Nose bleeding
Reading File
Finding Sources
Searching the Web
epistaxis nosebleed causes management treatment clinical
Searching PubMed
epistaxis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Epistaxis (Nosebleed)
Epistaxis is a very common otolaryngologic complaint. It is rarely life-threatening, but can be distressing and, in a minority of cases, requires emergency management. It has a bimodal age distribution - peaks in children and in the elderly.
Anatomy
The nasal blood supply comes from three arterial territories with rich anastomoses:
| Artery | Origin | Area Supplied |
|---|---|---|
| Sphenopalatine artery | External carotid | Turbinates, posterior and inferior septum |
| Anterior and posterior ethmoidal arteries | Ophthalmic branch of internal carotid | Superior mucosa, medially and laterally |
| Superior labial branch of facial artery | External carotid | Anterior mucosal septum, anterior lateral mucosa |
Kiesselbach's plexus (Little's area) is the rich arterial anastomosis on the anteroinferior nasal septum - the most common bleeding site.
Classification
Anterior Epistaxis (90%)
- Arises from Kiesselbach's plexus
- Common in children and young adults
- Usually unilateral
- Typically self-limited
Posterior Epistaxis (10%)
- Originates from the posterior septum or turbinates
- More common in elderly patients with atherosclerosis or bleeding disorders
- More severe, harder to manage
- May require inpatient monitoring
Causes
Local Causes
- Nose picking (most common in children)
- Nasal trauma / blunt impact
- Upper respiratory infections (mucosal vasodilation)
- Nasal foreign bodies
- Nasal polyps
- Tumours (including juvenile angiofibroma in adolescent boys)
- Granulomatous disorders
- Environmental irritants, cocaine use
- Chronic use of nasal vasoconstrictors
Systemic Causes
- Hypertension (no proven causation, but associated with persistent bleeding)
- Anticoagulants - warfarin, rivaroxaban
- Antiplatelet agents - aspirin, clopidogrel
- Coagulopathies - haemophilia, von Willebrand disease
- Thrombocytopenia, leukaemia
- Hepatic disease / alcoholism
- Vitamin K or folic acid deficiency
- Hereditary Haemorrhagic Telangiectasia (HHT) / Osler-Weber-Rendu disease - recurrent multifocal bleeding from thin-walled vessels lacking muscle and elastic tissue

HHT (Osler's disease) with multiple facial telangiectasias - Bailey & Love's Surgery, 28th Ed.
Clinical Evaluation
History: Timing, frequency, severity; laterality; trauma; medications (anticoagulants, antiplatelets, NSAIDs); bleeding disorders; prior nasal surgery.
Examination:
- Assess airway, hemodynamics, and tissue perfusion first
- Have the patient blow the nose to expel clots, then apply firm bilateral pressure on the cartilaginous part of the nose (not the bony bridge) for 10-15 minutes
- Administer 0.05% oxymetazoline (2 sprays) into the affected naris before applying pressure
- Examine the floor of the nose with the head parallel to the floor (not tilted back)
Labs: Not routinely needed. Order coagulation studies (PT, PTT, INR) and CBC in patients on anticoagulants, severe haemorrhage, suspected liver disease, or haematologic malignancy.
Management
Step 1 - First Aid (all patients)
- Sit upright, lean slightly forward (prevents swallowing blood)
- Compress the cartilaginous nose firmly for 10-15 minutes without releasing
- Topical vasoconstrictor: oxymetazoline or xylometazoline spray
Step 2 - Anterior Epistaxis (if bleeding point identified)
Chemical cautery with a silver nitrate stick:
- Applied from periphery to centre, superior to inferior
- Contact no longer than 15 seconds to avoid septal necrosis
- Never apply bilaterally at the same session (risks septal necrosis)
Topical haemostatic agents: Absorbable gelatin sponge (Gelfoam), Surgicel - if cautery fails.
Topical tranexamic acid: Inhibits fibrinolysis. 500 mg of IV solution applied to a nasal pledget or atomized. Evidence shows it reduces bleeding at 10 minutes and re-bleeding at 7-10 days, particularly effective in patients on antiplatelet drugs. No significant increase in adverse events. - Rosen's Emergency Medicine, 10th Ed.
Step 3 - Anterior Nasal Packing (if above fails)
Options:
- Merocel (polyvinyl acetal nasal tampon) - inserted along the floor of the nose
- Rapid Rhino (inflatable nasal balloon) - procoagulant-coated, moistened before insertion, inflated with air
- Petroleum jelly (Vaseline)-impregnated ribbon gauze - packed posterior to anterior
A 2025 systematic review and meta-analysis (PMID 40546131) found no significant difference in efficacy between Merocel and Rapid Rhino devices.
Note: Routine prophylactic antibiotics with anterior nasal packing are NOT recommended.
Step 4 - Posterior Epistaxis
Suspect when bleeding persists despite proper anterior packing.
- Double balloon catheter device: Posterior balloon inflated first in nasopharynx, then pulled anteriorly and seated; anterior balloon then inflated
- Foley catheter alternative: Inserted into nasopharynx, inflated with 5-7 mL of water
- Requires inpatient monitoring (risk of airway compromise, hypoxia, vagal reactions)
- Elderly patients: nasal packing carries risk of pulmonary/cardiac complications
Step 5 - Refractory / Surgical Cases
For epistaxis not responding to packing:
| Procedure | Notes |
|---|---|
| Endoscopic sphenopalatine artery clipping | Effective for significant refractory epistaxis |
| Internal maxillary artery ligation | Via pterygopalatine fossa (endoscopic access) |
| Anterior/posterior ethmoidal artery ligation | For superior/ethmoidal bleeding |
| External carotid artery ligation | Last resort above the lingual artery |
| Endovascular embolization | Interventional radiology; success rates 91-97%, complication rate 0-3%; preferred over surgery in many centres for posterior bleeding |
Special Situations
Juvenile Angiofibroma: Affects adolescent boys. Highly vascular - do NOT biopsy. Diagnose with contrast CT or MRI (Holman-Miller sign: anterior bowing of the posterior antral wall). Managed with preoperative embolization followed by endoscopic excision.
HHT: Recurrent, multifocal bleeds. Standard packing is often inadequate. Laser photocoagulation, anti-angiogenic therapy (bevacizumab), or septal dermoplasty may be needed.
Paediatric epistaxis (<2 years): Rare - consider non-accidental trauma and bleeding disorders.
Anticoagulated patients: Topical tranexamic acid is particularly effective. Address anticoagulation reversal if appropriate.
When to Refer to ENT / Hospital Admission
- Posterior epistaxis
- Haemodynamic instability or large blood loss
- Failed anterior packing
- Suspected underlying vascular or haematologic disorder
- Juvenile angiofibroma or tumour suspected
Sources: Rosen's Emergency Medicine - Concepts and Clinical Practice, 10th Ed. | Bailey and Love's Short Practice of Surgery, 28th Ed. | Cummings Otolaryngology Head and Neck Surgery | Grainger & Allison's Diagnostic Radiology
Scoliosis explain and ot and pt managment
Reading File
Finding Sources
Searching the Web
scoliosis occupational therapy physical therapy management rehabilitation
Searching PubMed
scoliosis physical therapy rehabilitation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive data from the best orthopaedic, surgical, and neurological textbooks, plus PubMed evidence. Let me now compile the full structured answer.
Scoliosis - Complete Overview with OT and PT Management
Definition
Scoliosis is a three-dimensional spinal deformity - the most visible component is lateral curvature, but it always involves a rotational component as well. It is defined radiologically as a lateral spinal curvature of >10 degrees (Cobb angle). The rotational element is best seen clinically on the Adams forward bend test, where rib asymmetry creates a characteristic rib hump.
Classification
By Aetiology
| Type | Description |
|---|---|
| Idiopathic | No identifiable cause; most common (80%) |
| Congenital | Vertebral segmentation defects (hemivertebrae, block vertebrae, butterfly vertebrae) |
| Neuromuscular | Secondary to cerebral palsy, spinal muscular atrophy (SMA), myelomeningocele, Friedreich's ataxia |
| Syndromic | Marfan syndrome, Ehlers-Danlos, neurofibromatosis, Klippel-Feil |
| Postural | Caused by leg length discrepancy; flexible, corrects on side-bending |
Idiopathic Scoliosis by Age of Onset
| Type | Age of Onset |
|---|---|
| Infantile | <3 years |
| Juvenile | 3-10 years |
| Adolescent | 10-18 years (most common) |
| Adult | Onset at/after skeletal maturity |
Key point: Earlier onset = higher risk of progression. Adolescent idiopathic scoliosis (AIS) is the most common structural type and affects girls more than boys.
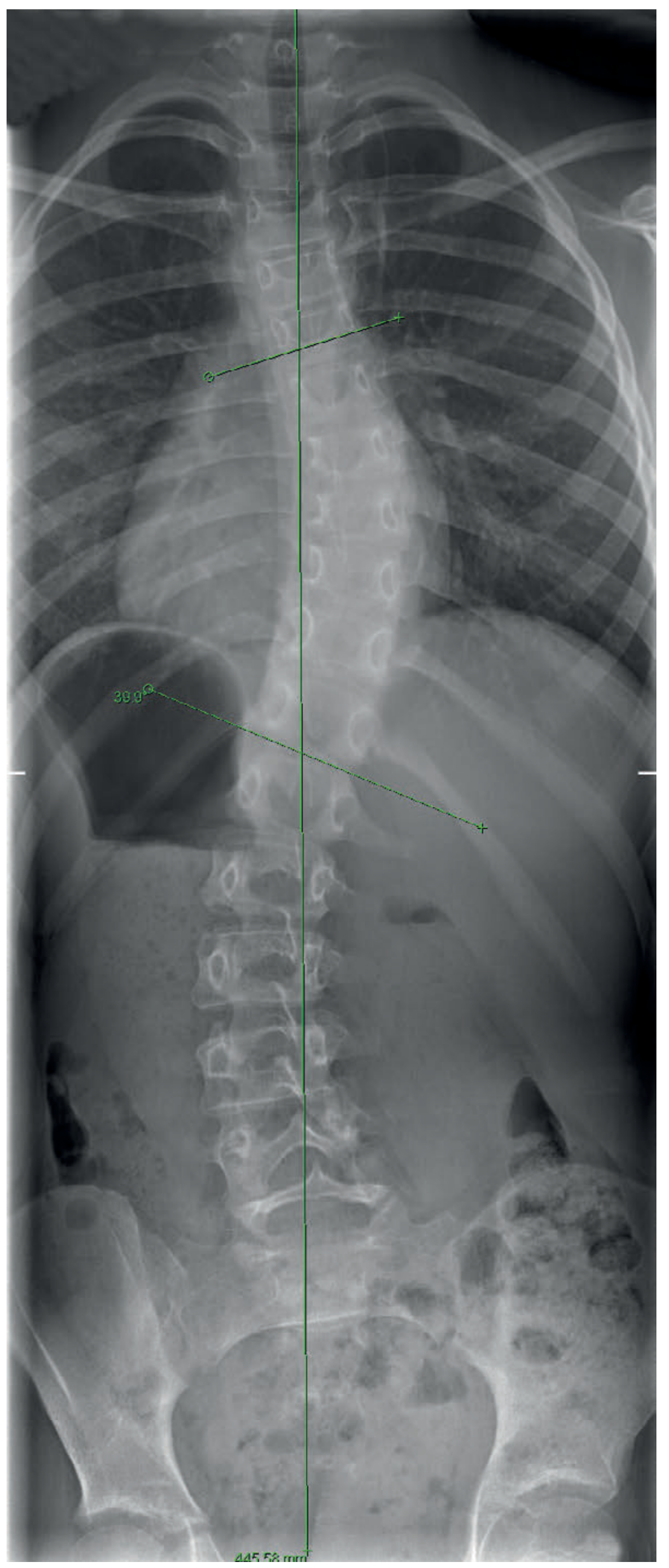
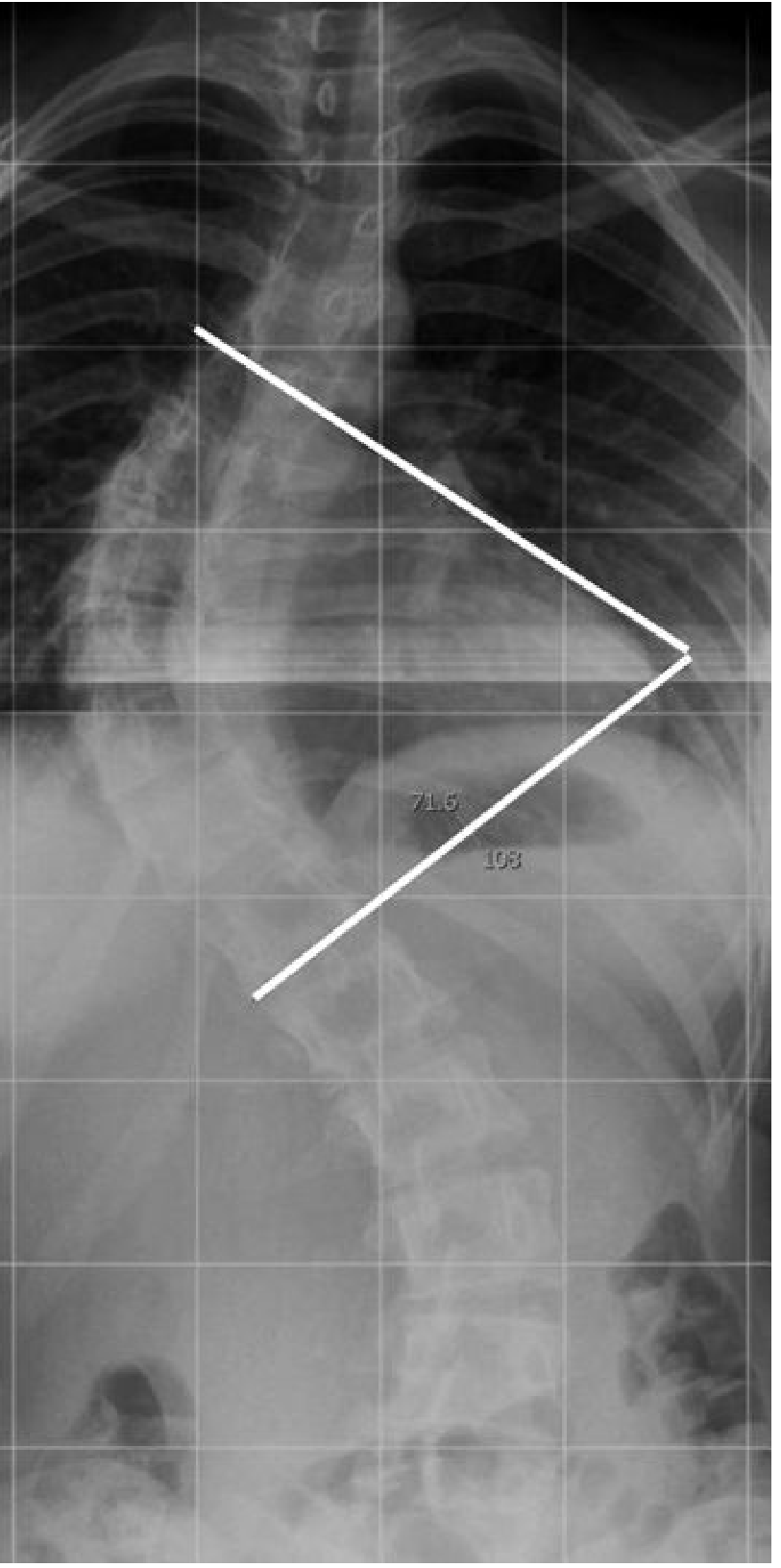
Cobb Angle - Measurement and Clinical Significance
The Cobb angle is the standard radiological measurement of curve severity. It is measured between the superior end plate of the uppermost tilted vertebra and the inferior end plate of the lowermost tilted vertebra.
| Cobb Angle | Management |
|---|---|
| <10° | Normal variant |
| 10-20° | Observation only |
| 20-25° | Observation, monitor for progression |
| 25-40° | Bracing (in growing child with documented progression) |
| 40-50° | Surgery considered (some may still brace) |
| >50° | Surgical indication |
Risk Factors for Curve Progression
- Female sex (worse prognosis)
- Young age at diagnosis (more growth remaining)
- Risser grade 0-2 (iliac crest apophysis - more growth = higher risk)
- Curve magnitude >30 degrees
- Pre-menarchal or <1 year post-menarchal
- Curve progression of ≥5 degrees on two or more visits
Idiopathic scoliosis of >10 degrees occurs in 2-3% of children under 16. Larger curves (>30 degrees) are much rarer at 0.15-0.3%.
Clinical Features
- Usually painless - pain in scoliosis should raise suspicion for tumour or infection
- Visible trunk asymmetry, shoulder height difference, waist asymmetry
- Rib hump on Adams forward bend test
- Back pain may occur in lumbar or thoracolumbar curves
- Large curves (>60 degrees) cause restrictive pulmonary impairment and reduced vital capacity
- ~10% of patients have neurologic abnormality
Investigations
- Standing PA radiograph (full spine) - for Cobb angle, Risser grade
- Adams forward bend test + scoliometer - rib hump measurement (trunk rotation angle)
- MRI - indicated if: left thoracic curve, pain, abnormal neurological exam, atypical findings - to exclude syringomyelia, tethered cord, tumour
- CT - for complex congenital vertebral anomalies
Treatment Overview
Nonoperative
The two most widely accepted nonoperative techniques are observation and bracing, ideally combined with Schroth-based physical therapy. Manipulation, electrical stimulation, and generic physical therapy alone have no scientific evidence of effectiveness for idiopathic scoliosis.
Physical Therapy (PT) Management
1. Physiotherapeutic Scoliosis-Specific Exercises (PSSE)
The Society on Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT) endorses PSSE as a mainstay alongside bracing. The most evidence-based approach is the Schroth Method.
Schroth Method
- A 3D approach developed specifically for scoliosis
- Uses rotational angular breathing, postural correction, and muscular co-contraction
- Aims to elongate and de-rotate the spine
- Performed in scoliosis-specific corrective positions
- A 2025 meta-analysis (PMID 40656945) confirmed Schroth exercises significantly reduce Cobb angle and improve quality of life in AIS
Goals of PT in Scoliosis
- Reduce or stabilize the Cobb angle (in growing patients)
- Improve spinal alignment, posture, and balance
- Strengthen paravertebral and core stabilizing muscles
- Improve flexibility and range of motion
- Improve respiratory function (especially chest expansion and vital capacity)
- Reduce pain (particularly in adult scoliosis)
- Educate patient on self-management and home exercise program
Key PT Interventions
| Intervention | Details |
|---|---|
| Schroth 3D corrective exercises | Curve-specific positions, rotational breathing, active self-correction |
| Core stabilization | Transversus abdominis, multifidus activation - goal of paraspinal strengthening to eventually allow brace weaning in adults |
| Stretching | Concave-side stretching, hip flexor stretching, hamstring flexibility |
| Breathing exercises | Expansion of collapsed concave thorax, intercostal stretching |
| Postural training | Corrective positioning, spinal alignment in daily activities |
| Proprioceptive training | Balance, coordination, body awareness |
| Manual therapy | Soft tissue mobilization, joint mobilization for pain relief |
| Hydrotherapy | Aquatic exercises - reduce gravitational load on the spine |
PT in Adult Scoliosis
For adult/degenerative scoliosis, the primary goal shifts from curve correction to pain management and functional improvement:
- Core strengthening program - to eventually allow brace to be discarded
- Cognitive behavioural therapy is another key component for chronic pain
- PT combined with soft TLSO bracing during symptomatic periods
PT After Spinal Fusion Surgery
- Early mobilization - patients ambulate immediately post-surgery with modern instrumentation
- Bracing is rarely needed post-operatively with rigid segmental instrumentation
- Progressive rehabilitation: ROM, walking, return to function
- Pre-operative and post-operative PT/OT assessment is critical (especially in neuromuscular scoliosis such as SMA)
Occupational Therapy (OT) Management
OT focuses on maximising functional independence and quality of life despite the physical limitations imposed by scoliosis or its treatment (bracing, surgery). OT is especially important in neuromuscular scoliosis (cerebral palsy, SMA, myelomeningocele).
Goals of OT
- Maximise independence in activities of daily living (ADLs) and instrumental ADLs
- Assess and adapt the patient's environment for safe function
- Optimise seating and positioning
- Address brace adaptation and compliance
- Manage fatigue, pain, and psychosocial wellbeing
- Return to work, school, and social participation
Key OT Interventions
1. Seating and Positioning
- Specialized wheelchair assessment at a comprehensive seating clinic - critical in neuromuscular scoliosis (SMA, CP)
- Maintaining an upright position in the wheelchair delays the development of scoliosis in non-ambulatory patients
- Custom-molded seating systems to correct pelvic obliquity and provide spinal support
- Pressure-relieving cushions to prevent pressure ulcers (especially with back braces in myelomeningocele)
2. Brace Management
- Patient and family education on brace donning/doffing
- Skin inspection and care - preventing pressure sores under the brace
- Adapting clothing for brace wear
- Problem-solving brace discomfort/compliance issues
- Compliance strategies - most braces require 16-23 hrs/day wear; OT helps integrate this into daily life
3. ADL Adaptation
- Adapt self-care tasks (dressing, bathing, grooming) to accommodate spinal restrictions
- Assistive devices for reaching, carrying, lifting
- Ergonomic assessment at school desk and workstation
- Energy conservation techniques for patients with respiratory compromise
4. Psychosocial Support
- Body image counselling - scoliosis and brace wear significantly affect self-esteem in adolescents
- Group therapy and peer support programs
- Anxiety management related to surgical procedures
- School reintegration support post-surgery
5. Vocational/School/Leisure Participation
- Return to school planning after surgery
- Modifications to sport, play, and leisure activities
- Adaptations for school environment
6. Neuromuscular Scoliosis - OT-specific Role
- In SMA: ensure any mobility device (scooter board, powered wheelchair) maintains function and delays contracture and scoliosis development
- Pre- and post-operative OT assessment is a critical step before spinal fusion in SMA patients
- Stretching programs for major joints as part of daily routine
- Maintain active mobility as long as possible - mobility devices, adaptations
Orthotic (Bracing) Management
Types of Braces
| Brace | Type | Use |
|---|---|---|
| Milwaukee brace | Full-length (cervical to pelvis) | Curves with apex at T6 or above; largely replaced now |
| Boston brace | Underarm TLSO | Curves with apex at T7 or lower; most common |
| Wilmington brace | Custom underarm TLSO | Similar to Boston |
| Miami brace | Underarm TLSO | Similar to Boston |
| Charleston brace | Nighttime only | Holds in maximal side-bending; single thoracolumbar/lumbar curves |
| Providence brace | Nighttime only (8-10 hrs) | Single curves; convenient for compliance |
- Full-time bracing: 23 hours/day originally; now 16+ hours commonly used
- Efficacy is dose-dependent: more hours of wear = less curve progression
- Success rate: 72% in braced patients vs. 48% with observation alone (large bracing study)
- Bracing does NOT correct permanent deformity - it prevents progression while growth continues
Surgical Management
Indications
- Curves >50 degrees with documented progression
- Loss of pulmonary function (curves >60 degrees)
- Progressive neurologic changes
- Significant coronal or sagittal imbalance
- Refractory pain (adults)
Goals of Surgery
- Prevent further progression (primary goal) via spinal fusion
- Correct and improve the deformity
- Maintain appropriate sagittal balance
- Preserve pulmonary function
- Minimize morbidity and maximize post-op function
Procedure
- Posterior spinal instrumentation and fusion (pedicle screws, rods)
- Lenke classification guides which curves to instrument and fuse
- Anterior + posterior approach in some cases (neuromuscular, congenital) - provides greater correction and lower pseudarthrosis rates
Post-Operative Considerations
- Early ambulation - immediately after surgery with modern rigid fixation
- Multimodal pain management protocol
- Hospital stay reduced with enhanced recovery protocols (2.9 vs 4.3 days)
- Complications: 13-40% overall; pseudarthrosis 13-17%; reoperation rate 20-40%
Special Scenarios
Early Onset Scoliosis (<10 years)
- Lung development occurs in early childhood - progressive deformity impairs this
- Management must preserve growth: serial casting (EDF - Elongation, Derotation, Flexion casts) or growing rods before fusion
Neuromuscular Scoliosis
- Occurs in up to 90% of myelomeningocele patients (100% with T12 lesion)
- More progressive, less responsive to bracing
- PT/OT multidisciplinary team is essential
- Surgery often required; posterior spinal fusion with pelvic fixation
Idiopathic Scoliosis + Pain
- Scoliosis itself is generally painless - pain warrants investigation for infection, tumour (especially osteoid osteoma), disc pathology, or spondylolisthesis
Recent Evidence
- A 2025 network meta-analysis (PMID 40183057) found Schroth-based exercises and yoga/pilates-type programs most effective for improving Cobb angle and quality of life in AIS
- A 2025 meta-analysis (PMID 40656945) confirmed Schroth exercises significantly reduce Cobb angle and improve trunk balance and quality of life
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Bailey and Love's Short Practice of Surgery 28th Ed | Grainger & Allison's Diagnostic Radiology | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.