Parkinson’s explain in detail
Reading File
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the detailed answer.
Parkinson's Disease - A Comprehensive Overview
1. Definition and Epidemiology
Parkinson's disease (PD) is the second most common neurodegenerative disorder after Alzheimer's disease. It is characterized by a progressive hypokinetic movement disorder caused by loss of dopaminergic neurons from the substantia nigra pars compacta. More than 10 million people worldwide are affected. Symptoms typically emerge between ages 55 and 65. Men are 1.5 times more likely than women to develop the disease. - Guyton & Hall Textbook of Medical Physiology
The disorder was first formally described by James Parkinson in 1817 in his "Essay on the Shaking Palsy." The term "parkinsonism" refers to the broader clinical syndrome (tremor, rigidity, bradykinesia, instability) which can result from various causes, but idiopathic PD accounts for the majority of parkinsonism cases. - Robbins & Kumar Basic Pathology
2. Pathophysiology and Neurochemistry
The Dopaminergic System
The fundamental lesion in PD is the degeneration of pigmented, catecholaminergic neurons in the substantia nigra pars compacta. These neurons project via the nigrostriatal pathway to the caudate nucleus and putamen (collectively the striatum), where they release dopamine. Dopamine is an inhibitory neurotransmitter in this circuit.
When dopaminergic neurons are lost:
- The caudate nucleus and putamen become overactive
- Continuous excitatory signals are sent to the corticospinal motor control system
- This excessive excitation leads to rigidity and other motor symptoms
- Feedback circuits begin to oscillate due to loss of inhibitory control, causing the characteristic tremor
Dopamine also acts on the nucleus accumbens (limbic system), and its depletion there may reduce the psychic drive for motor activity, contributing to akinesia. - Guyton & Hall
Basal Ganglia Circuit Disruption
PD disrupts both the direct and indirect basal ganglia pathways:
- Direct pathway (facilitatory to movement): dopamine acts on D1 receptors, normally promoting movement
- Indirect pathway (inhibitory to movement): dopamine acts on D2 receptors, normally suppressing unwanted movements
- Loss of dopamine causes the subthalamic nucleus (STN) to become hyperactive because of reduction of GABA influence - Adams & Victor's Principles of Neurology
- This subthalamic overactivity drives excessive inhibitory output from the globus pallidus internus (GPi) to the thalamus, suppressing motor cortex activity
3. Pathology
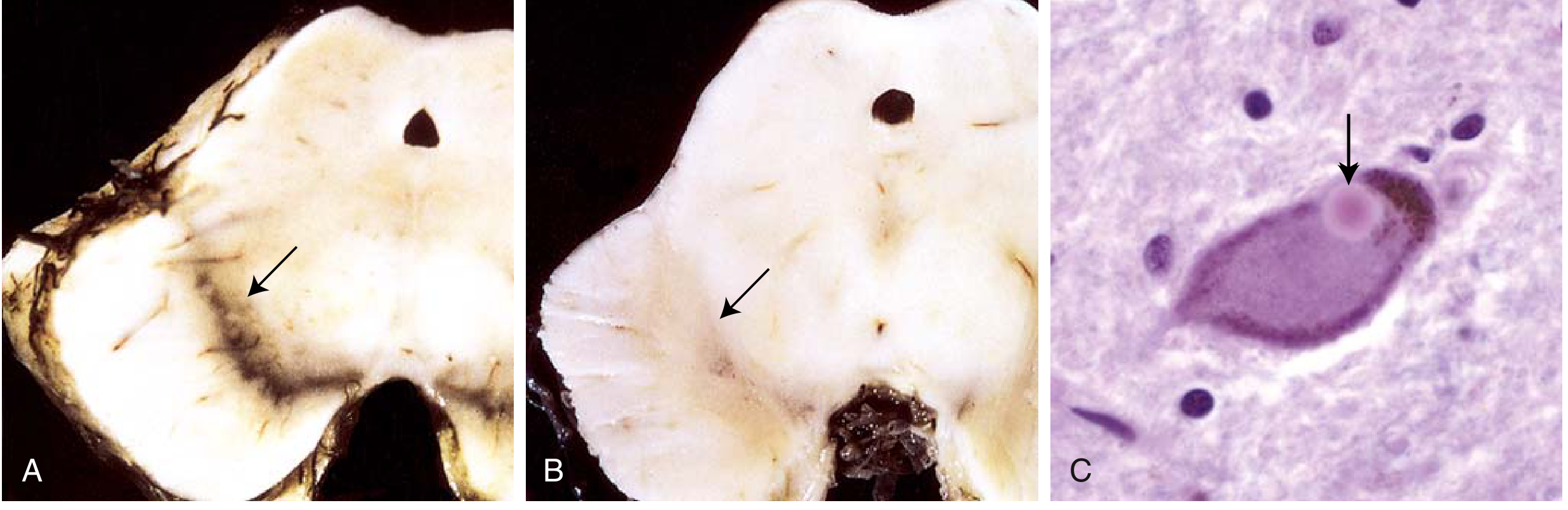
Gross Pathology
- Pallor of the substantia nigra and locus coeruleus (visible to the naked eye due to loss of melanin-containing neurons)
- Normal substantia nigra appears dark/black; in PD it appears pale or grey
Microscopic Pathology
The hallmark finding is the Lewy body - a round to elongated, eosinophilic, cytoplasmic inclusion found in surviving neurons. Ultrastructurally, Lewy bodies consist of:
- Fine filaments of alpha-synuclein (α-synuclein)
- Neurofilaments
- Ubiquitin
- Associated with Lewy neurites - dystrophic neuritic processes also containing aggregated α-synuclein - Robbins & Kumar Basic Pathology
Alpha-Synuclein: The Core Protein
Alpha-synuclein is normally a soluble, unfolded synaptic protein. In PD, it misfolds and aggregates into filaments. The mechanisms include:
- Gene mutations (A53T, A30P) that promote oligomerization
- Gene duplication/triplication increasing protein levels
- Defects in autophagy, lysosomal degradation, and the ubiquitin-proteasome system (parkin mutations)
- The protofibrillary form of α-synuclein is directly toxic to dopaminergic neurons
- Dopamine itself can bind to synuclein, enhancing protofibril formation - Adams & Victor's Principles of Neurology
Neuronal loss also occurs in the enteric nervous system, dorsal motor nucleus of the vagus, and reticular formation - often even before nigral involvement - explaining many non-motor symptoms. - Robbins
4. Genetics
Most PD is sporadic; only ~5% are monogenic. Key genes:
| Gene (Protein) | Inheritance | Age of Onset | Lewy Bodies | Special Notes |
|---|---|---|---|---|
| SNCA (α-synuclein) | AD | 30-40 years | Yes | Mutations A53T, A30P; also gene duplication |
| PARK2 (Parkin) | AR | 20-40 years | No | 50% of familial early-onset cases; excellent L-dopa response |
| LRRK2 (Dardarin) | AD | Late onset | Yes | Most common dominant mutation (G2019S); 1% of sporadic cases; common in Ashkenazi Jewish and North African populations |
| PINK1 | AR | Early onset | Yes | Codes for mitochondrial kinase |
| DJ-1 | AR | Early onset | - | Essential for neuronal response to oxidative stress |
- Adams & Victor's Principles of Neurology
GBA gene (glucocerebrosidase): heterozygosity for Gaucher disease-causing mutations is a significant risk factor, present in ~7% of patients with fully sequenced genes; more common among Ashkenazi Jews - Robbins & Kumar; Adams & Victor's
5. Etiology and Risk Factors
- Genetic factors (as above)
- Environmental toxins: pesticides (organophosphates), industrial chemicals; agrarian/industrialized exposure is slightly more frequent in some studies
- MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine): a synthetic heroin contaminant that selectively destroys the substantia nigra, serving as a neurotoxin model
- Mitochondrial dysfunction: implicated via PINK1 mutations and iron deposition in substantia nigra
- Oxidative stress: dopaminergic neurons are especially vulnerable
- Age is the strongest risk factor; male sex also increases risk
6. Clinical Features
Motor Symptoms (The Classic Tetrad)
- Tremor - "pill-rolling" resting tremor, 3-6 cycles/sec, present at rest, diminishes with intentional movement (unlike cerebellar tremor). It is involuntary throughout waking hours.
- Bradykinesia/Akinesia - slowness and difficulty initiating movement. Often the most disabling symptom; patients must exert extreme mental effort for even simple movements, which then occur in a stiff, staccato manner.
- Rigidity - "cogwheel" or "lead-pipe" rigidity of muscles throughout the body. Due to excessive excitatory output to the motor system.
- Postural instability - impaired postural reflexes leading to poor balance and falls. Appears later in the disease. - Guyton & Hall; Robbins
Additional motor features:
- Shuffling gait with reduced arm swing; festination (progressive acceleration of steps)
- Hypomimia (masked face)
- Micrographia (small handwriting)
- Hypophonia (soft speech)
- Dysphagia (swallowing difficulty) - present in up to 82% by objective measures
- Postural changes (stooped posture)
Non-Motor Symptoms
Non-motor features are increasingly recognized as equally important:
-
Sleep disturbances - REM sleep behavior disorder (RBD) can precede motor symptoms by years
-
Depression and anxiety - very common; anxiety affects quality of life significantly
-
Autonomic dysfunction - orthostatic hypotension, constipation, urinary urgency/nocturia (38-71% of patients have lower urinary tract symptoms), sexual dysfunction, sialorrhea (drooling)
-
Cognitive impairment/Dementia - emerges in many patients; if within 1 year of motor onset, termed Lewy Body Dementia (LBD)
-
Olfactory loss (hyposmia) - often an early pre-motor symptom
-
Pain and fatigue
-
Guyton & Hall; Bradley & Daroff's Neurology; Robbins
Disease Progression
The disease typically progresses over 10-15 years, eventually producing severe motor slowing approaching near-immobility. Death often results from aspiration pneumonia (due to dysphagia) or trauma from falls. - Robbins
7. Diagnosis
Diagnosis is primarily clinical, based on the presence of the cardinal motor features. No definitive pre-mortem biomarker exists.
Diagnostic criteria (UK Brain Bank / MDS criteria):
- Bradykinesia PLUS at least one of: rest tremor, muscular rigidity
- Response to levodopa supports diagnosis
Investigations are used to exclude other conditions:
-
CT/MRI brain: to rule out vascular parkinsonism, normal pressure hydrocephalus (NPH), structural lesions
-
DaT scan (dopamine transporter SPECT): shows reduced uptake in the striatum; useful in differentiating PD from essential tremor
-
PET with FDG: reduced uptake in striatum
-
Neurologist referral when parkinsonism-plus syndrome is suspected
-
Textbook of Family Medicine 9e
Differential Diagnosis (Parkinsonism-Plus Syndromes)
| Condition | Key Distinguishing Features |
|---|---|
| Progressive Supranuclear Palsy (PSP) | Truncal rigidity, falls, vertical gaze palsy, tau inclusions; minimal L-dopa response |
| Multiple System Atrophy (MSA) | Autonomic failure (orthostatic hypotension), cerebellar ataxia, α-synuclein inclusions in oligodendrocytes |
| Corticobasal Degeneration | Asymmetric motor disturbances, apraxia, tau inclusions in cortex |
| Lewy Body Dementia | Dementia within 1 year of motor onset, visual hallucinations, fluctuating cognition |
| Drug-induced Parkinsonism | History of dopamine antagonists (antipsychotics, metoclopramide); reversible |
| Vascular Parkinsonism | Lower body predominance, no tremor, vascular lesions on MRI |
- Robbins & Kumar; Adams & Victor's
8. Treatment
When to Start
Drug therapy is initiated when symptoms cause functional impairment. Current therapies manage symptoms but do not slow disease progression. - Textbook of Family Medicine 9e
Pharmacotherapy
A. Levodopa + Carbidopa (Gold Standard)
- Levodopa is a dopamine precursor that crosses the blood-brain barrier and is converted to dopamine in surviving nigral neurons
- Given alone, it is rapidly metabolized peripherally to dopamine (which cannot cross the BBB), causing nausea, vomiting, and hypotension
- Carbidopa is a peripheral dopa-decarboxylase inhibitor; combined with levodopa, it prevents peripheral conversion, reducing dose needed and side effects
- Standard starting dose: carbidopa/levodopa 25 mg/100 mg three times daily
- Most effective for bradykinesia and rigidity; limited effect on non-motor symptoms
- Long-term complications: motor fluctuations ("wearing off" between doses), "on-off" phenomena, dyskinesias (involuntary movements)
B. Dopamine Agonists
- Pramipexole, ropinirole, rotigotine (patch), apomorphine
- Act directly on striatal dopamine receptors; useful as initial therapy or adjunct to levodopa
- Longer duration of action than levodopa; fewer motor fluctuations initially
- Side effects: excessive daytime sleepiness, impulse control disorders, hallucinations (especially in elderly)
C. MAO-B Inhibitors
- Selegiline, rasagiline
- Inhibit monoamine oxidase type B, which metabolizes dopamine - prolonging its action
- May also slow neurodegeneration (neuroprotective effect debated)
- Used as monotherapy in early disease or adjunct in later disease
- Effective combination with L-dopa for better control
D. COMT Inhibitors
- Entacapone, tolcapone
- Inhibit catechol-O-methyltransferase, another enzyme metabolizing dopamine
- Used as adjuncts to carbidopa/levodopa to prevent motor fluctuations ("wearing off")
- Tolcapone requires liver function monitoring (hepatotoxicity risk)
- Stalevo = carbidopa + levodopa + entacapone in one tablet
E. Anticholinergics
- Trihexyphenidyl (Artane), benztropine (Cogentin)
- Useful primarily for tremor
- Avoid in elderly (impaired memory, urinary retention, blurred vision)
F. Amantadine
- Modest anti-parkinsonian effects; also useful for levodopa-induced dyskinesias
- NMDA glutamate receptor antagonist
Drug Summary Table
| Drug Class | Examples | Primary Use |
|---|---|---|
| L-DOPA combination | Carbidopa/levodopa (Sinemet) | First-line; bradykinesia & rigidity |
| Dopamine agonists | Pramipexole, ropinirole, rotigotine | Early disease; adjunct |
| MAO-B inhibitors | Selegiline, rasagiline | Early or adjunct; neuroprotection |
| COMT inhibitors | Entacapone, tolcapone | Motor fluctuations; adjunct |
| Anticholinergics | Trihexyphenidyl, benztropine | Tremor (younger patients) |
| Amantadine | Amantadine | Mild disease; dyskinesias |
- Textbook of Family Medicine 9e; Guyton & Hall; Neuroanatomy through Clinical Cases
Non-Pharmacological Treatment
- Physical therapy: gait training, balance exercises, strength training. A 2025 network meta-analysis (PMID 39880702) found that exercise meaningfully improves motor symptoms; optimal dose and type vary by outcome
- Virtual reality therapy: 2025 meta-analysis (PMID 40142335) found VR combined with conventional therapy improves balance beyond conventional therapy alone
- Speech therapy: for hypophonia and dysphagia (LSVT-LOUD program)
- Occupational therapy: adaptive strategies, fall prevention
- Nutritional support: addressing dysphagia, constipation
- Management of neuropsychiatric symptoms: cognitive behavioral therapy, pharmacologic management of anxiety (PMID 40568748)
Surgical Treatment: Deep Brain Stimulation (DBS)
DBS is indicated for patients with advanced PD who have motor fluctuations and dyskinesias despite optimal pharmacotherapy. Electrodes are implanted in either the:
- Subthalamic nucleus (STN): slightly larger benefit in medication-off state; may allow larger dopamine medication reductions; higher risk of neuropsychiatric side effects
- Globus pallidus internus (GPi): better dyskinesia suppression, better long-term flexibility, relatively safer neuropsychiatric profile; preferred for "brittle" dyskinesia (occurring at very low medication doses)
Both targets show similar overall motor outcomes. Multiple RCTs have confirmed DBS superiority over best medical therapy for quality of life and motor function. - Bradley & Daroff's Neurology in Clinical Practice
Experimental/Emerging Therapies
- Cell transplantation: fetal dopamine-secreting cells transplanted into caudate/putamen (some short-term success); stem cell strategies under investigation
- Alpha-synuclein targeting: immunotherapy approaches attempting to remove α-synuclein aggregates (mostly unsuccessful so far)
- Gene therapy: targeting specific pathways - Adams & Victor's; Guyton & Hall
9. Complications
- Motor fluctuations: "wearing off," "on-off" phenomena
- Levodopa-induced dyskinesias: chorea, dystonia
- Aspiration pneumonia: from dysphagia - leading cause of death
- Falls and fractures: from postural instability
- Dementia: affects a large proportion in later stages
- Depression/anxiety: highly prevalent, affects quality of life
- Autonomic failure: orthostatic hypotension, urinary dysfunction, constipation
- Psychosis/Hallucinations: particularly with dopaminergic medications (and in Lewy Body Dementia)
10. Key Summary Points
| Feature | Detail |
|---|---|
| Core lesion | Loss of dopaminergic neurons, substantia nigra pars compacta |
| Pathologic hallmark | Lewy bodies (α-synuclein filaments) |
| Cardinal symptoms | Resting tremor, bradykinesia, rigidity, postural instability |
| First-line treatment | Carbidopa/levodopa (Sinemet) |
| Advanced disease | Deep brain stimulation (STN or GPi) |
| Leading cause of death | Aspiration pneumonia, trauma from falls |
| Prognosis | Progressive over 10-15 years; no disease-modifying therapy exists |
Sources: Guyton & Hall Textbook of Medical Physiology | Robbins & Kumar Basic Pathology | Adams & Victor's Principles of Neurology, 12e | Bradley & Daroff's Neurology in Clinical Practice | Textbook of Family Medicine 9e | Neuroanatomy through Clinical Cases 3e
This is a shared conversation. Sign in to Orris to start your own chat.