓ opioid requirements, ↓ PONV, ↓ sedation, ↓ urinary retention
- Cautions: GI bleeding (non-selective), ↓ renal function, anastomotic healing concerns
- COX-2 inhibitors (celecoxib): fewer GI effects, minimal platelet inhibition; celecoxib confirmed cardiovascularly non-inferior to ibuprofen/naproxen (24,081-patient RCT - Miller's p.11712)
2. Acetaminophen (Paracetamol)
- Central mechanism: activates descending serotonergic pathways + inhibits prostaglandin synthesis
- Analgesic effect 20-30% less than NSAIDs, but safer profile
- IV formulation approved - useful when oral route unavailable
- When combined with NSAIDs: ↓ pain scores + ↓ opioid consumption significantly
- Max dose: 4 g/day in adults; avoid in acute decompensated liver failure
- Preoperative dosing: 975 mg IV (Barash 9e, Table 55-6)
3. Gabapentinoids (Gabapentin / Pregabalin)
- Mechanism: bind voltage-gated calcium channel α2δ subunit in dorsal horn
- Single preoperative dose: ↓ postoperative pain and opioid consumption in first 24h
- May reduce incidence of chronic post-surgical pain
- Side effects: sedation, dizziness (particularly in elderly - risk of falls)
- Gabapentin dosing: 300 mg for age <65 years; 100-300 mg for age >65 years (Barash 9e, Table 55-6); renally cleared - adjust in renal failure
4. NMDA Receptor Antagonists
Ketamine:
- Bolus: 0.1-0.35 mg/kg; Infusion: 0.1-1 mg/kg
- Particularly beneficial in opioid-tolerant patients
- Blocks central sensitization and wind-up
- Avoid in psychiatric disturbance, cardiovascular/hepatic disease, pregnancy
Magnesium:
- NMDA antagonist and calcium channel blocker
- Bolus: 1-3 g; Infusion: 0.5-1 g
- Reduces postoperative pain and opioid consumption
- Side effects: hypotension, potentiation of NMB
- Avoid in renal insufficiency, neuromuscular disorders, electrolyte imbalance
5. IV Lidocaine
- Systemic anti-inflammatory and analgesic effect
- Bolus: 0.5-1.5 mg/kg; Infusion: 1-1.5 mg/kg
- In major abdominal surgery: associated with faster return of bowel function and decreased hospital stay (Morgan's 7e)
- Opioid-sparing
- Avoid combining with regional LA techniques; avoid in cardiac abnormalities, seizure disorder
6. Alpha-2 Agonists (Dexmedetomidine)
- Bolus: 0.5-0.6 mcg/kg; Infusion: 0.3-1 mcg/kg/h
- Opioid-sparing; useful as perineural adjunct for nerve blocks
- Main side effects: hypotension and bradycardia
7. Opioids (Systemic)
- "Despite the increasing use of nonopioid analgesic medications, the use of systemic opioids remains a cornerstone in the management of surgical pain." - Morgan's 7e
- IV PCA provides superior analgesia and patient satisfaction vs PRN opioids
- Oral opioids: important option but judicious prescribing essential given opioid epidemic
- ~6% of opioid-naive patients will continue filling prescriptions 3-6 months post-surgery
📘 PART 7: IV PATIENT-CONTROLLED ANALGESIA (IV PCA)
Miller's (p.11701-11704) provides a thorough discussion:
Principle: Negative feedback loop - when pain experienced, patient self-administers analgesic; when pain reduced, no further demands.
Advantages over PRN:
- Compensates for wide interpatient variability
- Avoids pharmacokinetic variability of IM injection
- Eliminates administrative delays
- Superior analgesia and patient satisfaction (meta-analysis confirmed)
- Greater perceived control
Key PCA Settings:
- Demand dose
- Lockout interval
- 1-hour and 4-hour limits
- Background infusion (see below)
Background infusion:
- NOT recommended in opioid-naive adults - increases total dose and respiratory adverse events
- Recommended for opioid-tolerant patients and paediatric patients
Rate of respiratory depression with IV PCA: ~1.5% - not more frequent than PRN opioids. Risk factors:
- Background infusion
- Advanced age
- Concomitant sedatives
- Obstructive sleep apnoea
- Operator programming errors
📘 PART 8: NEURAXIAL ANALGESIA
Miller's (Table 77.3) - Properties of Neuraxial Opioids:
| Property | Lipophilic (Fentanyl, Sufentanil) | Hydrophilic (Morphine, Hydromorphone) |
|---|---|---|
| Onset | Rapid (5-10 min) | Delayed (30-60 min) |
| Duration | Shorter (2-4 hours) | Longer (6-24 hours) |
| CSF spread | Minimal | Extensive |
| Site of action | Spinal < systemic | Primarily spinal |
| Delayed resp. depression | Primarily early, minimal delay | Both early AND delayed (>6h) possible |
| PONV/Pruritus | Lower incidence | Higher incidence |
Clinical tip: Lipophilic opioids suit ambulatory patients needing rapid onset + moderate duration. Hydrophilic opioids (morphine) suit inpatient settings where longer analgesia is beneficial.
Epidural analgesia - for high thoracic/abdominal surgery: provides superior pain control, avoids systemic opioid respiratory depression. Combination of LA + opioid (e.g. bupivacaine + fentanyl) provides synergistic analgesia.
Monitoring Requirements for Postoperative Analgesia (Miller's Box)
- Vital signs: temperature, HR, BP, RR, average pain score
- Pain score at rest AND with activity
- Respiratory status + level of sedation
- Nausea/vomiting, pruritus, urinary retention
- Motor block and sensory level assessment
- Evidence of epidural haematoma
📘 PART 9: PREOPERATIVE DOSING TABLE (Barash 9e, Table 55-6)
| Drug | Pre-op Dose | Comments |
|---|---|---|
| Acetaminophen | 975 mg IV (adults) | Avoid in acute liver failure |
| Celecoxib | 400 mg PO (<65y); 200 mg PO (>65y) | Avoid in pre-existing renal failure |
| Gabapentin | 300 mg PO (<65y); 100-300 mg PO (>65y) | 100% renal clearance - dose-adjust |
🔵 TOPIC 2: FLUID MANAGEMENT IN MAJOR ABDOMINAL SURGERY
📘 PART 1: WHY FLUID MANAGEMENT MATTERS
"There is increasing evidence that perioperative fluid administration affects patient outcome following major surgery, with the quantity of fluid administered - either too restrictive or too liberal - being associated with increased incidence of postoperative complications." - Morgan's 7e, Ch. 48
Consequences of Fluid Overload (Liberal Therapy)
- ↓ Tissue oxygenation
- Anastomotic leakage
- Pulmonary oedema and pneumonia
- Wound infection
- Postoperative ileus
- Prolonged hospitalisation
- Weight gain of 3-6 kg - impairs postoperative mobilisation
Consequences of Excessive Restriction
- The RELIEF Trial (largest RCT to date): Restrictive fluid therapy (≤5 mL/kg/h) vs liberal (8 mL/kg/h) with isotonic crystalloid - acute kidney injury occurred MORE frequently in the restrictive group
- Hypovolaemia → organ hypoperfusion → AKI, anastomotic ischaemia
Current recommendation (Morgan's 7e): Target a positive fluid balance of 1-2 L at the end of surgery using isotonic balanced crystalloid solutions.
📘 PART 2: GOAL-DIRECTED FLUID THERAPY (GDFT)
"GDFT aims to avoid both hypovolaemia and fluid excess, and it is the optimal approach for fluid administration in high-risk surgical patients." - Morgan's 7e, p.2114
Principles of GDFT
- Optimize hemodynamic parameters rather than using fixed rate protocols
- Parameters monitored: HR, BP, stroke volume (SV), pulse pressure variation (PPV), stroke volume variation (SVV)
- Guided by: pulse-contour arterial waveform analysis, oesophageal Doppler, transesophageal echocardiography
Evidence Base
- Miller's (p.39): Closed-loop-assisted intraoperative GDFT during major abdominal surgery - reduction in intraoperative net fluid balance, associated with reduced postoperative complications
- Multiple RCTs support GDFT in colorectal surgery, kidney transplant, and high-risk major surgery
- Kidney transplant data (Miller's p.3218): GDFT group had lower rates of early graft dysfunction AND early cardiovascular events even with similar total fluid volumes
📘 PART 3: CHOOSING THE RIGHT FLUID
Morgan's First-Line Fluid Replacement Table (Table 48-3)
| Physiological Requirement | Replace With | Amount |
|---|---|---|
| Insensible losses (closed abdomen) | Isotonic balanced crystalloid | 0.5 mL/kg/h |
| Insensible losses (open abdomen) | Isotonic balanced crystalloid | 1 mL/kg/h |
| Urine production | Crystalloid | Measured output |
| Blood loss | Iso-oncotic colloid | Estimated losses |
| Further preload deficit | Colloid | Per clinical/monitoring estimation |
Crystalloids
- Isotonic balanced crystalloids (Hartmann's/Ringer's Lactate, Plasmalyte) - preferred over normal saline
- Normal saline risks: hyperchloraemic metabolic acidosis - avoid in high volumes
- Miller's (p.5666): "The use of balanced salt solutions avoids hyperchloraemic metabolic acidosis and is likely preferable in most circumstances, including in patients with end-stage kidney disease."
Colloids
- Replace intravascular losses (blood, plasma)
- Iso-oncotic colloids used to replace physiologically important blood losses
- Debate remains on HES vs albumin vs gelatin for specific indications
📘 PART 4: MONITORING INTRAOPERATIVE FLUID STATUS
Dynamic Predictors of Fluid Responsiveness (Best Indicators)
| Parameter | Threshold for Fluid Responsiveness |
|---|---|
| Pulse Pressure Variation (PPV) | > 13% |
| Stroke Volume Variation (SVV) | > 10-15% |
| Oesophageal Doppler SV | ↑ >10% after 200 mL fluid challenge |
Limitations of static monitors:
- CVP: unreliable for predicting fluid responsiveness - not recommended for guiding fluid therapy
- Urine output: Miller's (p.5657) - "Intraoperative urine formation is not validated as a measure of the risk of postoperative renal dysfunction" - do NOT use as sole guide for fluid management
Point-of-Care Devices
- PiCCO system (transpulmonary thermodilution)
- LiDCO, PICCO, FloTrac (pulse contour analysis)
- Oesophageal Doppler - non-invasive cardiac output
- TEE - visual assessment of volume status + cardiac function
📘 PART 5: LAPAROSCOPIC ABDOMINAL SURGERY - SPECIAL CONSIDERATIONS
Barash 9e (p.3659) notes important considerations for laparoscopic major abdominal surgery:
- Pneumoperitoneum creates volume shifts that alter expected perioperative fluid therapy goals
- Classic hemodynamic indicators (HR, BP, CVP) may NOT be reliable during laparoscopy due to pneumoperitoneum and positioning
- Urine output as a guide is limited during pneumoperitoneum
- Fluid loading (40 mL/kg vs 15 mL/kg) in ambulatory laparoscopic cholecystectomy - unexpected improvements in postoperative pulmonary function, exercise capacity, and well-being
- However, in patients with comorbidities undergoing major laparoscopic abdominal surgery, fluid loading may be deleterious
📘 PART 6: FLUID MANAGEMENT IN ENHANCED RECOVERY PROTOCOLS (ERAS)
Morgan's (p.1900-1904) integrates fluid management into ERAS:
The ERAS fluid strategy:
- Avoid prolonged preoperative fasting - allow clear fluids up to 2h preoperatively
- Carbohydrate loading reduces the preoperative fluid deficit
- Intraoperative: GDFT with balanced crystalloids targeting SVV/PPV
- Avoid positive balance >1-2 L by end of surgery
- Early postoperative: switch to oral fluids; discontinue IV fluids early
- Avoid routine nasogastric tubes - they increase ileus
Other ERAS elements that directly interact with fluid therapy:
- Normothermia maintenance - reduces sympathetic activation and vasoconstriction
- Optimal oxygenation - FiO₂ 40-60% intraoperatively; evidence on 80% oxygen inconclusive
- PONV prophylaxis - ensures early oral fluid intake
- Early mobilisation - improves tissue oxygenation and reduces DVT risk
📘 PART 7: RENAL PROTECTION DURING MAJOR ABDOMINAL SURGERY
Miller's (p.5663, Ch. 15):
- Intraoperative hypotension and hypovolaemia are significant risk factors for AKI
- AKI occurs in 5-25% of hospitalised patients; mortality of ICU AKI = 50-80%
- Goal: maintain renal blood flow and perfusion pressure
- Balanced crystalloids associated with lower rates of AKI vs saline
- Volume overload itself is a risk factor for adverse outcomes in AKI
- Preoperative creatinine >2 mg/dL: independent risk factor for cardiac complications
🟢 TOPIC 3: ANAESTHETIC MANAGEMENT OF COLLES FRACTURE
📘 PART 1: WHAT IS A COLLES FRACTURE?
A Colles fracture is a distal radius fracture with dorsal displacement and angulation, typically occurring after a fall on an outstretched hand. It is one of the most common fractures in adults, particularly in elderly women with osteoporosis.
Anaesthetic options:
- Brachial plexus block (regional anaesthesia) - most ideal
- IV Regional Anaesthesia (Bier Block) - simple and effective
- General anaesthesia - usually not required; reserved for special circumstances
- Haematoma block - simple local infiltration
📘 PART 2: BRACHIAL PLEXUS ANATOMY - THE FOUNDATION
Understanding the plexus is critical to choosing the right block level.
Morgan's (p.1861): "Local anesthetic may be deposited at any point along the brachial plexus, depending on the desired block effects: interscalene for shoulder and proximal humerus surgical procedures; and supraclavicular, infraclavicular, or axillary for surgeries distal to the mid-humerus."
BRACHIAL PLEXUS (C5-T1)
Roots → Trunks → Divisions → Cords → Branches (Terminal Nerves)
C5, C6 → Upper trunk
C7 → Middle trunk
C8, T1 → Lower trunk
↓
Anterior/Posterior Divisions
↓
Lateral, Medial, Posterior Cords
↓
Terminal Nerves: Musculocutaneous, Median, Ulnar, Radial, Axillary
Miller's (p.6235):
- Above clavicle blocks (interscalene, supraclavicular) → target ventral rami, trunks, divisions
- Below clavicle blocks (infraclavicular, axillary) → target cords and terminal nerves
📘 PART 3: CHOOSING THE RIGHT BLOCK FOR COLLES FRACTURE
For Colles fracture (distal radius, wrist): The wrist and hand are supplied by the lower trunk (C8-T1) - median, ulnar, and radial terminal nerves.
| Block | Approach | Coverage | Suitable for Colles? |
|---|---|---|---|
| Interscalene | Roots/Upper trunks (C5-C7) | Shoulder, upper arm | ❌ Misses C8-T1 (ulnar nerve) |
| Supraclavicular | Trunks/Divisions | Entire arm from mid-humerus distally | ✅ Excellent |
| Infraclavicular | Cords | Elbow to hand | ✅ Very good |
| Axillary | Terminal nerves | Elbow to hand | ✅ Good |
| Bier Block (IVRA) | Venous absorption | Entire forearm/hand | ✅ Simple, effective |
Best choice for Colles fracture: Supraclavicular block (or infraclavicular/axillary)
📘 PART 4: SUPRACLAVICULAR BRACHIAL PLEXUS BLOCK
Why supraclavicular for Colles?
- Targets trunks and divisions - ensures coverage of all terminal nerves to the hand
- Compact cluster of nerves near subclavian artery makes it reliable and complete
- No phrenic nerve block (unlike interscalene) - safer in respiratory compromise
Technique (Barash 9e, p.2951)
Patient position: Supine, head turned ~45° to contralateral side
Nerve stimulation technique:
- Midpoint of clavicle marked; needle entry point 1 cm posterior to midpoint in interscalene groove
- 2.5-5 cm, 22-gauge needle; initial insertion angle 45° cephalad
- Acceptable responses: pectoralis, deltoid, biceps (upper trunk), triceps (upper/middle trunk), forearm, hand (lower trunk)
- Current: 0.4 mA (0.1-0.3 ms)
- Volume: 25-40 mL local anaesthetic
Ultrasound-guided technique:
- Probe in coronal oblique plane at lateral end, just above clavicle
- Identify subclavian artery; plexus sits superolateral to subclavian artery above first rib
- Plexus appears as cluster of hypoechoic nodules
- In-plane needle approach; spread around all trunks/divisions confirms placement
Risk: Pneumothorax (1%) - identify pleura clearly; never angle medially below 20°
📘 PART 5: AXILLARY BRACHIAL PLEXUS BLOCK
Suitable for: Forearm and hand surgery (elbow and below).
Morgan's (p.1862):
- "Brachial plexus block at the level of the cords provides excellent anesthesia for procedures at or distal to the elbow."
- The axillary, musculocutaneous, and medial brachial cutaneous nerves branch proximal to LA deposition - they are usually spared and must be independently blocked
- The musculocutaneous nerve must be independently blocked to anaesthetise the lateral forearm
Technique:
- Arm abducted 90°, elbow flexed 90°
- Identify axillary artery by palpation/Doppler
- Ultrasound: identify 4 terminal nerves around the artery (median anterosuperior, ulnar inferior, radial posterior, musculocutaneous within coracobrachialis)
- Multiple injection technique: 5-8 mL per nerve
- Total volume: ~30-40 mL
📘 PART 6: IV REGIONAL ANAESTHESIA (BIER BLOCK)
Morgan's (p.1862): "Intravenous regional anesthesia (Bier block) can provide intense surgical anesthesia for relatively short (45-60 min) surgical procedures on an extremity."
Principle: Local anaesthetic injected IV into an exsanguinated, double-cuff tourniquet-occluded limb distributes to nerve endings via venous system.
Technique for Colles Fracture
- Place IV cannula in dorsum of hand on operative side
- Apply double-cuff tourniquet to upper arm
- Exsanguinate limb with Esmarch bandage (or elevation if fracture)
- Inflate proximal cuff to 100 mmHg above systolic BP
- Inject 0.5% prilocaine 40 mL (3 mg/kg) or 0.5% lidocaine slowly
- Onset of dense anaesthesia within 5-10 minutes
- After 20-25 min, inflate distal cuff (now over anaesthetised skin) then deflate proximal cuff
- Minimum tourniquet inflation time: 25 minutes to prevent systemic LA toxicity on release
Advantages:
- Technically simple
- Rapid onset, complete block
- Muscle relaxation
- Bloodless field with tourniquet
Disadvantages/Risks:
- Maximum duration ~90 minutes (tourniquet tolerance)
- No postoperative analgesia
- Risk of LAST if tourniquet deflated too early
- Contraindicated in sickle cell disease, Raynaud's, peripheral vascular disease
📘 PART 7: INTERSCALENE BLOCK - WHY NOT FOR COLLES
Miller's (p.6236): "This technique is not recommended for forearm and hand surgery because blockade of the inferior trunk (C8 and T1) can be incomplete and require supplementation of the ulnar nerve for adequate surgical anesthesia in that distribution."
Morgan's (p.1861): "A properly performed interscalene block almost invariably blocks the ipsilateral phrenic nerve, so careful consideration must be given to patients with severe pulmonary disease or pre-existing contralateral phrenic nerve palsy. Bilateral interscalene blocks are ALWAYS contraindicated."
Phrenic nerve block considerations:
- 100% ipsilateral hemidiaphragmatic paralysis with interscalene
- Reduces ipsilateral lung function by ~25%
- Clinically significant in patients with COPD, obesity, contralateral phrenic nerve palsy
📘 PART 8: LOCAL ANAESTHETIC AGENTS FOR UPPER LIMB BLOCKS
| Drug | Concentration | Volume | Onset | Duration | Comments |
|---|---|---|---|---|---|
| Lignocaine | 1.5-2% | 30-40 mL | Fast (10-15 min) | 2-3 h | Good for Bier block |
| Bupivacaine | 0.5% | 25-35 mL | Medium (20-30 min) | 6-12 h | Excellent for single-shot supraclavicular |
| Ropivacaine | 0.5-0.75% | 25-35 mL | Medium | 6-12 h | Safer cardiac profile than bupivacaine |
| Levobupivacaine | 0.5% | 25-35 mL | Medium | 8-14 h | Lowest cardiac toxicity |
Adjuvants to prolong block duration:
- Dexamethasone (4-8 mg perineurally or IV) - extends block by 6-8 hours
- Dexmedetomidine (50-100 mcg perineurally) - extends and deepens block
- Clonidine (150 mcg perineurally) - moderate prolongation
📘 PART 9: PATIENT CONSIDERATIONS FOR COLLES FRACTURE
| Consideration | Relevance | Action |
|---|---|---|
| Elderly / frail | High prevalence of Colles; reduced LA dose needed | Reduce volume by 20-30% |
| Osteoporosis medications | May affect bone healing | Medication reconciliation |
| Anticoagulation | Common in elderly (AF, DVT prophylaxis) | Peripheral nerve blocks generally safe; avoid deep blocks if INR >1.5 |
| NSAID use | Analgesic option | Caution in renal impairment, GI history |
| Comorbidities | Often multiple in elderly | Regional avoids GA hazards |
| Closed reduction | Short procedure, adequate sedation may be needed | Titrated IV sedation (midazolam + fentanyl/ketamine) alongside block |
General anaesthesia - if regional contraindicated or refused:
- LMA appropriate for most cases
- Short-acting agents preferred (propofol, sevoflurane, desflurane)
- Multimodal analgesia at emergence
🟠 TOPIC 4: PERIPHERAL VASCULAR DISEASE (PVD) - ANAESTHETIC MANAGEMENT
📘 PART 1: THE HIGH-RISK PVD PATIENT
Miller's (p.7919): "Major vascular surgery is particularly challenging to the anesthesiologist because these are high-risk operations in a patient population with a high prevalence of either overt or occult coronary artery disease, which is the leading cause of perioperative and long-term mortality after vascular surgery."
Key principle: "Maintenance of vital organ perfusion and function by the provision of stable perioperative hemodynamics is more important to overall outcome than is the choice of anesthetic drug or technique."
Coexisting Disease in PVD Patients (Miller's Ch. 52)
- Coronary artery disease (CAD): Leading cause of perioperative mortality. In the Cleveland Clinic series of 1000 PVD patients: only 8.5% had normal coronary arteries; 60% had advanced/severe lesions (>70% stenosis)
- Hypertension: Very common; systemic atherosclerosis
- Diabetes mellitus: Peripheral and autonomic neuropathy; impaired wound healing; nephropathy
- Chronic renal disease: Serum creatinine >2 mg/dL = independent risk factor for cardiac complications; CrCl <60 mL/min = independent predictor of short- and long-term mortality
- COPD/Pulmonary disease: Smoking history; spirometry/PFTs needed
- Cerebrovascular disease: Potential for perioperative stroke, particularly with carotid surgery
📘 PART 2: PREOPERATIVE ASSESSMENT
Cardiac Risk Stratification
Miller's (p.7925): CAD assessment should be focused on intermediate clinical risk patients:
- Low risk (<1% cardiac risk): may proceed to surgery
- Intermediate risk (1-5%): noninvasive testing may be warranted
- High risk (>5%): further cardiac evaluation required
Important: Noninvasive testing should only be undertaken if it will change patient management. Prophylactic coronary revascularisation before vascular surgery has NOT been shown to reduce perioperative or long-term morbidity.
Miller's (p.7920): "Guidelines suggest that coronary intervention is rarely necessary to simply decrease the risk for surgery unless such intervention is indicated irrespective of the preoperative context."
Perioperative Medical Optimisation
Beta-blockers:
- Continue chronic beta-blocker therapy throughout perioperative period
- Do NOT use as primary treatment of tachycardia caused by hypovolaemia, anaemia, pain, or infection
- If initiating de novo: start small dose and titrate over 7-10 days before planned surgery
- Acute initiation of large-dose beta-blockade in the perioperative period should be avoided
Statins:
- Continue perioperatively for all patients already on statin therapy
- Benefits: anti-inflammatory, plaque-stabilising, antioxidant effects + lipid lowering
- Can preserve renal function after aortic surgery; improve graft patency after lower extremity bypass
Antiplatelet therapy:
- Requires individualised consideration; risk of surgical bleeding vs thrombotic risk
- Aspirin generally continued; dual antiplatelet therapy management requires cardiologist input
📘 PART 3: INTRAOPERATIVE MONITORING
Miller's (p.7963): For major vascular surgery:
- Arterial catheter (A-line) - routine in all patients undergoing aortic reconstruction; radial artery most commonly used
- Contralateral non-invasive BP cuff as backup
- Central venous access - central line + two large peripheral IVs
- ST-segment analysis - computerised monitoring to detect myocardial ischaemia throughout perioperative period
- Pulmonary artery catheter or TEE - for high-risk patients with severe LV dysfunction
- Neurological monitoring - for carotid endarterectomy (SSEP, EEG, cerebral oximetry)
- Temperature monitoring - postoperative hypothermia associated with many undesirable physiologic effects
📘 PART 4: AORTIC CROSS-CLAMPING PHYSIOLOGY
One of the most challenging aspects of major vascular surgery is managing the haemodynamic response to aortic cross-clamping and unclamping.
Physiologic Changes with Aortic Cross-Clamping (Miller's Box 52.1)
Haemodynamic changes (above clamp):
- ↑ Arterial blood pressure
- ↑ Left ventricular wall tension
- ↑ Pulmonary occlusion pressure and CVP
- ↑ Coronary blood flow
- ↓ Ejection fraction (severe LV impairment)
- Segmental wall motion abnormalities
Below clamp:
- ↓ Arterial blood pressure
- ↓ Renal blood flow
- ↓ Cardiac output (with thoracic cross-clamping)
Metabolic changes:
- ↑ Mixed venous O₂ saturation (reduced consumption below clamp)
- ↑ Epinephrine and norepinephrine
- Eventual metabolic acidosis (lactate accumulation below clamp)
Key insight (Miller's p.7948): Thoracic aortic cross-clamping causes a 155% increase in blood flow above the clamp due to splanchnic blood volume redistribution. The splanchnic veins (25% of total blood volume) are venoconstricted by catecholamines, actively forcing blood proximally.
Management Approach - Cross-Clamping
- Vasodilators (nitroglycerin, nitroprusside) to control proximal hypertension
- Reduce volatile anaesthetic concentration (↓ afterload)
- Consider diverting circulatory support for thoracic cross-clamping
Management Approach - Unclamping (Box 52.3)
- Correct all preoperative fluid deficits BEFORE unclamping
- Replace all blood loss BEFORE unclamping
- Reduce/discontinue vasodilators BEFORE unclamping
- Decrease volatile anaesthetic concentration
- Pre-emptive fluid bolus (~500 mL) immediately before infrarenal clamp release
- For supraceeliac unclamping: more aggressive fluid administration needed
- Have vasopressors ready (phenylephrine, norepinephrine)
- Communicate with surgical team: gradual clamp release or digital compression if severe hypotension
📘 PART 5: CHOICE OF ANAESTHETIC TECHNIQUE
General Anaesthesia (GA)
- Standard for major aortic surgery
- Any volatile anaesthetic acceptable; isoflurane, sevoflurane commonly used
- Volatile anaesthetics provide anaesthetic preconditioning benefit - cardioprotective
- Maintain haemodynamic stability more important than agent choice
Regional Anaesthesia
- Spinal or epidural anaesthesia is favoured for:
- Carotid endarterectomy (CEA) under LA/regional - allows neurological monitoring
- Lower limb peripheral bypass procedures
- Endovascular procedures (EVAR)
- Benefits of regional for vascular surgery:
- Improved peripheral blood flow (sympathetic blockade → vasodilation → ↑ graft flow)
- ↓ DVT/thromboembolism risk
- ↓ Coagulation activation
- ↓ Pulmonary complications in patients with significant lung disease
- Better postoperative analgesia
Miller's (p.7942): "Although improved pulmonary outcome with regional anesthesia is not clear, patients with significant pulmonary disease may benefit from epidural techniques."
Combined GA + Epidural
- Used for open aortic and major abdominal vascular procedures
- Epidural provides excellent intraoperative and postoperative analgesia
- Avoids systemic opioid respiratory depression
- Facilitates early extubation
📘 PART 6: SPECIFIC PERIPHERAL VASCULAR PROCEDURES
A. Carotid Endarterectomy (CEA)
Special considerations:
- Brain monitoring during cross-clamping: SSEP, EEG, cerebral oximetry (NIRS), or awake patient (best monitor)
- Awake technique (cervical plexus block): allows real-time neurological assessment - gold standard for detecting shunt need
- Shunting indicated if neurological deterioration occurs after carotid clamping
- Blood pressure management: avoid hypotension (reduces cerebral perfusion) AND avoid hypertension (cerebral hyperperfusion syndrome post-procedure)
- Key complication post-CEA: Hyperperfusion syndrome - headache, seizures, intracerebral haemorrhage
- Haemodynamic instability common from carotid sinus manipulation
B. Lower Extremity Peripheral Bypass (Femoro-popliteal, Femoro-distal)
Anaesthetic options:
- General anaesthesia (LMA or ETT)
- Spinal anaesthesia - excellent for below-knee procedures; sympathetic block improves graft flow
- Epidural anaesthesia - continuous; useful for longer procedures
Regional advantages in lower limb:
- Sympathectomy → peripheral vasodilation → ↑ graft perfusion
- ↓ DVT risk
- Superior postoperative analgesia
Monitoring:
- A-line for haemodynamic monitoring
- Consider TEE/oesophageal Doppler in high-risk cardiac patients
Critical intraoperative events:
- Heparinisation: systemic heparin given before clamping (usually 5000-10,000 IU); protamine reversal after clamp release if required
- Reperfusion injury: ischaemia-reperfusion after limb revascularisation → metabolic acidosis, hyperkalaemia, myoglobinaemia; prepare for these
C. Endovascular Aortic Repair (EVAR)
- Less physiologically stressful than open repair
- Options: GA, regional (spinal/epidural), or monitored anaesthesia care (MAC) with LA
- Endoleak is a complication specific to EVAR - inability to exclude aneurysm sac from arterial blood flow
- Lower haemodynamic instability; no cross-clamping physiology
- Blood loss generally much less than open repair
- Shorter ICU stay
📘 PART 7: RENAL PROTECTION IN VASCULAR SURGERY
Miller's (p.7932-7933):
- Prevalence of acute renal failure: ~7% after abdominal aortic reconstruction
- Renal blood flow decreases with any level of aortic cross-clamping
- Embolic plaque showered into renal arteries especially with suprarenal clamps
Protective strategies:
- Maintain adequate intravascular volume and cardiac output before/during/after clamping
- Mannitol (0.5 g/kg IV before cross-clamping): osmotic diuretic, free radical scavenger
- Selective renal artery perfusion during suprarenal clamping
- Avoid nephrotoxins (contrast, aminoglycosides, NSAIDs)
- Moderate hypothermia provides some renal protection during prolonged ischaemia
- Sodium bicarbonate: correct acidaemia that may exacerbate ischaemic injury
📘 PART 8: POSTOPERATIVE MANAGEMENT OF PVD PATIENTS
Pulmonary Complications
Miller's (p.7932): "Pulmonary complications in the postoperative period are difficult to avoid. Incentive spirometry and CPAP do provide benefit."
- Preoperative optimisation: bronchodilators, antibiotics, steroids as indicated
- Regional anaesthesia/epidural analgesia → avoids systemic opioid respiratory depression
- Early extubation (awake, warm, comfortable) where possible
Cardiovascular Complications
- Continue perioperative ST-segment monitoring postoperatively
- Beta-blocker continuation
- Early detection of perioperative MI (peaks day 2-3 post-thoracotomy/major vascular surgery)
Vascular Graft Complications
- Monitor for graft thrombosis: limb colour, temperature, pulses, Doppler
- Anticoagulation monitoring and management
- Wound care in diabetic/ischaemic limbs
📘 SUMMARY TABLES
Quick Reference: Anaesthetic Technique Selection for PVD
| Procedure | Preferred Technique | Monitoring Essentials |
|---|---|---|
| Open AAA repair | GA ± epidural | A-line, CVP/PAC or TEE, temp |
| EVAR | GA or spinal/regional or MAC | A-line, TEE optional |
| Carotid endarterectomy | Regional (cervical plexus block) or GA + EEG/SSEP | Cerebral oximetry, neurological monitoring |
| Femoro-popliteal bypass | Spinal/epidural or GA | A-line, standard monitors |
| Lower limb embolectomy | Spinal or GA | Standard monitors |
| Peripheral endovascular | MAC or spinal | Standard + A-line |
Key Threshold Values for PVD Patients
| Marker | Threshold | Clinical Significance |
|---|---|---|
| Serum creatinine | > 2 mg/dL | Independent risk factor for cardiac complications |
| Creatinine clearance | < 60 mL/min | Independent predictor of short- and long-term mortality |
| CAD stenosis | > 70% | Advanced disease; consider coronary workup |
| Baseline PaCO₂ | > 45 mmHg | Higher risk for postoperative morbidity |
| Perioperative BP target | Maintain ±20% of baseline | Avoid hypotension AND hypertension |
📚 Sources
- Miller's Anesthesia, 2-Volume Set, 10e - Chapters 42 (Regional Anesthesia), 48 (Fluid Management), 52 (Vascular Surgery), 77 (Acute Pain Management)
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Chapters 23, 31, 46 (Regional), 48 (ERAS/Fluid/Multimodal Analgesia)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Chapters 15 (Laparoscopic), 36 (Regional), 55 (Acute Pain Management)
This is a shared conversation. Sign in to Orris to start your own chat.