Hey give me some points about lung abscess
Reading File
Finding Sources
Searching PubMed
"lung abscess"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer. Here is a well-organized summary of lung abscess:
Lung Abscess
Definition: Lung abscess is localized necrosis and cavitation of the pulmonary parenchyma due to microbial infection, usually forming a single dominant cavity >2 cm in diameter. - Harrison's Principles of Internal Medicine 22E, p. 1079 | Sabiston Textbook of Surgery
Classification
| Type | Description |
|---|---|
| Primary (~80%) | Due to aspiration in otherwise healthy host; mainly anaerobes |
| Secondary (~20%) | Underlying condition - obstruction, immunocompromise, septic emboli |
| Acute | <4-6 weeks duration |
| Chronic | >4-6 weeks; ~40% of cases |
| Putrid | Foul-smelling sputum; strongly suggests anaerobic origin |
Etiology & Predisposing Factors
Aspiration is by far the most common mechanism. Risk groups include:
- Altered consciousness (alcoholism, drug overdose, seizures, anesthesia)
- Bulbar dysfunction, prior stroke, neuromuscular disease
- Esophageal dysmotility, GERD, gastric distension
- Poor dentition / periodontal disease (anaerobic colonization of gingival crevices)
Other causes:
- Necrotizing pneumonia - from S. aureus, Streptococcus pyogenes, Klebsiella pneumoniae, Pseudomonas spp.
- Bronchial obstruction - especially lung carcinoma (impaired drainage + atelectasis)
- Septic emboli - right-sided infective endocarditis (typically S. aureus), Lemierre's syndrome (Fusobacterium necrophorum)
- Hematogenous spread - staphylococcal bacteremia → multiple abscesses
- Fungi/mycobacteria - Aspergillus, Cryptococcus, Histoplasma, M. tuberculosis can mimic or cause cavitary disease
Microbiology
- Anaerobes are present in up to 93% of cases and are the sole isolates in 1/3 to 2/3 of primary abscesses - Fishman's Pulmonary Diseases
- Most common anaerobes: Prevotella, Fusobacterium, Bacteroides, Peptostreptococcus, and microaerophilic streptococci (oral commensals)
- In immunocompromised hosts: Pseudomonas aeruginosa, gram-negative rods, Nocardia, Aspergillus, Cryptococcus
- Metronidazole alone is NOT effective as single-agent therapy - it misses microaerophilic streptococci - Harrison's, p. 1079
Location (Morphology)
- Right side > Left side (more vertical right mainstem bronchus)
- Posterior segment of right upper lobe and apical segments of lower lobes - dependent segments in a recumbent person
- Aspiration-related: usually single
- Pneumonia/bronchiectasis-related: often multiple, basal, bilateral
- Hematogenous: multiple, scattered
- Abscess size ranges from a few mm to 5-6 cm in diameter
- Robbins & Kumar Basic Pathology
CT Scan Example
Below is a CT chest of a 43-year-old patient showing a left upper-lobe lung abscess (arrow), complicating Streptococcus milleri infection:
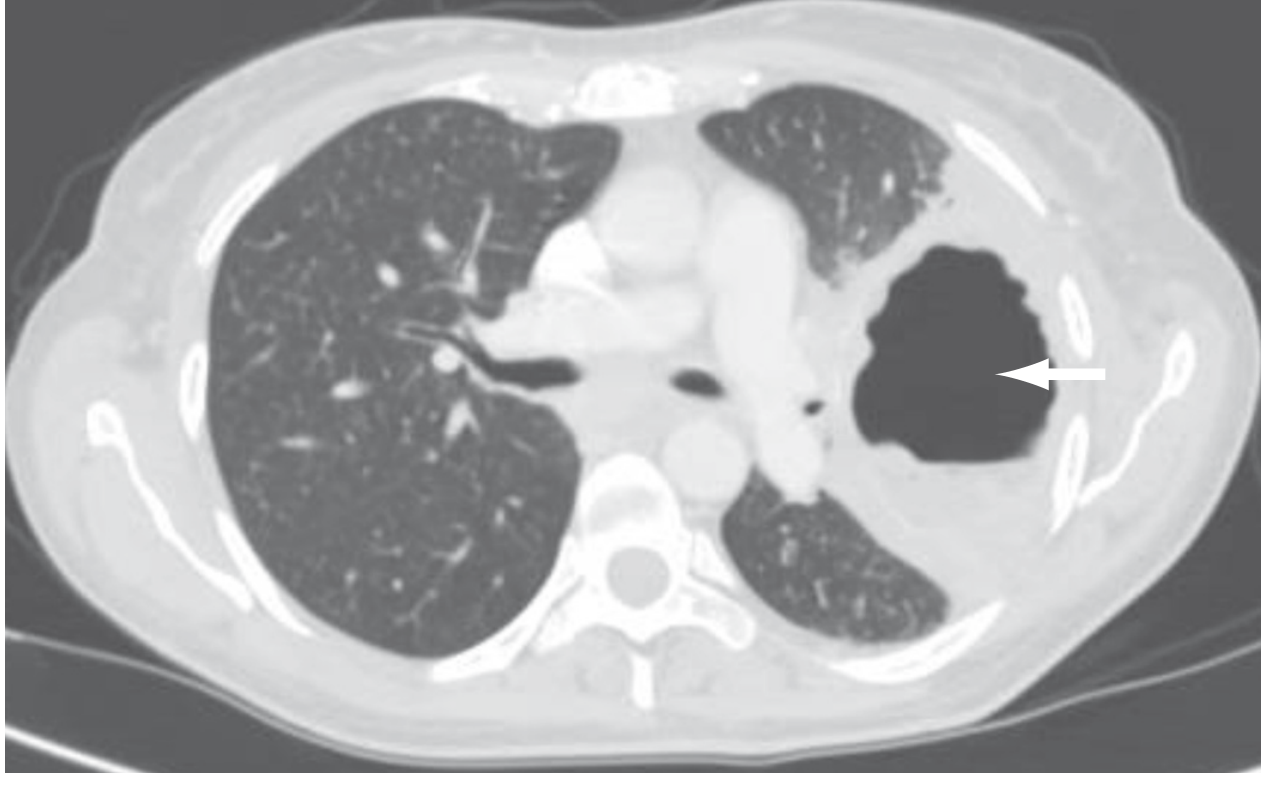
- Sabiston Textbook of Surgery
Clinical Features
- Indolent onset over weeks to months (especially anaerobic)
- Fever, cough, purulent or foul-smelling sputum (putrid = anaerobic)
- Night sweats, weight loss, anemia (chronic systemic features)
- Hemoptysis (variable)
- On CXR: cavity with air-fluid level after drainage into an airway
Diagnosis
- Chest X-ray: Infiltrate with cavity, often with air-fluid level
- CT chest (preferred): Better delineates cavitation, distinguishes parenchymal abscess from pleural collection (empyema), detects associated mass lesions
- Sputum culture, blood cultures
- Bronchoscopy: to obtain cultures, exclude obstructing lesion/foreign body
Periodontal disease + aspiration risk = classic primary lung abscess. Edentulous patients with abscess should prompt search for obstructing lesion or alternative etiology.
Treatment
Antibiotics (first-line)
- Clindamycin 600 mg IV TID → then 300 mg PO QID (superior to penicillin due to beta-lactamase-producing anaerobes in RCTs)
- IV beta-lactam/beta-lactamase inhibitor (e.g., ampicillin-sulbactam) → then oral amoxicillin-clavulanate
- Moxifloxacin 400 mg/d PO - shown as effective as ampicillin-sulbactam in one small study
Duration: 3-4 weeks minimum; up to 14 weeks; many recommend at least 6 weeks for better outcomes. Continue until imaging shows resolution or small residual scar. - Harrison's, p. 1079
When Medical Therapy Fails
- 10-20% of patients may not respond (continued fevers, abscess progression)
- Abscesses >6-8 cm are less likely to respond to antibiotics alone
- Options: Percutaneous drainage (risk: pneumothorax, hemothorax, pleural contamination) or surgical resection
- Bronchoscopy for direct cavity drainage may be used
Surgical Indications (Sabiston)
- Persistent cavity ≥2 cm, thick-walled after ≥8 weeks of treatment
- Failure to clear sepsis
- Hemoptysis, rupture into pleural space
Complications
- Empyema - extension to pleural space
- Life-threatening hemoptysis
- Massive aspiration of abscess contents
- Pneumatoceles or bronchiectasis (especially with large initial cavities)
- Recurrence despite therapy
Prognosis
| Group | Mortality |
|---|---|
| Primary abscess | As low as 2% |
| Secondary abscess | Up to 75% (some series) |
Poor prognostic factors: Age >60, malignancy, aerobic bacteria, sepsis on presentation, symptoms >8 weeks, abscess >6 cm diameter.
- Harrison's Principles of Internal Medicine 22E (2025)
- Robbins & Kumar Basic Pathology
- Fishman's Pulmonary Diseases and Disorders
- Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.