
20260602_101354(1).jpg
is there recession of hairline if yes which grade and how to recover lost hairline
Reading File
Finding Sources
Searching PubMed
androgenetic alopecia treatment hairline restoration
Searching the Web
Norwood Hamilton scale grade II III hairline recession treatment options 2025
Finding Sources
Searching PubMed
androgenetic alopecia finasteride minoxidil treatment
Reading File
Loading Image
Reading File
Now I have all the information needed. Here is my full analysis:
Hairline Assessment
Yes, there is clear hairline recession. Looking at the image, you show bilateral temporal recession with the classic "M-shaped" hairline pattern. The hairline has receded at both corners but the frontal midline tuft is still relatively preserved. There is no significant crown/vertex loss visible from this angle.
Grade: Norwood-Hamilton Scale Type II-III
Comparing your hairline to the Norwood scale below:
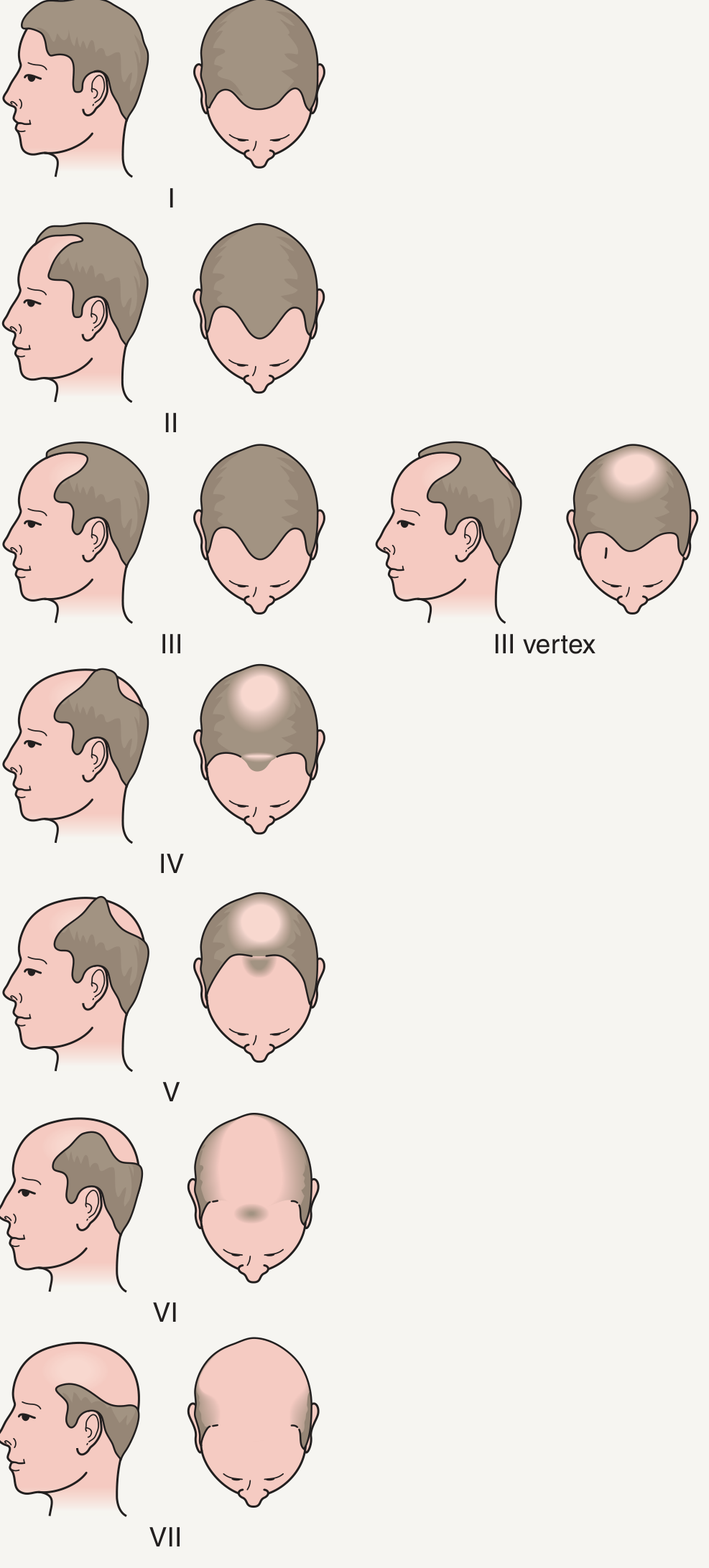
- Type II: Triangular recessions at the frontoparietal (temporal) regions - this matches your image closely
- The recession depth and pattern put you closer to Type II-III, meaning early-to-moderate androgenetic alopecia (AGA)
This is actually a favorable stage - early intervention at this point gives the best outcomes for hairline preservation and partial recovery.
How to Recover the Lost Hairline
Treatment works on two fronts: stop further loss and stimulate regrowth. Here is what the evidence supports:
Tier 1: Medical Treatment (First Line - Start Now)
1. Finasteride 1 mg/day (oral)
- Inhibits type II 5-alpha-reductase, blocking conversion of testosterone to DHT in hair follicles
- FDA-approved for male AGA
- In a randomized trial of 1553 men, significantly greater hair counts were observed vs placebo; 90% of patients maintained above-baseline hair counts at 5 years
- Crucially: finasteride also stimulates regrowth of frontal scalp/hairline hairs (not just vertex), making it directly relevant to your pattern
- Works best in men in their mid-twenties with higher DHT levels
- Allow at least 6 months before judging effect
- If stopped, AGA returns to pre-treatment appearance
- Side effects: decreased libido/erectile dysfunction in <2% (vs 1% placebo); rare gynecomastia, depression
(Dermatology 2-Volume Set 5e, p.3160)
2. Topical Minoxidil 5% (twice daily) or Oral Low-Dose Minoxidil (0.625-2.5 mg/day)
- Extends anagen (growth) phase, increases follicle caliber, and has vasodilatory/angiogenic effects
- FDA-approved 5% solution for men 16+
- Growing evidence for oral low-dose minoxidil (0.625-2.5 mg/day) showing safety and efficacy in both male and female pattern hair loss
- Best results when combined with finasteride - a 2025 systematic review (PMID: 41127390) confirms the combination outperforms minoxidil alone
- Side effects: facial/cheek hypertrichosis (especially oral), headache, ankle edema, contact dermatitis (topical)
(Dermatology 2-Volume Set 5e, p.3160)
Combination Therapy (Finasteride + Minoxidil) = Best Non-Surgical Outcome
- 2025 network meta-analysis (PMID: 40586152) confirms 5-alpha-reductase inhibitors and minoxidil have complementary mechanisms; combination is superior
- Research shows 92.4% of patients remain stable or improved at 12 months on combination oral therapy
Tier 2: Adjunct / Supportive Therapies
| Treatment | Role | Evidence |
|---|---|---|
| PRP (Platelet-Rich Plasma) | Scalp injections stimulate follicle growth factors; 2026 systematic review (PMID: 41877369) supports benefit | Moderate |
| Low-Level Laser Therapy (LLLT) | FDA-cleared devices; improves follicle metabolic activity | Moderate |
| Microneedling | Stimulates dermal papilla, can be combined with topical minoxidil for enhanced penetration | Mild-moderate |
| Scalp massage | Daily 4-minute massage may alter gene expression regulating hair growth | Low/supportive |
Tier 3: Surgical Option (Permanent Hairline Restoration)
FUE (Follicular Unit Extraction) or DHI (Direct Hair Implantation)
- At Norwood II-III, you are an ideal candidate - strong donor reserves, fewer grafts needed
- Typically 1,500-2,500 grafts sufficient for hairline reconstruction at this stage
- Best done after the hair loss pattern has stabilized (usually after medical therapy for 1-2 years first, to know the final extent)
- Permanent results with natural-appearing hairline
Lifestyle Factors That Accelerate Loss (Address These Too)
- Chronic stress (triggers telogen effluvium)
- Smoking
- Nutritional deficiencies (iron, zinc, vitamin D - get blood levels checked)
- Poor sleep
Recommended Action Plan
- Immediately: Start finasteride 1 mg/day + minoxidil 5% topical (or low-dose oral) - consult a dermatologist/trichologist first
- 3-6 months: Add PRP or LLLT if response is slow
- 12-18 months: Reassess. If stabilized and you want hairline lowering/filling, consider FUE/DHI hair transplant
- Blood work: Check ferritin, vitamin D, zinc, thyroid (TSH) to rule out contributing deficiencies
Note: This assessment is based on visual analysis from a single lateral photo. A dermatologist or trichologist can perform trichoscopy and full scalp examination for a definitive grade and personalized treatment plan. Do not start finasteride without medical supervision, especially if you have any liver disease or are concerned about sexual side effects.
This is a shared conversation. Sign in to Orris to start your own chat.