Umn lesion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Upper Motor Neuron (UMN) Lesion
Definition
The upper motor neuron (UMN) refers to all descending motor pathways from the cerebral cortex to the anterior horn of the spinal cord (or cranial nerve motor nuclei). This includes:
- Corticospinal tract (the direct pathway; runs through the medullary pyramid - also called the pyramidal tract)
- Indirect pathways: rubrospinal, reticulospinal, vestibulospinal, tectospinal tracts
These tracts collectively modulate (and in part, drive) the lower motor neuron (LMN). The terms "corticospinal," "pyramidal," and "upper motor neuron" are not synonymous and should not be used interchangeably - "UMN" is the broadest term.
(Adams and Victor's Principles of Neurology, 12th Ed.)
Anatomy of the Corticospinal Tract
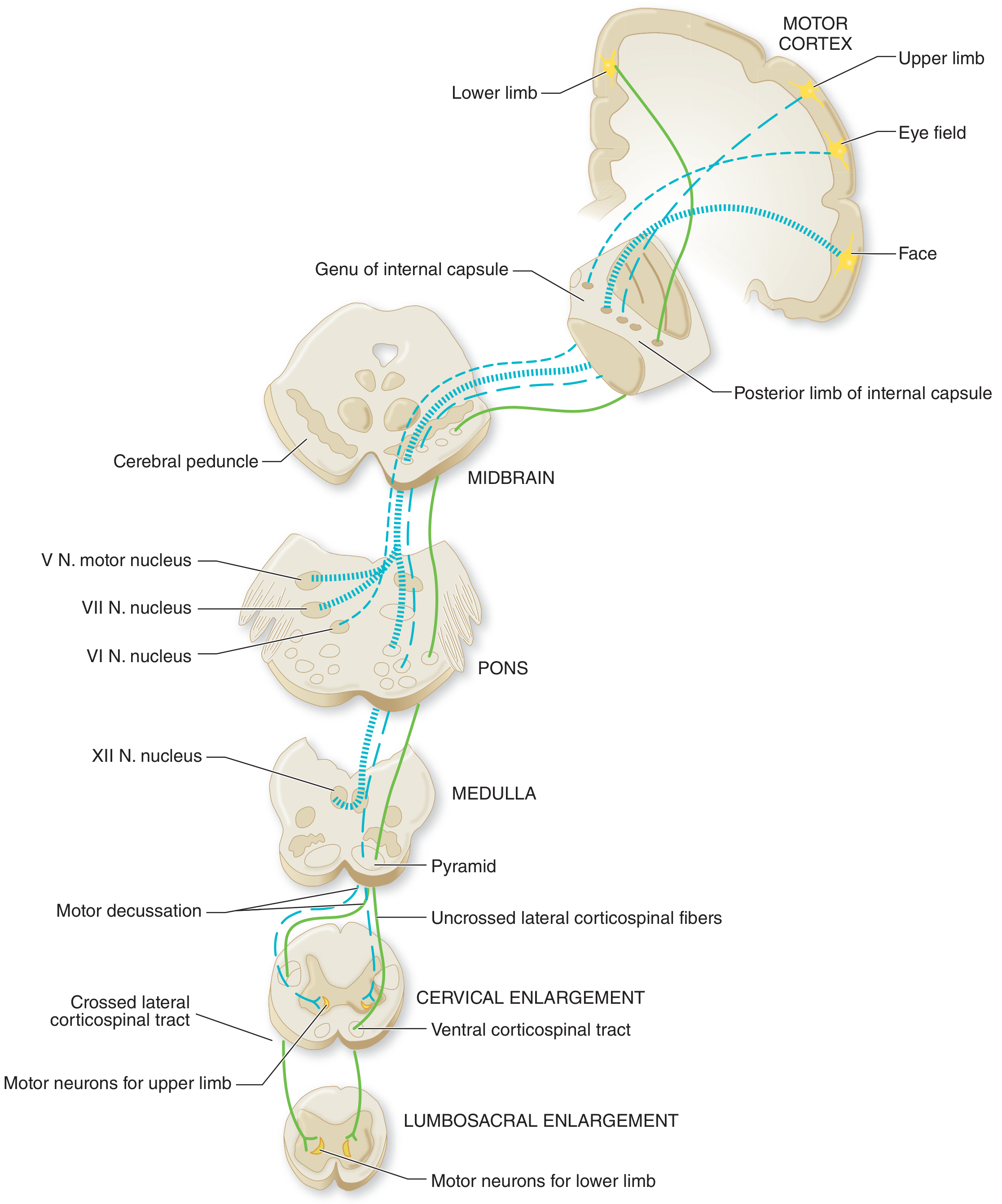
The tract originates from:
- Primary motor cortex (Brodmann area 4) - Betz cells (~30%)
- Premotor/supplementary motor cortex (area 6) - ~30%
- Parietal somatosensory cortex (areas 1, 3, 5, 7) - ~40%
It descends through:
- Corona radiata (subcortical white matter)
- Posterior limb of internal capsule
- Cerebral peduncle (midbrain)
- Basis pontis
- Medullary pyramid
- Motor decussation (lower medulla) - ~85% of fibers cross here
- Lateral funiculus of spinal cord (as the lateral corticospinal tract)
Signs of UMN Lesion
Comparison Table
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Muscle atrophy | Absent (disuse only) | Present (denervation) |
| Fasciculations | Absent | Present |
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Deep tendon reflexes | Increased (hyperreflexia) | Decreased / absent |
| Plantar response (Babinski) | Extensor (upgoing) | Flexor (normal) |
(Neuroanatomy through Clinical Cases, 3rd Ed.; Harriet Lane Handbook, 23rd Ed.)
Note on infants: In infants, UMN lesions paradoxically show decreased tone (because descending tracts are not fully myelinated). An upgoing Babinski is normal until 1-2 years of age.
Key Clinical Features in Detail
1. Weakness
- Affects groups of muscles, never individual muscles
- Bilateral movements (eyes, jaw, pharynx, upper face, diaphragm, abdomen) are largely spared due to bilateral cortical innervation - this is "Broadbent's law" for facial muscles
- Rarely complete and permanent (unlike LMN destruction)
- Upper limb: flexors relatively stronger; lower limb: extensors relatively stronger (explains hemiplegic posture)
2. Spasticity
- Velocity-dependent increase in muscle tone
- Results from loss of descending inhibitory pathways (corticoreticulospinal) rather than pure corticospinal tract damage alone - a pure pyramidal tract lesion does NOT cause spasticity
- Leads to the classic clasp-knife phenomenon
3. Hyperreflexia
- Brisk deep tendon reflexes
- Clonus may be present (rhythmic oscillation at ankle or patella)
- Lost inhibitory control of spinal stretch reflex arcs
4. Babinski Sign (Extensor Plantar Response)
- Stroking the lateral sole causes dorsiflexion of the big toe and fanning of other toes
- Pathognomonic of UMN damage
- Hoffmann's sign (flicking the middle fingernail causes thumb flexion) is the upper limb equivalent
5. Acute UMN Lesion - Spinal Shock
- Important: Immediately after an acute UMN lesion (e.g., stroke, spinal cord injury), the picture is paradoxically flaccid paralysis with hyporeflexia
- This is called spinal shock (below the lesion) or diaschisis (for brain lesions)
- Spasticity and hyperreflexia develop over hours to months as the spinal cord adapts
6. EMG in UMN Lesion
- Normal insertional activity
- No spontaneous activity (no fibrillations/fasciculations)
- Normal MUAP morphology
- Reduced interference pattern due to poor voluntary activation
- Recruitment frequency/ratio is normal (distinguishes from LMN)
(Bradley and Daroff's Neurology in Clinical Practice)
Localization by Level of UMN Lesion
| Site of Lesion | Pattern |
|---|---|
| Motor cortex | Contralateral monoplegia (arm or leg, depending on somatotopy) |
| Internal capsule / corona radiata | Contralateral hemiplegia (arm + leg + lower face) |
| Brainstem above facial nucleus | Contralateral hemiplegia with lower face weakness (upper face spared - bilateral cortical input); ipsilateral CN palsy possible (crossed syndrome) |
| Cervical spinal cord | Ipsilateral arm + leg (hemiplegia if unilateral; quadriplegia if bilateral) |
| Thoracic spinal cord | Ipsilateral leg (paraplegia if bilateral) |
Causes of UMN Lesions
| Category | Examples |
|---|---|
| Vascular | Stroke (ischemic/hemorrhagic), AVM, subdural hematoma |
| Demyelinating | Multiple sclerosis |
| Neoplastic | Brain tumor, spinal cord compression |
| Traumatic | Spinal cord injury, TBI |
| Degenerative | ALS (also has LMN component), primary lateral sclerosis, hereditary spastic paraplegia |
| Infectious/Inflammatory | Abscess, transverse myelitis |
UMN vs LMN - Clinical Mnemonic
UMN = "UPPER" features:
- Upgoing plantar (Babinski+)
- Pyramidal pattern weakness
- Plastic/spastic tone increase
- Exaggerated reflexes
- Rigid (clasp-knife) - no atrophy, no fasciculations
LMN = "LOWER" features (the 3 As):
- Atrophy
- Areflexia
- Atonia + fasciculations
Sources: Adams and Victor's Principles of Neurology, 12th Ed. | Neuroanatomy through Clinical Cases, 3rd Ed. | Bradley and Daroff's Neurology in Clinical Practice | Harriet Lane Handbook, 23rd Ed.
Picture of ant children
Generating Image
cute cartoon ant children playing together, young ants with small backpacks and big eyes, cheerful and colorful illustration
!
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
This is a shared conversation. Sign in to Orris to start your own chat.