Discuss the etiopathology, clinical features and management of nasopharyngeal carcinoma. in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
nasopharyngeal carcinoma treatment advances
Searching the Web
nasopharyngeal carcinoma etiopathology clinical features management RGUHS ENT 50 marks
Reading File
Reading File
Reading File
Searching PubMed
nasopharyngeal carcinoma immunotherapy EBV PD-L1
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
NASOPHARYNGEAL CARCINOMA (NPC)
A Comprehensive 50-Mark Answer for RGUHS MS ENT Examination
INTRODUCTION
Nasopharyngeal carcinoma (NPC) is a distinct malignancy arising from the epithelial lining of the nasopharynx. It differs from other head and neck squamous cell carcinomas in its epidemiology, etiology, biology, and treatment. It is the most common malignancy of the nasopharynx and is characterized by its close association with Epstein-Barr virus (EBV), its marked geographical predilection, and its high radiosensitivity.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 8
- Cummings Otolaryngology Head and Neck Surgery, Chapter 117
SECTION 1: ANATOMY RELEVANT TO NPC
┌─────────────────────────────────────────────────────────────────┐
│ ANATOMICAL DIAGRAM OF NASOPHARYNX │
├─────────────────────────────────────────────────────────────────┤
│ │
│ Sphenoid sinus │
│ ↓ │
│ ══════════════════════ │
│ │ Roof (vault) │← Adenoids │
│ │ ←FOSSA OF ROSENMULLER │ (most common NPC site: 60-70%) │
│ │ (Pharyngeal recess) │ │
│ ══════════════════════ │
│ │ Eustachian tube │← Torus tubarius │
│ │ orifice │ │
│ ══════════════════════ │
│ │ Posterior wall │ │
│ ══════════════════════ │
│ ↓ │
│ Oropharynx │
│ │
│ Boundaries: │
│ Anteriorly → Posterior choanae │
│ Posteriorly → C1 & C2 vertebrae │
│ Superiorly → Base of skull │
│ Inferiorly → Soft palate (imaginary line) │
│ Laterally → Fossa of Rosenmuller + ET orifice │
└─────────────────────────────────────────────────────────────────┘
The Fossa of Rosenmuller (pharyngeal recess) is the most common site of origin of NPC, accounting for >80% of cases. Its location immediately adjacent to the Eustachian tube and the skull base explains the characteristic spread pattern of the tumor.
SECTION 2: EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Global incidence | <1 per 100,000 worldwide |
| Endemic areas | Southern China (Cantonese): 30-50/100,000 |
| Intermediate risk | Greenland Inuit, Maghrebis (NW Africa) |
| Low risk | Caucasians (<1/100,000) |
| Sex ratio | Male : Female = 3:1 |
| Age distribution | Bimodal - Peak 1: 15-25 years; Peak 2: 50-60 years |
| India | Relatively uncommon (~0.4% of cancers), but commoner in Northeast |
- Scott-Brown's (Vol 1), p. 138; Bailey & Love's, Chapter 52
SECTION 3: ETIOPATHOLOGY
NPC is a multifactorial disease with an interplay of three major groups of factors:
┌─────────────────────────────────────────────────────────────┐
│ ETIOPATHOLOGICAL TRIAD OF NPC │
│ │
│ ┌───────────────┐ │
│ │ GENETIC │ │
│ │ Susceptibility│ │
│ └───────┬───────┘ │
│ │ │
│ ┌───────────▼───────────┐ │
│ │ NPC DEVELOPMENT │ │
│ └───────────┬───────────┘ │
│ │ │
│ ┌────────────┴────────────┐ │
│ ▼ ▼ │
│ ┌──────┐ ┌──────────┐ │
│ │ EBV │ │ENVIRON- │ │
│ │Infect│ │MENTAL │ │
│ │-ion │ │Factors │ │
│ └──────┘ └──────────┘ │
└─────────────────────────────────────────────────────────────┘
A. GENETIC FACTORS
- HLA associations: HLA-A2 and HLA-Bsin/B46 are associated with increased susceptibility in Chinese populations
- Familial clustering: ~10% of cases show familial aggregation suggesting inherited genetic susceptibility
- Ethnic predisposition: Cantonese (southern Chinese) people retain elevated risk even when they migrate to low-incidence countries - this confirms genetic rather than purely environmental causation
- Tumor suppressor genes: Loss of heterozygosity at chromosomes 3p, 9p (p16 locus), 11q, 13q, and 14q
- Molecular alterations: Deletion/methylation of RASSF1A, p16, and other tumor suppressor genes are early events
B. VIRAL FACTORS - EBV (CENTRAL ROLE)
The Epstein-Barr virus is the most important etiological factor in endemic NPC.
┌──────────────────────────────────────────────────────────────┐
│ EBV PATHOGENESIS IN NPC - STEP BY STEP │
├──────────────────────────────────────────────────────────────┤
│ │
│ STEP 1: Primary EBV infection (usually childhood) │
│ EBV normally infects B-lymphocytes │
│ → Establishes latency │
│ ↓ │
│ STEP 2: Environmental carcinogens alter nasopharyngeal │
│ epithelium → premalignant transformation │
│ ↓ │
│ STEP 3: EBV infects premalignant epithelial cells │
│ (Normally, EBV does NOT infect normal NP epithelium)│
│ ↓ │
│ STEP 4: EBV establishes LATENCY TYPE II in epithelial cells │
│ Latent gene products expressed: │
│ • LMP1 (Latent Membrane Protein 1) │
│ • LMP2A/B │
│ • EBNA1 (Epstein-Barr Nuclear Antigen 1) │
│ • EBERs (non-coding RNAs) │
│ • miR-BARTs (viral microRNAs) │
│ ↓ │
│ STEP 5: LMP1 acts as constitutively active CD40 receptor │
│ → Activates NF-κB pathway │
│ → Anti-apoptosis, proliferation, invasion │
│ ↓ │
│ STEP 6: LMP2A mimics BCR signaling → cell survival │
│ EBNA1 → maintains viral episome in dividing cells │
│ ↓ │
│ STEP 7: Immune escape mechanisms │
│ • Downregulation of MHC class I │
│ • Altered cytokine milieu (IL-10 overexpression) │
│ • PD-L1 upregulation (recent discovery) │
│ ↓ │
│ STEP 8: MALIGNANT NPC established │
└──────────────────────────────────────────────────────────────┘
Evidence for EBV association (Scott-Brown's, p.139):
- EBV DNA sequences found in cancer cell nuclei
- 90%+ of Asian NPC cases EBV-positive
- Elevated EBV antibodies (VCA-IgA, EA-IgA) in NPC patients
- EBER (EBV-encoded small RNA) detectable by ISH in cancer cells
- EBV found ONLY in poorly differentiated and undifferentiated NPC
Note: In Caucasian populations, some NPC cases are HPV-positive rather than EBV-positive.
C. ENVIRONMENTAL/DIETARY FACTORS
- Salted fish and preserved foods: The most studied dietary factor. Cantonese-style salted fish contains nitrosamines (particularly dimethylnitrosamine) that are known carcinogens. Early weaning onto salted fish during infancy is associated with highest risk.
- Other preserved foods: Fermented vegetables, salt-preserved meats
- Tobacco smoking: Independent risk factor (Bailey & Love's)
- Occupational exposures: Formaldehyde, wood dust
- Alcohol: Moderate association
SECTION 4: PATHOLOGY AND WHO CLASSIFICATION
Macroscopic Appearance
The tumor may appear as:
- Bulging, exophytic and lobulated mass
- Ulcerative mass
- Submucosal infiltration (no visible tumor - requires blind biopsy)
Most tumors originate in the Fossa of Rosenmuller and spread submucosally.
WHO HISTOLOGICAL CLASSIFICATION (2005, revised 2017)
┌─────────────────────────────────────────────────────────────┐
│ WHO CLASSIFICATION OF NPC │
├─────────────────────────────────────────────────────────────┤
│ │
│ NPC │
│ ├── TYPE 1: KERATINIZING SQUAMOUS CELL CARCINOMA │
│ │ • ~25% in N. America; only 2% in China │
│ │ • Rarely in patients <40 years │
│ │ • Well-defined nests with intercellular bridges │
│ │ • Keratin pearl formation │
│ │ • Desmoplastic stromal response │
│ │ • EBV NEGATIVE │
│ │ • Graded: well/moderately/poorly differentiated │
│ │ │
│ └── TYPE 2: NON-KERATINIZING CARCINOMA (most common) │
│ ├── 2a: DIFFERENTIATED │
│ │ • 12% worldwide; 2% in China │
│ │ • No/little keratinization │
│ │ • Vague intercellular bridges │
│ │ • May undergo cyst formation │
│ │ • No desmoplastic response │
│ │ │
│ └── 2b: UNDIFFERENTIATED (Lymphoepithelioma) │
│ • ~63% worldwide; 95% in China │
│ • MOST COMMON subtype overall │
│ • Most common in children │
│ • Round nuclei, prominent eosinophilic nucleoli │
│ • Dispersed/microvacuolated chromatin │
│ • Scant cytoplasm │
│ • PROMINENT lymphocytic infiltrate (CD8+ T-cells) │
│ • Two growth patterns: │
│ - Regaud: cohesive/nested cells │
│ - Schmincke: non-cohesive/diffuse cells │
│ • EBV POSITIVE (confirmed by EBER-ISH) │
└─────────────────────────────────────────────────────────────┘
Histopathology Images:
H&E staining of NPC - undifferentiated type (a = H&E showing syncytial sheets of malignant cells with lymphocytic infiltrate; b = EBER-ISH showing EBV positivity):
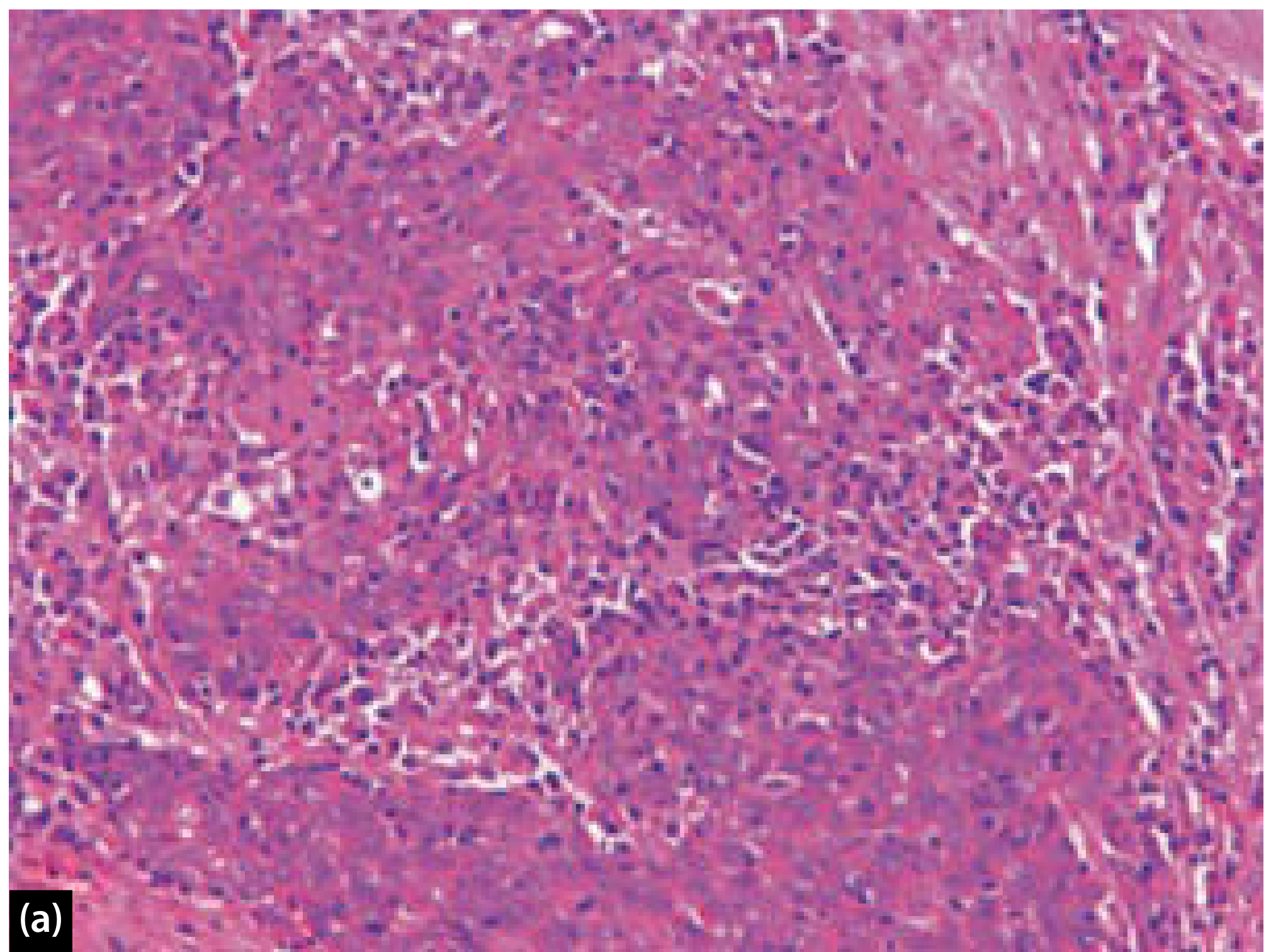
Figure: H&E stain of undifferentiated NPC (WHO Type 2b/lymphoepithelioma). Sheets of poorly differentiated, non-keratinizing malignant cells with ill-defined cytoplasmic borders imparting a syncytial appearance. Small lymphocytes are present within and surrounding the tumor cells. (Scott-Brown's, Fig 26.12)
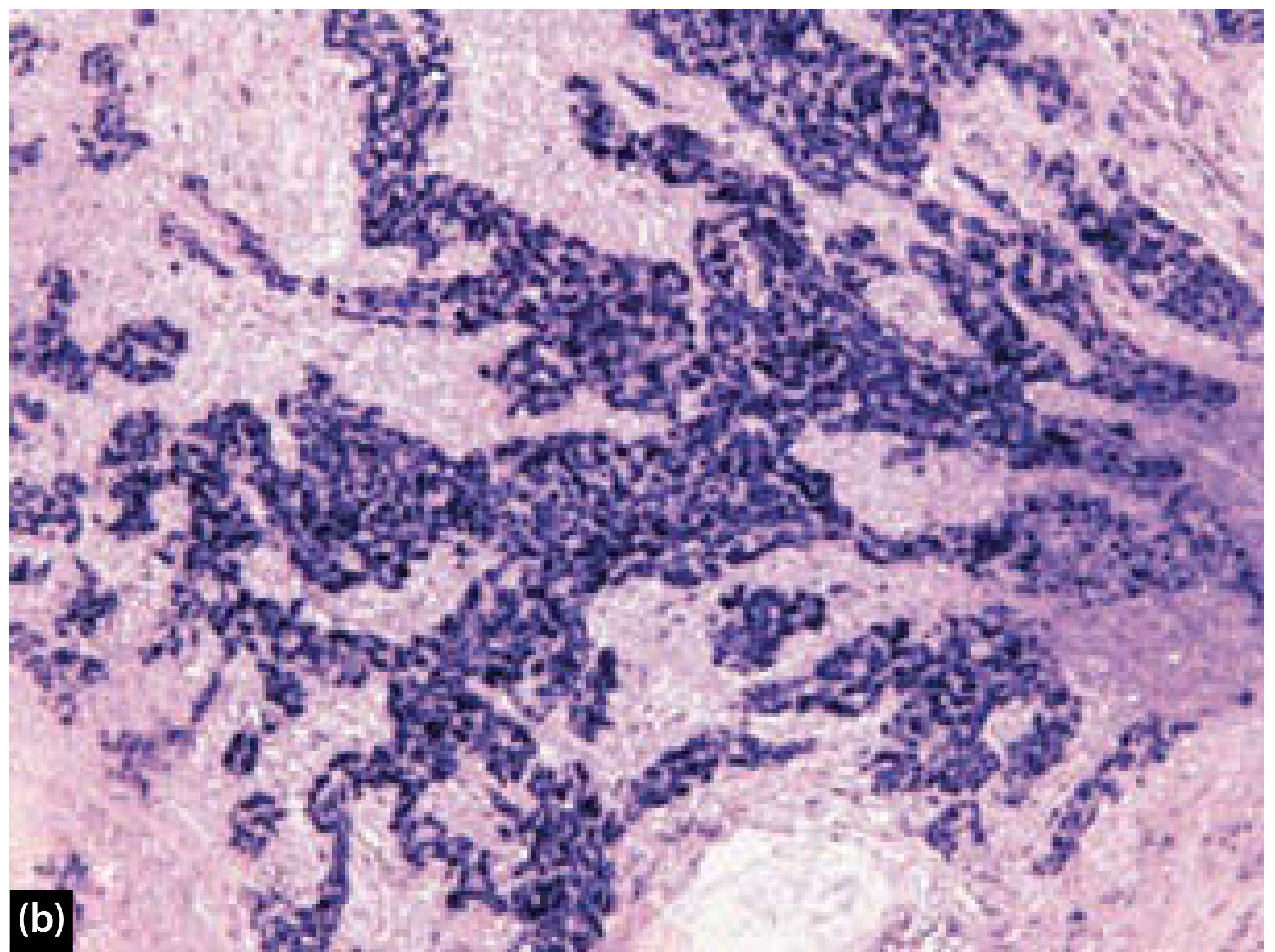
Figure: In situ hybridization (ISH) for EBER confirms diffuse positive signal indicating EBV infection. (Scott-Brown's, Fig 26.12b)
SECTION 5: SPREAD OF NPC
DIRECT SPREAD
┌─────────────────────────────────────────────────────────────────┐
│ DIRECT SPREAD PATTERN OF NPC │
│ (Arising from Fossa of Rosenmuller) │
├─────────────────────────────────────────────────────────────────┤
│ │
│ LATERAL spread (MOST COMMON): │
│ → Parapharyngeal space │
│ → Masticator space │
│ → Mandibular nerve (V3) involvement │
│ → Intracranial spread via foramen ovale │
│ │
│ SUPERIOR spread: │
│ → Skull base erosion (clivus, petrous apex) │
│ → Sphenoid sinus │
│ → Foramen lacerum │
│ → Cavernous sinus → CN III, IV, V, VI palsies │
│ │
│ ANTERIOR spread: │
│ → Nasal cavity │
│ → Maxillary sinus erosion │
│ → Pterygopalatine fossa │
│ → Maxillary nerve (V2) → Foramen rotundum │
│ │
│ INFERIOR spread: │
│ → Along pharyngeal wall │
│ → Oropharynx │
│ │
│ POSTERIOR spread: │
│ → Retropharyngeal space │
│ → Prevertebral muscles │
│ │
│ EUSTACHIAN TUBE obstruction: │
│ → Obstructive secretory otitis media │
└─────────────────────────────────────────────────────────────────┘
LYMPHATIC SPREAD
The nasopharynx has a rich lymphatic network.
LYMPHATIC DRAINAGE PATTERN:
PRIMARY node: Node of ROUVIÈRE (retropharyngeal nodes)
↓
Level II (Upper jugular / Jugulodigastric) ← FIRST PALPABLE node
↓
Level V (Posterior triangle / Spinal accessory chain)
↓
Level III, IV
↓
Bilateral and extensive nodal disease common
Ho's Triangle: Area of highest risk for occult nodal disease
Trotter's Syndrome (Eustachian tube involvement):
- Conductive deafness (OME)
- Palatal palsy (V3 involvement)
- Trismus (pterygoid involvement)
- 60-70% of patients have cervical lymphadenopathy at presentation
- Bilateral nodal disease in 50%
- Hematogenous spread: Bone (vertebrae, pelvis, skull) > Liver > Lung
SECTION 6: CLINICAL FEATURES
NPC is notorious for late presentation because it is hidden in the nasopharynx and the early features are non-specific. The 4 classic symptom groups are:
┌──────────────────────────────────────────────────────────────┐
│ 4 CARDINAL SYMPTOM GROUPS OF NPC │
├──────────────────────────────────────────────────────────────┤
│ │
│ ① NASAL (Anterior tumor extension) │
│ • Nasal obstruction (usually unilateral) │
│ • Epistaxis (blood-stained postnasal drip = CLASSIC) │
│ • Blood-stained nasal discharge │
│ • Post-nasal drip │
│ │
│ ② AURAL (Eustachian tube obstruction) │
│ • Unilateral conductive hearing loss (most common) │
│ • Tinnitus │
│ • Aural fullness │
│ • Serous otitis media / Otitis media with effusion │
│ • Otalgia (referred) │
│ │
│ ③ NECK MASS (Lymph node metastasis) │
│ • Most common PRESENTATION (60-70% at diagnosis) │
│ • Painless, firm, matted nodes │
│ • Bilateral cervical lymphadenopathy │
│ • Level II (first palpable), Level V common │
│ • "Neck mass with unknown primary" → always suspect NPC │
│ │
│ ④ NEUROLOGICAL (Skull base invasion) │
│ • Headache (often persistent, temporal) │
│ • Cranial nerve palsies: │
│ - CN V (trigeminal): facial pain, numbness, trismus │
│ - CN VI (abducens): first CN affected in skull base │
│ - CN III, IV: ophthalmoplegia, ptosis, diplopia │
│ - CN IX, X, XI, XII: Jugular foramen syndrome │
│ (dysphagia, hoarseness, shoulder weakness, tongue Δ) │
│ - CN II: Visual field defect, visual loss │
│ • Proptosis (orbital involvement) │
│ • Cavernous sinus syndrome │
└──────────────────────────────────────────────────────────────┘
TROTTER'S SYNDROME (Classic Triad)
Seen with lateral extension involving the Eustachian tube cushion:
- Unilateral conductive deafness
- Palatal palsy (ipsilateral palatal movement absent)
- Trismus (pterygoid muscle infiltration)
Named Signs
- Ho's Triangle: The triangular area of skull base where NPC commonly erodes (bounded by foramen ovale, foramen spinosum, foramen lacerum)
- Linconi's Highway: Pathway of spread from fossa of Rosenmuller to skull base
- Node of Rouvière: First lymph node involved (retropharyngeal)
SECTION 7: INVESTIGATIONS
┌──────────────────────────────────────────────────────────────┐
│ INVESTIGATION FLOWCHART FOR SUSPECTED NPC │
├──────────────────────────────────────────────────────────────┤
│ │
│ CLINICAL SUSPICION │
│ (Neck mass + aural symptoms + blood-stained PND) │
│ ↓ │
│ STEP 1: NASOPHARYNGOSCOPY │
│ • Rigid 0°/30° endoscope or flexible nasopharyngoscope │
│ • Examine under anesthesia if needed │
│ • Biopsy of suspicious area (sensitivity 70%) │
│ • Blind biopsy of fossa of Rosenmuller if no visible tumor │
│ ↓ │
│ STEP 2: TISSUE DIAGNOSIS │
│ • Punch/forcep biopsy of nasopharyngeal mass │
│ • FNAC of neck node (if neck mass is primary presentation) │
│ • Excision biopsy NOT recommended (may cause dissemination) │
│ • EBER-ISH for EBV confirmation │
│ ↓ │
│ STEP 3: STAGING INVESTIGATIONS │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ MRI HEAD & NECK (GOLD STANDARD for primary tumor) │ │
│ │ • Superior soft tissue delineation │ │
│ │ • Skull base marrow involvement │ │
│ │ • Intracranial/perineural extension │ │
│ │ • Retropharyngeal nodes (better than PET-CT) │ │
│ ├─────────────────────────────────────────────────────┤ │
│ │ CT SCAN │ │
│ │ • Bone erosion of skull base/clivus │ │
│ │ • Neck nodes + chest + liver/abdomen in one exam │ │
│ ├─────────────────────────────────────────────────────┤ │
│ │ PET-CT │ │
│ │ • Detection of distant metastases (M staging) │ │
│ │ • Superior for cervical node staging │ │
│ │ • Identification of unknown primary │ │
│ │ • Intratumoral heterogeneity (SUV correlates with │ │
│ │ prognosis - Huang et al.) │ │
│ │ RECOMMENDATION (Ng et al.): │ │
│ │ MRI + PET-CT as initial staging │ │
│ ├─────────────────────────────────────────────────────┤ │
│ │ EBV SEROLOGY │ │
│ │ • VCA-IgA (viral capsid antigen): most sensitive │ │
│ │ screening test, high titre diagnostic │ │
│ │ • EA-IgA (early antigen): high titre = poor prognosis│ │
│ │ • EBNA-IgG │ │
│ │ • Plasma EBV DNA: most useful for monitoring │ │
│ │ treatment response and recurrence detection │ │
│ └─────────────────────────────────────────────────────┘ │
│ ↓ │
│ STEP 4: ADDITIONAL INVESTIGATIONS │
│ • Audiometry (conductive/mixed hearing loss baseline) │
│ • Dental evaluation (pre-RT assessment) │
│ • Thyroid function (pre-RT baseline) │
│ • Full blood count, renal/liver function (pre-chemo) │
└──────────────────────────────────────────────────────────────┘
CT showing NPC with Eustachian tube obstruction:
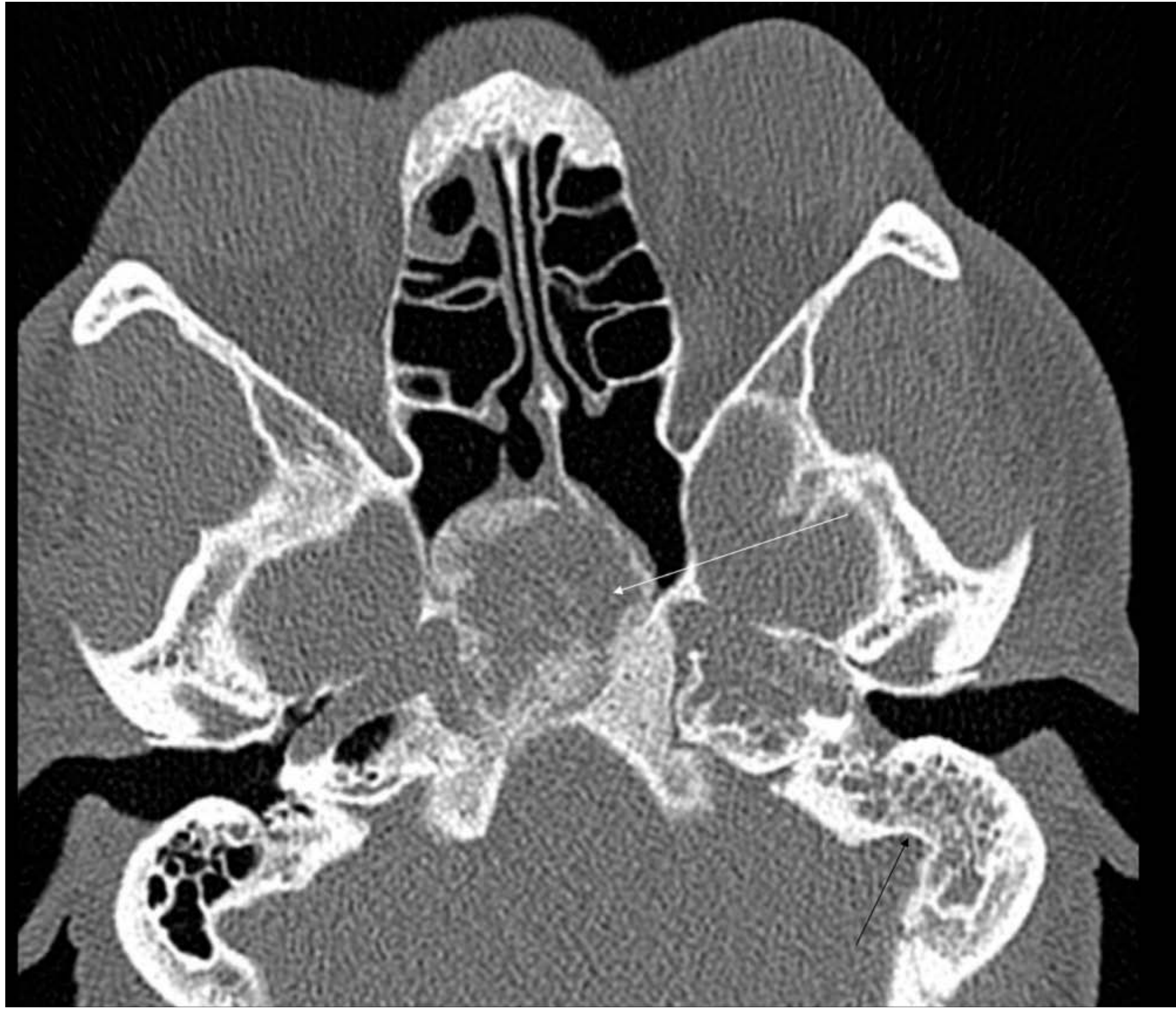
Figure: Axial CT on bone settings showing nasopharyngeal carcinoma (white arrow) and retained secretions in the left mastoid air cells (black arrow) due to Eustachian tube obstruction. (Scott-Brown's, Fig 37.5)
SECTION 8: STAGING - TNM (AJCC/UICC 8th Edition)
T - Primary Tumor
| Stage | Description |
|---|---|
| T0 | No evidence of primary (EBV+ nodes only) |
| Tis | Carcinoma in situ |
| T1 | Confined to nasopharynx OR extends to oropharynx/nasal cavity without parapharyngeal extension |
| T2 | With parapharyngeal extension and/or involvement of medial pterygoid, lateral pterygoid, prevertebral muscles |
| T3 | Bony structures of skull base, cervical vertebra, pterygoid structures, paranasal sinuses |
| T4 | Intracranial extension, CN involvement, hypopharynx, orbit, parotid, soft tissue of neck beyond lateral surface of lateral pterygoid |
N - Regional Nodes
| Stage | Description |
|---|---|
| N0 | No regional nodes |
| N1 | Unilateral cervical ≤6cm, above caudal border of cricoid; AND/OR bilateral/unilateral retropharyngeal ≤6cm |
| N2 | Bilateral cervical ≤6cm, above caudal border of cricoid |
| N3 | Cervical nodes >6cm OR extension below caudal border of cricoid |
M - Distant Metastasis: M0 = no distant mets; M1 = distant metastasis
Overall Stage Grouping
| Stage | T | N | M |
|---|---|---|---|
| I | T1 | N0 | M0 |
| II | T0-1, T2 | N1; N0-N1 | M0 |
| III | T0-2, T3 | N2; N2; N0-N2 | M0 |
| IVA | T4 | N0-N2 | M0 |
| IVB | Any T | N3 | M0 |
| IVC | Any T | Any N | M1 |
SECTION 9: MANAGEMENT
TREATMENT PHILOSOPHY
NPC is among the most radiosensitive of all head and neck carcinomas, particularly the non-keratinizing/undifferentiated type. Radiotherapy is the cornerstone of treatment. Surgery plays a very limited primary role due to:
- Deep, inaccessible location of nasopharynx
- Proximity to critical neurovascular structures
- Excellent response to radiation
┌──────────────────────────────────────────────────────────────┐
│ TREATMENT ALGORITHM FOR NPC (FLOWCHART) │
├──────────────────────────────────────────────────────────────┤
│ │
│ CONFIRMED NPC DIAGNOSIS + STAGING │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ STAGE I (T1N0M0) │ │
│ │ │ │
│ │ RT ALONE (IMRT preferred) │ │
│ │ Dose: 70 Gy to GTV (primary) │ │
│ │ 59.4-63 Gy to CTV (high-risk subclinical) │ │
│ │ 50-56 Gy to neck (prophylactic) │ │
│ │ 5-year OS: 85-90% │ │
│ └─────────────────────────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ STAGE II (T2N0-1 or T1N1) │ │
│ │ │ │
│ │ CONCURRENT CHEMORADIOTHERAPY (CCRT) │ │
│ │ Cisplatin 100mg/m² every 3 weeks OR │ │
│ │ Cisplatin 40mg/m² weekly │ │
│ │ + IMRT 70 Gy │ │
│ │ 5-year OS: 70-80% │ │
│ └─────────────────────────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ LOCALLY ADVANCED (Stage III-IVB) │ │
│ │ │ │
│ │ INDUCTION CHEMO → CCRT → ADJUVANT CHEMO │ │
│ │ │ │
│ │ Induction: Gemcitabine + Cisplatin (GemCis) ×3 │ │
│ │ OR TPF (Docetaxel+Cisplatin+5FU) │ │
│ │ ↓ │ │
│ │ CCRT: Cisplatin + IMRT 70 Gy │ │
│ │ ↓ │ │
│ │ Adjuvant (if indicated): Cisplatin + 5-FU ×3 │ │
│ │ OR Capecitabine (oral) │ │
│ │ │ │
│ │ 5-year OS: 50-70% │ │
│ └─────────────────────────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ STAGE IVC (Distant Metastasis) │ │
│ │ │ │
│ │ PALLIATIVE SYSTEMIC THERAPY │ │
│ │ • Gemcitabine + Cisplatin (first-line standard) │ │
│ │ • Add PD-1 inhibitor (Camrelizumab/Sintilimab) │ │
│ │ → SIGNIFICANT benefit (2024 meta-analysis PMID │ │
│ │ 37227161, Laryngoscope 2024) │ │
│ │ • Palliative RT for symptomatic sites │ │
│ │ Median OS: 12-24 months │ │
│ └─────────────────────────────────────────────────────┘ │
└──────────────────────────────────────────────────────────────┘
A. RADIOTHERAPY IN DETAIL
Intensity-Modulated Radiation Therapy (IMRT) has become the gold standard for NPC treatment. It allows:
- High-dose delivery to tumor while sparing critical structures
- Reduced xerostomia (parotid glands outside high-dose field)
- Better local control rates
- Reduced rates of radiation retinopathy, blindness, brainstem injury
IMRT plan for T4N2 NPC - coronal view:
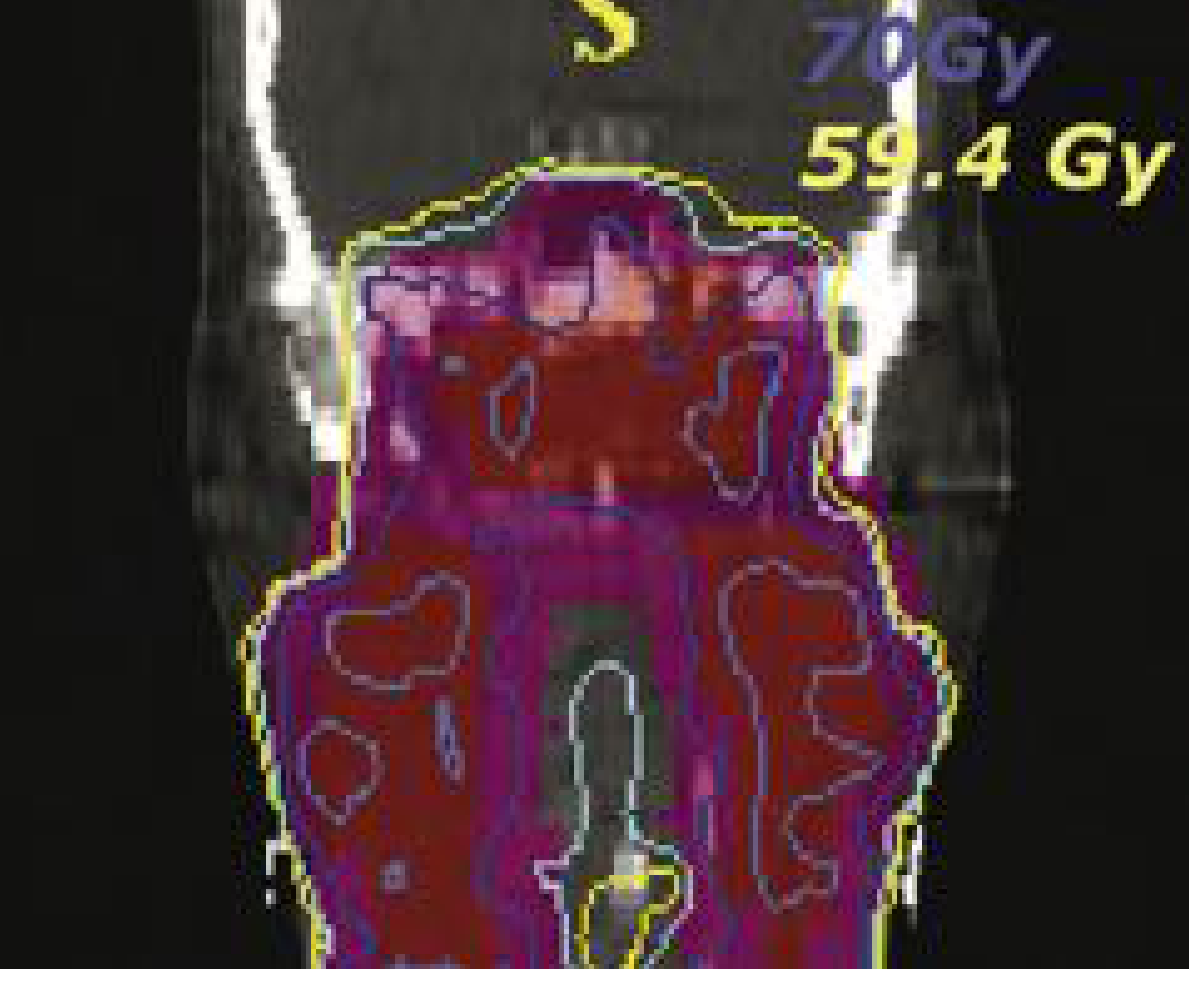
Figure: IMRT coronal plan for T4N2 NPC. Red area = GTV (70 Gy); Magenta = high-risk CTV (59.4 Gy). Notice parotid glands are outside high-dose regions (mean dose <28 Gy). (Cummings, Fig. 117.10)
IMRT Dose Prescription (standard):
- GTV (primary + nodes): 70 Gy in 35 fractions
- High-risk CTV: 59.4-63 Gy
- Low-risk CTV/prophylactic neck: 50-56 Gy
Results of IMRT (from Cummings, Table 117.15):
- Local progression-free survival: 93-97%
- Loco-regional control: 95-98%
- RTOG 0225 trial: 2-year loco-regional control 90% in multi-institutional setting
- Hong Kong Cancer Registry (3328 patients): validated IMRT outcomes
B. CHEMOTHERAPY
Landmark Trial: Al-Sarraf et al. (Intergroup 0099) - Concurrent cisplatin with RT followed by adjuvant cisplatin + 5-FU significantly improved OS versus RT alone (76% vs 46% at 3 years).
Current standard regimens:
- Concurrent: Cisplatin 100mg/m² q3 weeks × 3 cycles during RT (preferred) OR weekly cisplatin 40mg/m²
- Induction (for N2-3 or T3-4): Gemcitabine (1000mg/m² d1, d8) + Cisplatin (80mg/m² d1) × 3 cycles - proven to reduce distant metastasis rates
- Adjuvant: Cisplatin + 5-FU × 3 cycles OR Capecitabine (oral metronomic)
C. SURGERY IN NPC
Surgery is generally NOT indicated as primary treatment. However, it plays a role in:
SURGICAL INDICATIONS IN NPC:
┌─────────────────────────────────────────────────────────┐
│ 1. NECK DISSECTION │
│ • Persistent/residual neck disease post-RT (most │
│ common surgical indication) │
│ • Salvage neck dissection (N2-N3 residual disease) │
│ │
│ 2. NASOPHARYNGECTOMY (Salvage surgery) │
│ • Local recurrence after definitive RT │
│ • Approaches: │
│ a. Transpalatal approach │
│ b. Infratemporal fossa approach │
│ c. Midfacial degloving │
│ d. Endoscopic endonasal approach (recent advance) │
│ │
│ 3. BIOPSY │
│ • Punch biopsy of primary for diagnosis │
│ • FNAC of neck nodes │
└─────────────────────────────────────────────────────────┘
D. MANAGEMENT OF RECURRENCE
RECURRENCE MANAGEMENT FLOWCHART:
POST-TREATMENT SURVEILLANCE
(EBV DNA monitoring + Clinical + MRI)
↓
Rising EBV DNA / Symptoms
↓
Confirm with MRI + PET-CT
↓
┌─────────────────────────────────────┐
│ LOCAL RECURRENCE (nasopharynx) │
│ │
│ • Re-irradiation (if >1yr interval) │
│ - IMRT re-irradiation │
│ - Stereotactic RT (SRS/SBRT) │
│ - Proton beam therapy │
│ • Salvage nasopharyngectomy │
│ (endoscopic approach preferred) │
└─────────────────────────────────────┘
OR
┌─────────────────────────────────────┐
│ REGIONAL RECURRENCE (neck nodes) │
│ │
│ • Salvage neck dissection │
│ • Re-irradiation if unresectable │
└─────────────────────────────────────┘
OR
┌─────────────────────────────────────┐
│ DISTANT METASTASIS │
│ │
│ • Systemic chemotherapy │
│ • Immunotherapy (PD-1 inhibitors) │
│ • Targeted therapy │
└─────────────────────────────────────┘
SECTION 10: COMPLICATIONS OF TREATMENT
Acute Side Effects of RT:
- Mucositis, pharyngitis, dysphagia
- Erythema, skin desquamation
- Xerostomia (reduced by IMRT)
- Nausea, fatigue (with cisplatin)
Late Side Effects:
- Xerostomia (salivary gland fibrosis) - chronic, most debilitating
- Trismus (fibrosis of pterygoid muscles)
- Neck fibrosis
- Sensorineural hearing loss (cochlear radiation dose)
- Radiation necrosis of temporal lobe, brainstem
- Osteoradionecrosis of skull base
- Hypothyroidism, Panhypopituitarism (in children)
- Radiation-induced second malignancies (fibrosarcoma, osteosarcoma)
- From Cummings: Grade 3+ late complications = 54% with conventional RT vs 13% with IMRT
SECTION 11: PROGNOSIS
| Stage | 5-Year Overall Survival |
|---|---|
| Stage I | 85-90% |
| Stage II | 75-85% |
| Stage III | 60-70% |
| Stage IVA-B | 40-55% |
| Stage IVC | <20% (with systemic therapy) |
Prognostic factors:
- Stage (most important)
- Histological type (undifferentiated = better response to RT)
- Plasma EBV DNA level (pre-treatment and post-treatment)
- Nodal status and size
- Distant metastases
- SUV on PET-CT (Huang et al.)
SECTION 12: RECENT ADVANCES (2023-2026)
1. Immunotherapy - PD-1/PD-L1 Checkpoint Inhibitors
EBV-driven NPC overexpresses PD-L1, creating an immunosuppressive microenvironment. This makes it ideal for checkpoint inhibitor therapy.
Key evidence (Guven et al., Laryngoscope 2024, PMID 37227161 - Systematic review & meta-analysis):
- Adding PD-1 inhibitors (pembrolizumab, nivolumab, camrelizumab, sintilimab) to first-line chemotherapy significantly improves OS and PFS in advanced NPC
- Camrelizumab + GemCis (CAPTAIN-1 trial): Improved PFS vs GemCis alone in recurrent/metastatic NPC
- Sintilimab + GemCis: Demonstrated significant PFS benefit
Blanchard et al., ESMO Open 2025, PMID 40138744 - Systematic review on individualization of systemic treatment for locoregionally advanced NPC.
2. Induction Chemotherapy Optimization
A 2025 Bayesian network meta-analysis (Song et al., Am J Otolaryngol, PMID 40578185) showed Gemcitabine + Cisplatin induction followed by CCRT is the optimal combination for locally advanced NPC, superior to TPF or PF induction.
3. IMRT Radiotherapy Target Volume Guidelines (2025)
The Lancet Oncology 2025 joint guidelines (Tang et al., Lancet Oncol, PMID 40907526) from CSTRO, CACA, CSCO, HNCIG, ESTRO, and ASTRO jointly provide contouring atlas for primary target volume delineation in NPC - marking a landmark international consensus.
4. EBV DNA as Liquid Biopsy
- Plasma EBV DNA used for:
- Screening in endemic populations
- Treatment response monitoring
- Early detection of recurrence (rising levels prompt imaging before clinical relapse)
- More sensitive and specific than conventional EBV serology
5. Proton Beam Therapy
- Allows even greater dose conformality
- Further spares brainstem, temporal lobes, cochlea
- Particularly useful in reirradiation of recurrent NPC
- Scott-Brown's (Vol 2): Proton beam becoming routine practice in the UK for NPC in children
6. Endoscopic Salvage Nasopharyngectomy
- Minimally invasive approach via endoscopic endonasal route
- For small local recurrences after primary RT
- Lower morbidity compared to open approaches
- Used increasingly in specialized centers
7. Targeted Therapy
- EGFR overexpressed in NPC → Cetuximab (anti-EGFR) studied in trials
- Anti-EBV LMP1 antibodies and LMP1-ALIX axis targeting (emerging, PMID 39402748)
- EBV-specific adoptive T-cell therapy (experimental)
8. Artificial Intelligence in RT Planning
- Deep learning algorithms for automated contouring
- AI-guided adaptive radiotherapy to account for tumor regression during treatment
SECTION 13: DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|---|
| Angiofibroma | Young males, epistaxis, no nodes, CT shows intense enhancement |
| NK/T-cell lymphoma | Midline destructive, necrosis, negative EBV EBER in epithelial cells |
| Adenoid hypertrophy | Children, no nodes, benign on biopsy |
| Chordoma | Arises from clivus, slower growing, BRACHYURY+ |
| Lymphoma (NHL) | Symmetric, homogenous enhancement, Waldeyer's ring involvement |
| Metastatic nodes (unknown primary) | Requires blind NP biopsy + imaging |
SECTION 14: SUMMARY FLOWCHART
SUSPECTED NPC
(Blood-stained PND + unilateral hearing loss + neck mass)
↓
NASOPHARYNGOSCOPY + BIOPSY
(Blind biopsy of fossa of Rosenmuller if no visible tumor)
↓
HISTOPATHOLOGY (WHO classification)
+ EBER-ISH for EBV
↓
STAGING: MRI Head & Neck + PET-CT + EBV DNA
↓
├── Stage I → IMRT alone (70 Gy)
│
├── Stage II → CCRT (Cisplatin + IMRT)
│
├── Stage III-IVB → Induction GemCis ×3
│ → CCRT (Cisplatin + IMRT)
│ → Adjuvant (if residual risk)
│
└── Stage IVC → Palliative GemCis + PD-1 inhibitor
↓
POST-TREATMENT SURVEILLANCE
(3-monthly for 2 years, then 6-monthly × 3 years, yearly thereafter)
EBV DNA + Clinical + MRI/PET-CT if residual suspected
↓
RECURRENCE DETECTED
├── Local recurrence → Re-IMRT / SBRT / Salvage nasopharyngectomy
├── Regional recurrence → Salvage neck dissection
└── Distant → Systemic therapy ± immunotherapy
REFERENCES FROM PRESCRIBED TEXTBOOKS
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th Ed, Gleeson) - Vol 1 Chapter 8 "Nasopharyngeal Carcinoma" pp. 138-156; Vol 2 Chapter 26 "Pathology of malignant nasopharyngeal tumours" pp. 478-482; Vol 2 Chapter 37 "Imaging in head and neck cancer" pp. 653-660
- Cummings Otolaryngology Head and Neck Surgery (7th Ed) - Chapter 117 "Radiation Management of Nasopharyngeal Carcinoma" pp. 2277-2281
- Bailey & Love's Short Practice of Surgery (28th Ed) - Chapter 52 "Nasopharyngeal carcinoma" pp. 805-808
- Robbins & Kumar Basic Pathology / Robbins Pathologic Basis of Disease - Chapter on Oral Cavity & Upper Respiratory Tract: Nasopharyngeal Carcinoma, pp. 877-881
- Dhingra's Diseases of Ear, Nose & Throat (standard Indian reference): NPC Chapter - epidemiology, EBV, clinical features, staging, and management
- Hazarika's Textbook of ENT & HNS (standard RGUHS reference): NPC - endemic distribution, WHO classification, spread, treatment with RT
- Stell & Maran's Textbook of Head and Neck Surgery - NPC chapter covering Trotter's syndrome, lymphatic spread, radiotherapy technique
Recent PubMed Sources:
- Guven DC et al. Laryngoscope 2024 (PMID 37227161) - Immunotherapy meta-analysis
- Blanchard P et al. ESMO Open 2025 (PMID 40138744) - Individualization of systemic therapy
- Tang LL et al. Lancet Oncol 2025 (PMID 40907526) - International RT contouring guidelines
- Song Z et al. Am J Otolaryngol 2025 (PMID 40578185) - Network meta-analysis on combination treatment
MARKS ALLOCATION GUIDE (RGUHS 50-Mark Pattern)
| Section | Suggested Marks |
|---|---|
| Introduction + Anatomy | 2 |
| Epidemiology | 2 |
| Etiopathology (Genetic + EBV + Environmental) | 8 |
| Pathology (WHO Classification + Histology) | 6 |
| Spread + Clinical Features (4 symptom groups) | 8 |
| Investigations (Endoscopy + Biopsy + Imaging + EBV) | 6 |
| TNM Staging | 5 |
| Management (RT + Chemo + Surgery) | 10 |
| Complications of Treatment | 2 |
| Prognosis | 1 |
| Recent Advances | 4 |
| Diagrams/Flowcharts | Bonus/within above |
| TOTAL | 50 |
Key Points to Remember for RGUHS Exam:
- Fossa of Rosenmuller = commonest site of origin
- WHO Type 2b (Undifferentiated) = most common histology in endemic areas; EBV-associated
- Most common presentation = cervical lymphadenopathy (painless)
- Trotter's syndrome (triad: deafness + palatal palsy + trismus)
- First lymph node = Rouvière (retropharyngeal); First palpable = Level II (jugulodigastric)
- EBV markers: VCA-IgA (screening), Plasma EBV DNA (monitoring)
- IMRT = Gold standard radiotherapy; 70 Gy to primary
- Concurrent cisplatin = added for Stage II and above
- Surgery = only for salvage (residual neck or local recurrence)
- Recent advance: PD-1 inhibitors (immunotherapy) for recurrent/metastatic NPC
This is a shared conversation. Sign in to Orris to start your own chat.