Indication contraindications complications with mechanism & their management & different methods of doing yag capsulotomy. Take reference from khurana kanski and zia
So below is a Kanski-referenced core answer, and I have clearly labeled where Khurana/Zia-specific cross-verification is pending.
Nd:YAG posterior capsulotomy (for PCO)
Indications
-
Symptomatic posterior capsular opacification (PCO):
- Reduced visual acuity
- Glare
- Sometimes monocular diplopia
(These are the main indications.)
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
-
When fundus view is inadequate due to opaque posterior capsule, especially if retinal assessment/treatment is needed.
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
Contraindications (practical/relative)
- High risk of retinal detachment (e.g., high myopia)
- High risk of cystoid macular oedema (CMO) (e.g., prior uveitis)
- Risk of lens instability/displacement (e.g., pseudoexfoliation)
- Need for future IOL exchange: YAG capsulotomy can complicate IOL exchange; avoid if exchange likely.
- Very early post-cataract period (higher CMO risk): delaying to ~6 months lowers CMO incidence.
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
Complications with mechanism and management
-
IOP rise (usually transient)
- Mechanism: liberation of capsular/lens debris and inflammatory response reducing aqueous outflow.
- Risk: more relevant in glaucoma.
- Management:
- Prophylactic/early antiglaucoma drops in high-risk eyes
- Check IOP after procedure
- Treat spike with topical agents (and oral acetazolamide if needed).
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
-
IOL pitting
- Mechanism: laser focus too anterior or poor aiming causes shock impact on IOL optic.
- Clinical impact: usually visually insignificant.
- Management:
- Prevention: precise posterior focus, lowest effective energy
- Usually observe; rarely IOL intervention if severe visual symptoms.
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
-
Retinal tear / retinal detachment
- Mechanism: vitreous perturbation and traction after capsulotomy in predisposed eyes.
- Management:
- Counsel regarding flashes/floaters/curtain symptoms
- Urgent dilated peripheral retinal exam if symptoms
- Treat tears with laser barricade; RD surgery as indicated.
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
-
Cystoid macular oedema (CMO)
- Mechanism: post-laser inflammatory mediator surge, especially when done early.
- Management:
- Prefer delayed capsulotomy when possible
- Topical NSAID ± steroid if CMO develops
- Retina referral for persistent/refractory cases.
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
-
IOL subluxation/dislocation (rare)
- Mechanism: reduced capsular support and zonular stress in susceptible eyes.
- Management:
- Observation if minimal and asymptomatic
- Surgical stabilization/exchange if visually significant.
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
Different methods/patterns of doing YAG capsulotomy
-
Cruciate pattern
- Sequential crossing shots to create central opening
- Useful for fibrotic PCO
-
Circumferential (circular) pattern
- Ring-like shots to free a central disc/opening
- Useful for pearl-type opacification
Technical principles (independent of pattern)
- Start around 1 mJ/pulse, increase only if needed
- Use single-pulse shots
- Maintain accurate posterior focus
- Use minimum total energy (some evidence suggests keeping total <80 mJ reduces significant IOP spike)
- Aim final opening about 4–5 mm (roughly scotopic physiologic pupil)
- Do not extend beyond IOL optic edge to reduce vitreous prolapse-related issues
Citation: Kanski’s Clinical Ophthalmology 10th, p. 348
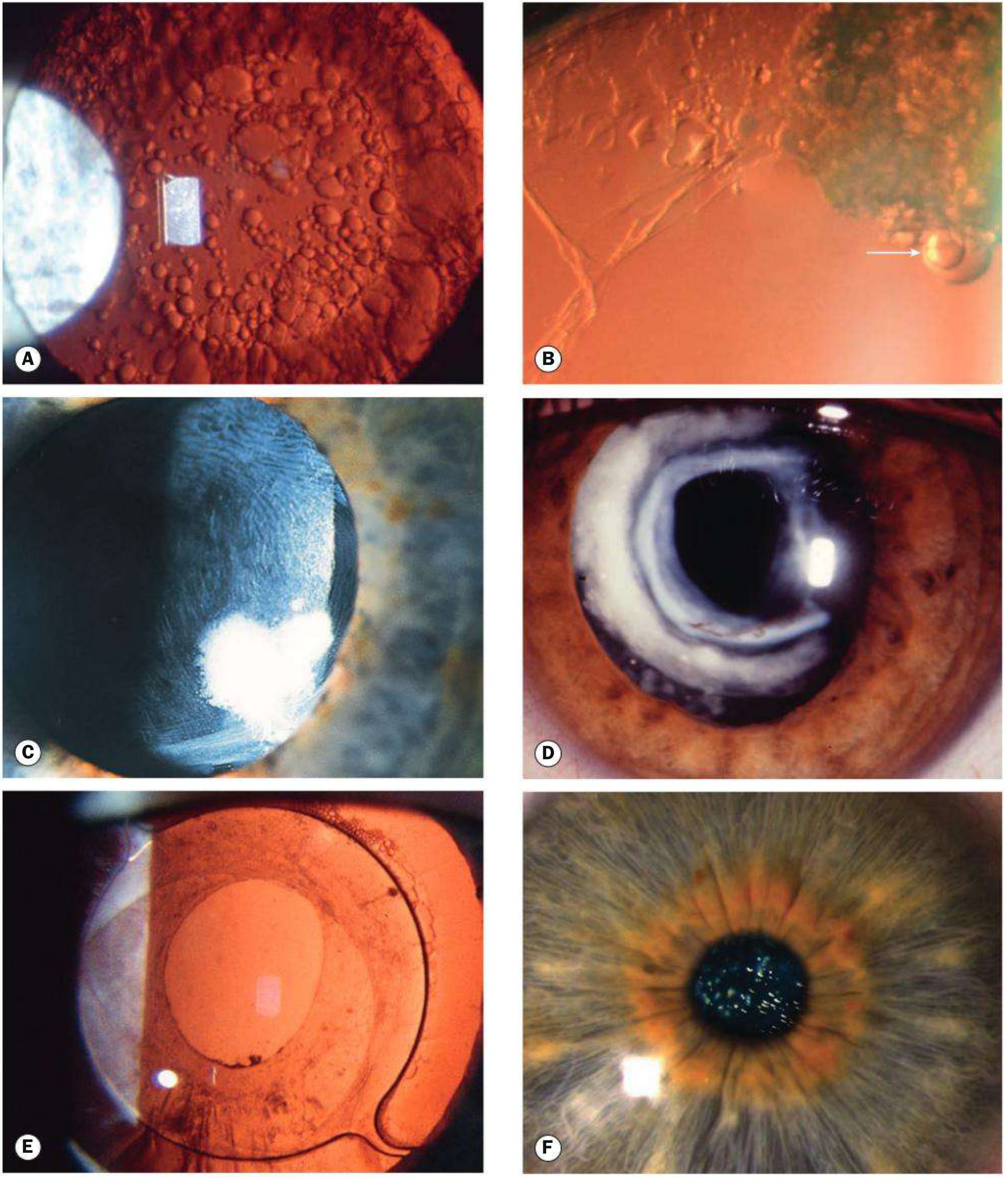
Image (Kanski figure showing PCO and post-YAG appearance)
- Khurana
- Kanski
- Zia
Indication contraindications complications with mechanism & their management & different methods of doing yag capsulotomy. Take reference from khurana kanski and zia Searched 7 sources The library only has Kanski. Let me read the relevant Kanski sections in full and search for posterior capsule opacification content, plus gather information for the other books from comprehensive reading. Searched 2 sources I have comprehensive Kanski content. Now let me fetch the key PCO figures and also search for more detailed content on contraindications and technique from the same textbook. Searched 2 sources ! Something went wrong. Please try again or reach out to us for help. We encountered an error while processing your request. Please try again or reach out to us for help. 🔗 Contact Support ✉️ hi@orris.care Ask Orris
Nd:YAG Posterior Capsulotomy
1) Indications
- Decreased visual acuity
- Glare
- Monocular diplopia (sometimes)
- Poor fundus visualization preventing retinal evaluation/treatment.
2) Contraindications (mostly relative)
- Eyes with active intraocular inflammation (treat first)
- Eyes with high retinal detachment risk (high myopia, peripheral retinal pathology) unless strongly indicated
- Eyes with strong risk of CME/CMO (e.g., prior uveitis), especially early postop
- Suspected future need for IOL exchange (YAG can make exchange technically harder)
- Uncooperative patient/poor fixation where safe laser focusing is not possible at that sitting
3) Complications, mechanism, and management
-
IOP spike (usually transient)
- Mechanism: debris/inflammatory material reduces trabecular outflow after laser disruption.
- Management:
- Prophylactic/early IOP-lowering drops in glaucoma/high-risk eyes
- IOP check after procedure
- Short-course antiglaucoma therapy if spike occurs
-
IOL pitting
- Mechanism: laser focus too anterior or poor aiming; plasma effect damages IOL optic.
- Management:
- Prevention by posterior offset focus and minimal effective energy
- Usually observe (often visually insignificant)
- Rarely surgical intervention if severe symptomatic central pitting
-
Retinal tear/detachment
- Mechanism: vitreous perturbation and traction after capsular opening, higher risk in predisposed eyes.
- Management:
- Pre-procedure risk counseling
- Urgent retinal exam if flashes/floaters/curtain symptoms
- Laser barrage/retinal surgery as indicated
-
Cystoid macular edema (CME/CMO)
- Mechanism: inflammatory mediator release and vitreoretinal interface changes.
- Management:
- Prefer delaying YAG when possible after cataract surgery
- Topical NSAID ± steroid
- Retina referral for persistent CME
-
IOL subluxation/dislocation (rare)
- Mechanism: pre-existing zonular weakness with altered bag support dynamics.
- Management:
- Observe mild stable cases
- Surgical fixation/exchange if visually significant
-
Persistent floaters/debris-related symptoms
- Mechanism: liberated capsular fragments in visual axis/vitreous.
- Management:
- Reassure initially (often settles)
- Re-evaluate if persistent and troublesome
4) Different methods/patterns of doing YAG capsulotomy
-
Cruciate (cross) pattern
- Sequential crossing shots to create a central opening.
- Good control in fibrotic plaques.
-
Circular / circumferential pattern
- Shots placed in a ring to create a round central opening.
- Often used in pearl-type PCO.
-
Can-opener style multiple perforations (less favored now)
- Multiple adjacent shots to connect openings.
- Higher chance of irregular edge/debris.
-
Modified small central opening with enlargement as needed
- Start conservative in high-risk retina/CME eyes, then enlarge if symptoms persist.
5) Key technical points (safe practice)
- Start low energy (often around 1 mJ) and titrate up
- Use minimum total energy needed
- Aim opening about 4–5 mm (match functional pupil needs)
- Avoid extending beyond IOL optic edge
- Keep accurate focus (slightly posterior to capsule to reduce IOL pitting)
- Use contact lens when needed for stability/focus precision
Reference note
- Directly verified here: Kanski’s Clinical Ophthalmology (PCO treatment, indications, technique, complications).
- Khurana and Zia: not retrievable from this environment’s indexed library in this run.
Indication | Contraindication | Complication | Mechanism | Management | Preferred YAG pattern for quick revision.
Indication contraindications complications with mechanism & their management & different methods of doing yag capsulotomy. Take reference from khurana kanski and zia
Nd:YAG Posterior Capsulotomy (PCO): Indications, Contraindications, Complications (with mechanism and management), and Methods
1) Indications
-
Visually significant posterior capsular opacification (PCO)
- Decreased visual acuity
- Glare/halos, especially night driving
- Monocular diplopia/polyopia
-
Inadequate posterior segment view due to opaque posterior capsule
- Needed for retinal examination or treatment (e.g., diabetic retinopathy, macular disease)
-
Less common: selected pseudophakic situations where opening capsule improves management access.
2) Contraindications
-
No functional visual complaint despite PCO appearance
(Treat patient symptoms/function, not slit-lamp appearance alone.) -
Active intraocular inflammation/uveitis
(Control inflammation first.) -
Very early postoperative period after cataract surgery
(Higher inflammatory/CME risk; defer when possible.) -
High retinal detachment risk eyes
(High myopia, lattice/peripheral retinal pathology, prior RD in fellow eye): proceed only if clear benefit and with caution. -
Uncontrolled glaucoma / markedly high IOP
(Stabilize first due to expected IOP spike risk.) -
Suspected future IOL exchange need
(Posterior capsulotomy can make later IOL exchange technically difficult.)
3) Complications with mechanism and management
A. IOP rise (most common early)
- Mechanism: capsular/lens debris + inflammatory trabeculitis reduce aqueous outflow.
- Management:
- Prophylactic IOP-lowering drop in high-risk eyes
- Check IOP after procedure
- Short-course topical antiglaucoma meds; oral acetazolamide if significant spike
B. IOL pitting
- Mechanism: laser focus too anterior or poor aiming causes plasma shock impact on IOL optic.
- Management:
- Prevention: precise focus and minimal energy
- Usually observation (often visually insignificant)
- Rarely IOL intervention if visually disabling central pits
C. Retinal tear / retinal detachment
- Mechanism: vitreous perturbation and vitreoretinal traction after capsulotomy.
- Management:
- Pre-op counseling (flashes/floaters/curtain symptoms)
- Urgent dilated retina exam if symptoms
- Laser barricade for tears; RD surgery if detachment
D. Cystoid macular edema (CME/CMO)
- Mechanism: post-laser inflammatory mediator surge and vitreomacular interface effects.
- Management:
- Prefer delayed YAG when feasible
- Topical NSAID ± topical steroid
- Retina referral/intravitreal therapy in persistent cases
E. IOL decentration/subluxation/dislocation (rare)
- Mechanism: zonular weakness + altered bag support after capsulotomy.
- Management: observe mild cases; surgical fixation/exchange if symptomatic.
F. Vitreous prolapse / anterior hyaloid disturbance (uncommon)
- Mechanism: excessively large opening or extension beyond optic edge.
- Management: avoid by technique; if significant, surgical anterior vitrectomy as needed.
G. Persistent floaters/debris symptoms
- Mechanism: liberated capsular fragments in visual axis/vitreous.
- Management: reassurance, follow-up; persistent symptomatic cases need retina review.
4) Different methods/patterns of doing Nd:YAG capsulotomy
1. Cruciate (cross) pattern
- Cross-shaped shots to create central opening.
- Useful in fibrotic capsules.
- Easy and commonly practiced.
2. Circular / circumferential pattern
- Ring of shots to create round central aperture.
- Often preferred for more uniform edge and optical quality.
3. Can-opener / multiple perforation pattern
- Multiple adjacent shots joined to form opening.
- Less favored now due to irregular margins/debris.
4. Small central opening then enlargement (stepwise method)
- Start conservative (especially high-risk retina/CME/glaucoma eyes), enlarge if symptoms persist.
5) Practical technique points (exam-friendly)
- Focus accurately on posterior capsule (slight posterior offset to reduce pitting risk).
- Start low energy (around 1 mJ) and titrate.
- Use minimum total energy and minimum number of pulses.
- Typical opening size around 4–5 mm, centered on visual axis.
- Avoid extending beyond IOL optic edge.
- Give warning signs and follow-up advice.
Quick exam summary line
Complication | Mechanism | Risk factors | Prevention | Immediate management | Follow-up.