Spinal bifida
Reading File
Finding Sources
Finding Sources
Searching PubMed
"spina bifida" OR "myelomeningocele"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Spina Bifida
Spina bifida is a neural tube defect (NTD) resulting from failure of the embryonic vertebral arches (and in severe forms, the neural tube itself) to fuse during early fetal development. It represents a spectrum from a clinically silent bony gap to severe, life-altering spinal cord exposure.
Embryology
The neural tube normally closes by day 26 of embryogenesis. Failure of the posterior neuropore to close produces open NTDs. Contributing factors include chromosomal abnormalities (deletions, duplications, trisomy), folate deficiency, vitamin A deficiency, and teratogen exposure. Single-gene mutations are uncommon.
- The Developing Human - Clinically Oriented Embryology, p. 928
- Goldman-Cecil Medicine, Ch. 385
Classification
| Type | Description | Key Features |
|---|---|---|
| Spina bifida occulta | Bony defect of vertebral arch only; no herniation | Usually asymptomatic; incidental imaging finding; may have overlying skin dimple, tuft of hair |
| Meningocele | Meninges and CSF herniate through bony defect, covered by skin | Nerve tissue NOT involved; better prognosis |
| Myelomeningocele | Spinal cord + meninges herniate through defect; roof formed by exposed neural tissue | Most severe open form; 75% develop hydrocephalus |
| Myelocele | Open midline lesion; exposed neural elements flush with adjacent skin | Visible at birth; high morbidity |
- Bailey and Love's Surgery, p. 543
- Goldman-Cecil Medicine, p. 4043
MRI Appearance
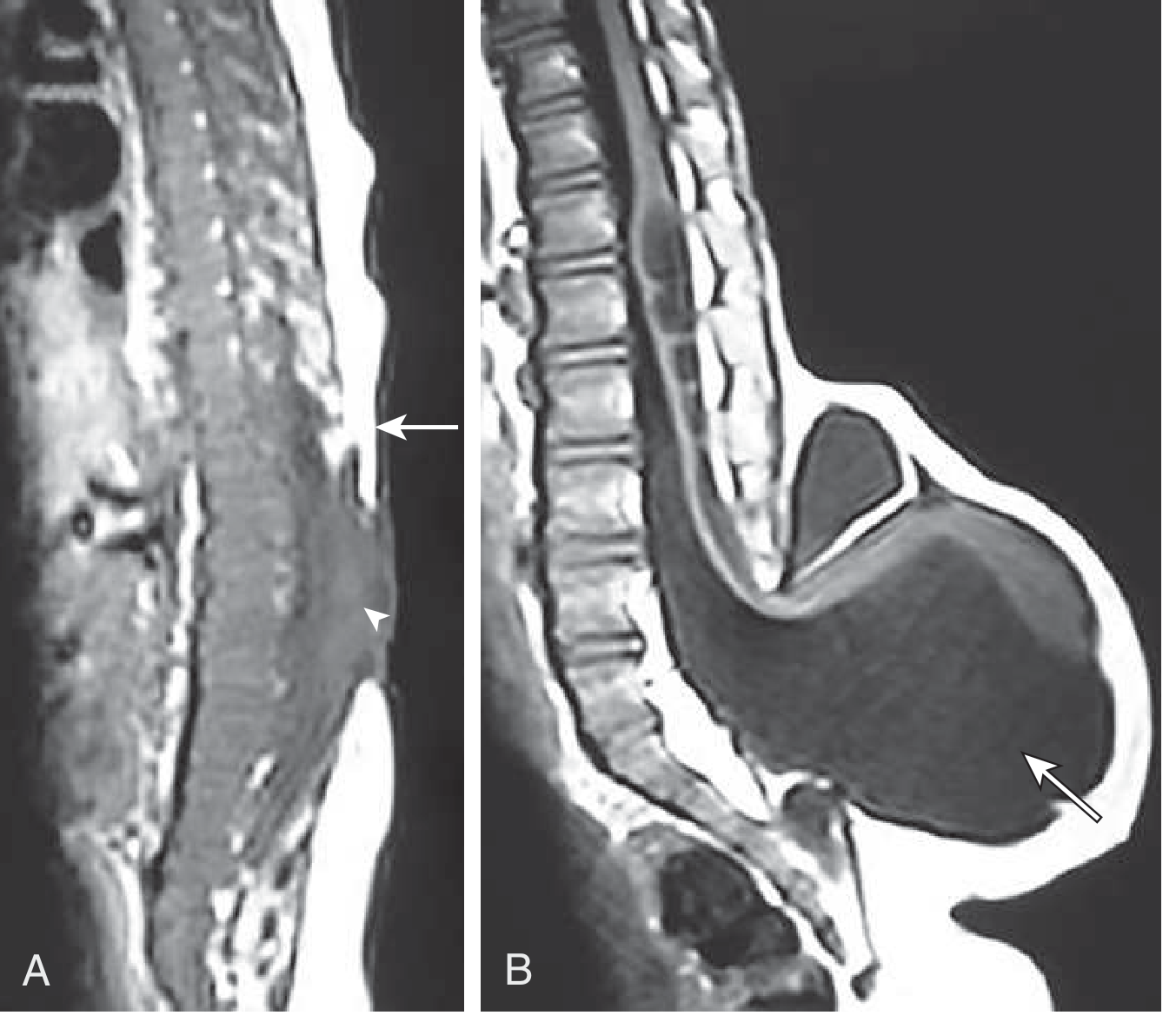
(A) Myelocele: neural tissue (arrowhead) is flush with the skin surface (arrow). (B) Myelomeningocele: lesion extends beyond the skin surface and contains nerve tissue + CSF (arrow).
- Goldman-Cecil Medicine, Fig. 385-1
Epidemiology
- Incidence: ~1 per 1,000 births worldwide; ~0.6 per 1,000 in the USA
- Females slightly more affected than males
- Incidence has been declining due to:
- Routine periconceptional folic acid supplementation
- Folate fortification of grain and cereal products
- Antenatal ultrasound screening
- Maternal serum alpha-fetoprotein (AFP) measurement
- Goldman-Cecil Medicine, p. 4043; Bailey and Love's, p. 543
Risk Factors
- Low maternal serum folate / inadequate folic acid intake (<400 mcg/day, OR ~3.7 for NTDs)
- Valproic acid or other folate-antagonist use during pregnancy (carbamazepine, methotrexate) - ~1-2% risk
- Prior affected pregnancy (3-5% recurrence risk)
- Chromosomal abnormalities
- Vitamin A deficiency
Clinical Features
Manifestations depend on the level and extent of the lesion:
- Lumbosacral (most common site): less devastating than thoracic/cervical
- Motor deficits: flaccid paralysis (lower motor neuron) or spasticity (upper motor neuron) below the lesion level
- Sensory loss below lesion - predisposes to pressure ulcers
- Bowel and bladder dysfunction - virtually universal regardless of level; neuropathic bladder leads to recurrent UTIs and may cause renal failure
- Hydrocephalus: 75% of myelomeningocele cases
- Chiari II malformation: downward displacement of cerebellar vermis, fourth ventricle, and medulla through the foramen magnum - commonly co-occurs with myelomeningocele
- Tethered cord: progressive neurological deterioration with growth
- Epilepsy: especially with associated brain malformation or hydrocephalus
- Skeletal deformities: kyphosis, clubfoot, extremity contractures, neuromuscular scoliosis
- Latex allergy: unusually common; frequency increases with age
- Corpus callosum agenesis: may be associated
Diagnosis
Prenatal:
- Antenatal ultrasound: often detects the defect
- Elevated maternal serum AFP (amniotic fluid AFP + acetylcholinesterase)
- Acetylcholinesterase in amniotic fluid (normally found in CSF, not amniotic fluid) is a confirmatory marker
- MRI can define the extent of abnormality
Postnatal:
- Clinical inspection at birth (visible midline back lesion)
- MRI of brain and spine for associated anomalies (Chiari, hydrocephalus, tethering)
Management
Surgical
| Intervention | Timing | Indication |
|---|---|---|
| Closure of open defect | Within 3 days of birth | Myelocele / myelomeningocele |
| Ventriculoperitoneal (VP) shunt | Early | Hydrocephalus (required in majority) |
| Prenatal (in utero) closure | ~23-25 weeks gestation | Reduces incidence of hydrocephalus and shunt need |
| Meningocele sac excision | 3-6 months | Prominent meningocele sac |
A selective approach is applied for myelomeningocele: severe hydrocephalus, large open defect with no distal neurological function may influence the decision to operate. The majority of non-operated children die within the first year.
Medical / Supportive
- Antibiotics immediately after birth for open NTDs
- Clean intermittent catheterization (CIC) for neuropathic bladder
- Skin care to prevent pressure ulcers
- Neuropsychological support
- Treatment of epilepsy
- Monitoring for VP shunt dysfunction, tethered cord, and syrinx (any neurological deterioration in a static lesion should prompt investigation)
Orthopaedic
- Muscle imbalance causes secondary joint deformity
- Physiotherapy, bracing, tendon releases, and deformity correction as indicated
- Gait analysis guides surgical and non-surgical planning
Prevention
- Folic acid 400 mcg/day periconceptionally for all women of childbearing age
- 4-5 mg/day for high-risk women (prior affected pregnancy, anticonvulsant use)
- Population-level grain fortification with folic acid
Associated Conditions
- Arnold-Chiari (Chiari II) malformation - herniation of medulla and cerebellar tonsils through foramen magnum; treated by decompression of foramen magnum
- Syringomyelia - CSF-filled cavity within the cord
- Spinal dysraphism - broader group including diastematomyelia (bony/cartilaginous spur across the vertebral canal)
- Tethered cord syndrome - progressive neurological deficit from cord traction with growth
Prognosis
With antibiotics, early surgical closure, and VP shunting: approximately half of children surviving the first 24 hours will reach school age. Long-term challenges include skin problems, neuromuscular scoliosis, joint deformity, renal complications from neuropathic bladder, and cognitive/learning difficulties.
- Bailey and Love's Surgery, p. 543-544
- Goldman-Cecil Medicine, Ch. 385
Recent evidence note: A 2024 meta-analysis (PMID 39126714) examined simultaneous vs. delayed VP shunt placement during myelomeningocele closure, and a 2026 systematic review (PMID 41849992) reviewed outcomes in African populations - these reflect ongoing refinement of surgical timing guidelines but do not contradict the core management framework above.
More diagrams
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Here is the full visual collection from the textbooks, organized by category:
Spina Bifida - Diagrams & Images
1. Cross-sectional anatomy: All four types (A & B panels)
A = Spina bifida occulta - unfused neural arch only, spinal cord in normal position, overlying tuft of hair. B = Meningocele - meninges and CSF herniate out, but spinal cord stays in place.
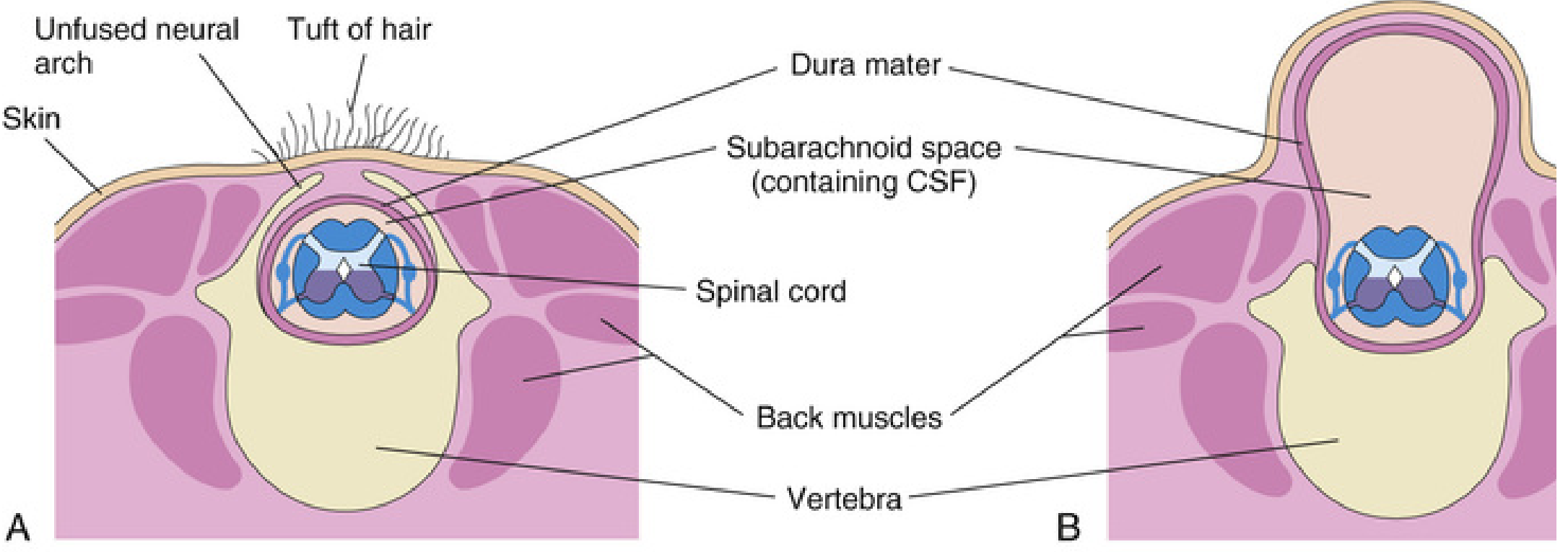
Fig. 17.12 A & B - The Developing Human: Clinically Oriented Embryology
C = Myelomeningocele - displaced spinal cord + nerve roots herniate into the membranous sac. D = Myeloschisis - open spinal cord fully exposed, flush with skin surface.
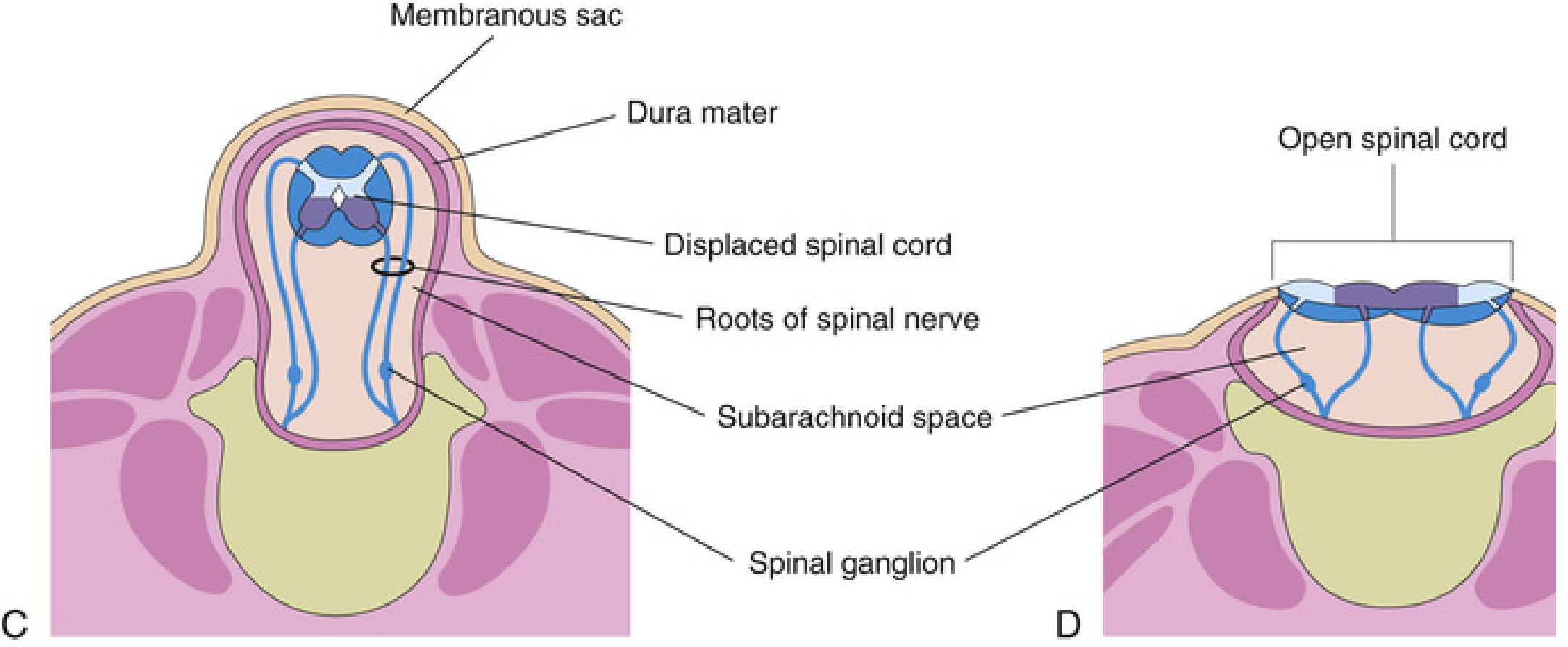
Fig. 17.12 C & D - The Developing Human: Clinically Oriented Embryology
2. Medical Physiology diagram - Variations of spina bifida
Axial cross-section showing the myelomeningocele sac with displaced spinal cord, membranous sac, and vertebral body clearly labelled.
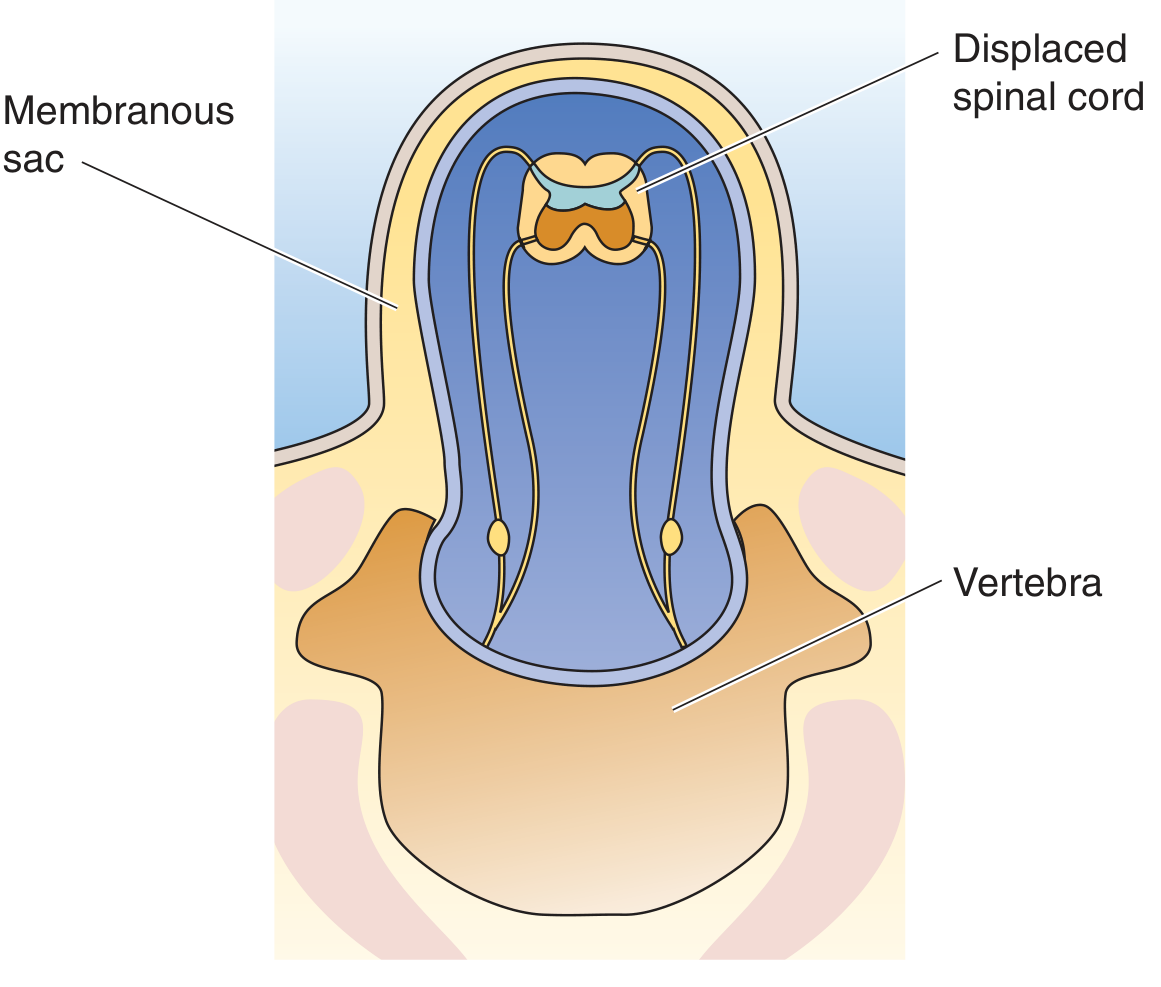
Fig. 10-7 - Medical Physiology (Boron & Boulpaep)
3. Sagittal MRI - Lumbosacral myelomeningocele
T1-weighted sagittal MRI showing the large myelomeningocele sac protruding posteriorly, with absent laminae/spinous processes. Also visible: brain, fourth ventricle, and thoracic aorta for orientation.
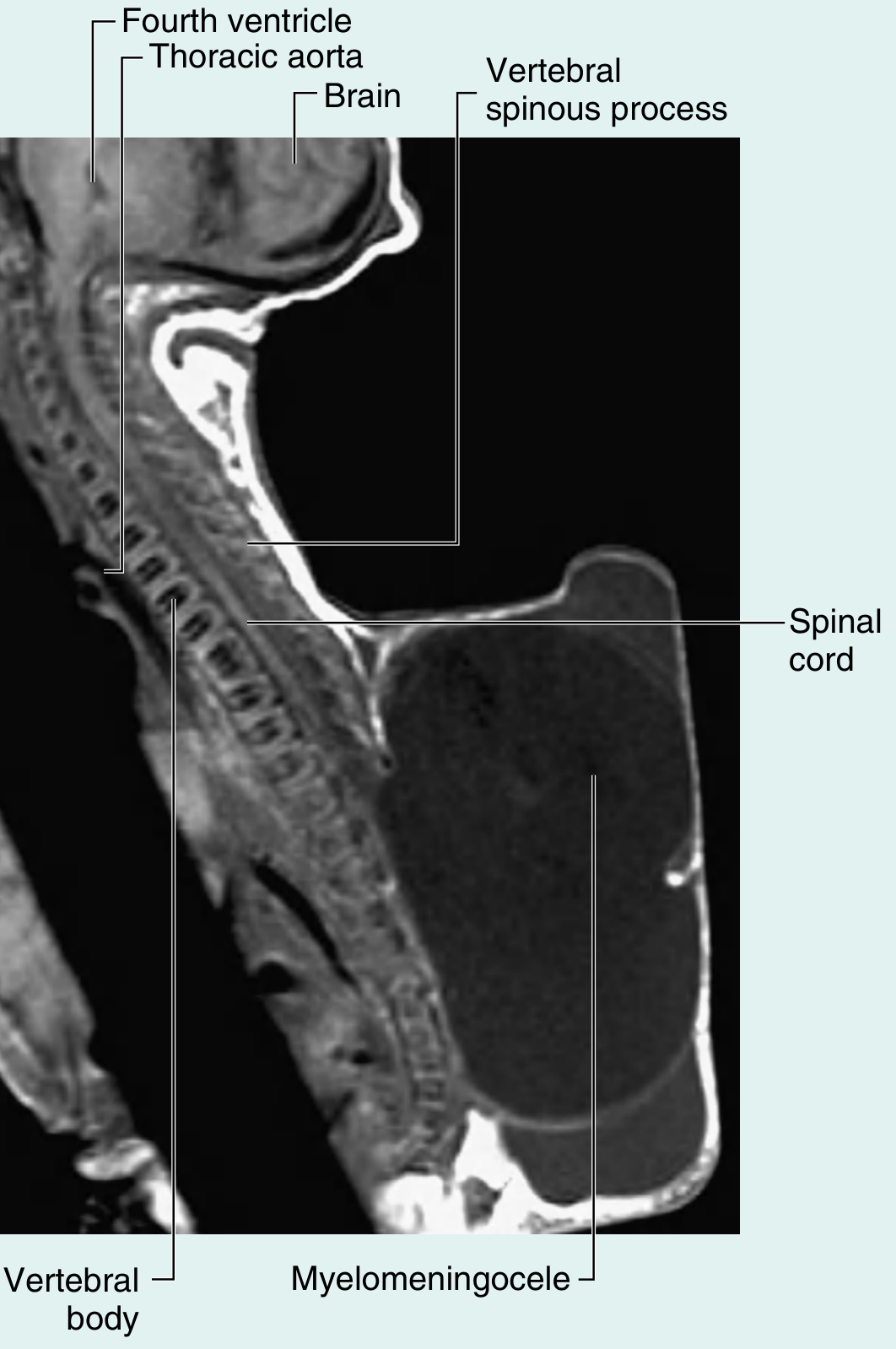
Fig. 2.24 - Gray's Anatomy for Students
4. Surgical anatomy illustrations - Myelomeningocele
A: Newborn infant with visible myelomeningocele on the back. B: Axial (cross-sectional) view showing the neural plaque, CSF, pia-arachnoid, dura, skin, and vertebra. C: Lateral/sagittal view showing how the neural plaque sits atop the sac with nerves exiting below, CSF within, and the skin deficit around it.
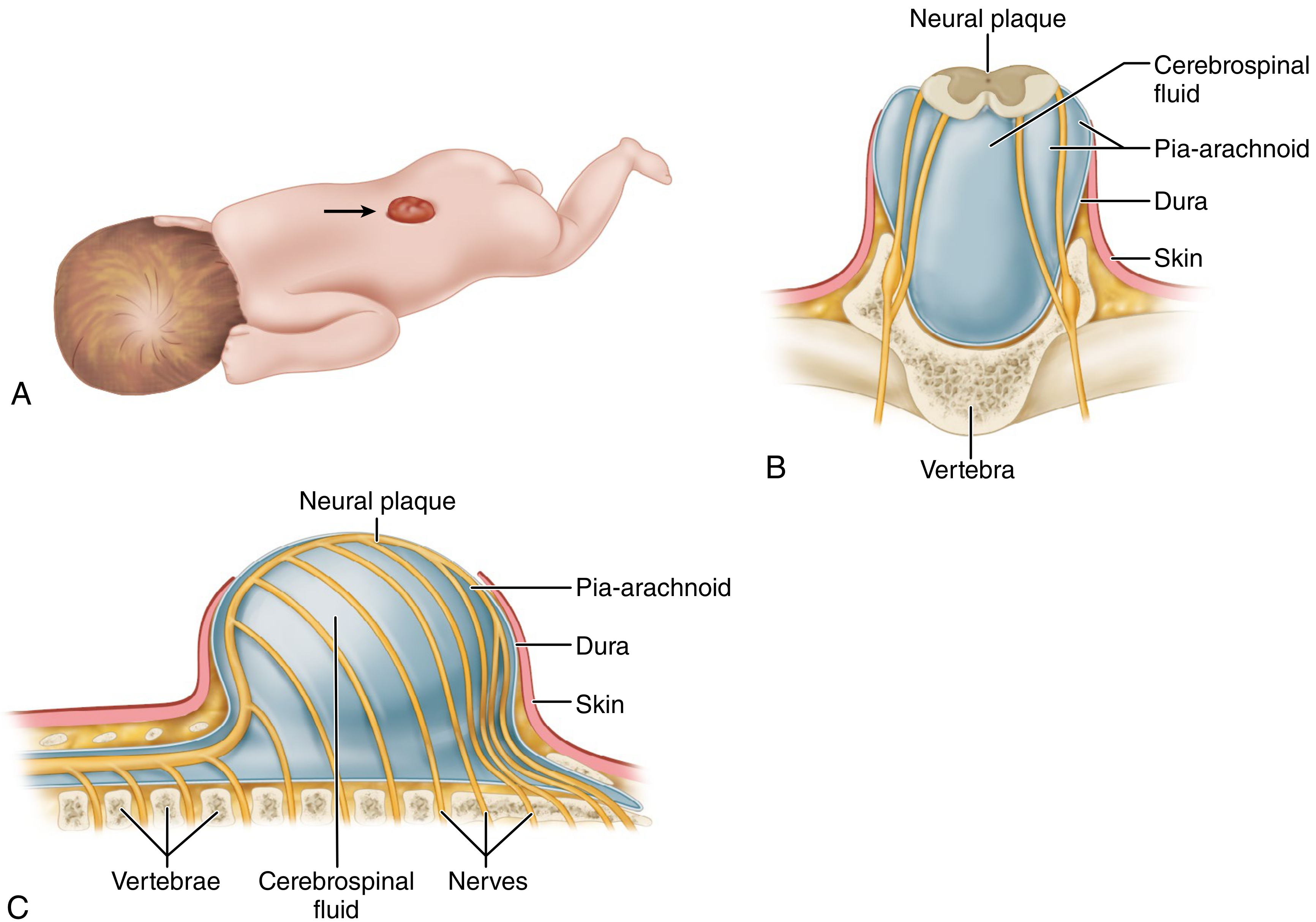
Fig. 36.2 - Campbell's Operative Orthopaedics 15th Ed. 2026
5. Bradley & Daroff's Neurology - Sagittal illustration of myelomeningocele
Detailed sagittal illustration showing the spinal cord and nerve roots (labelled "Cord" and "Roots") herniated into the posterior sac, with the vertebral column visible anteriorly.
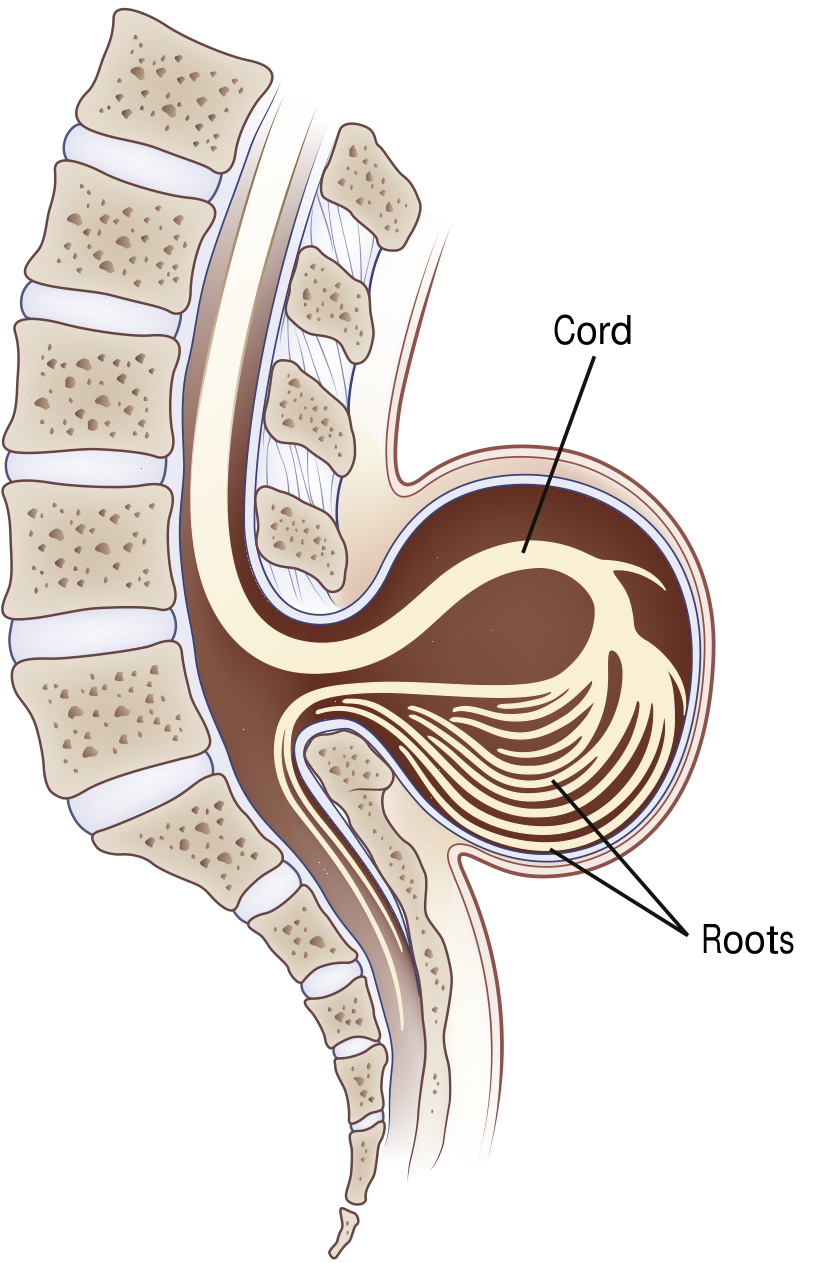
Fig. 104.10 - Bradley and Daroff's Neurology in Clinical Practice
6. Bradley & Daroff's Neurology - Sagittal illustration of meningocele
Companion diagram showing a meningocele: the sac contains only CSF with no cord or roots within it - the cord stays in the canal.
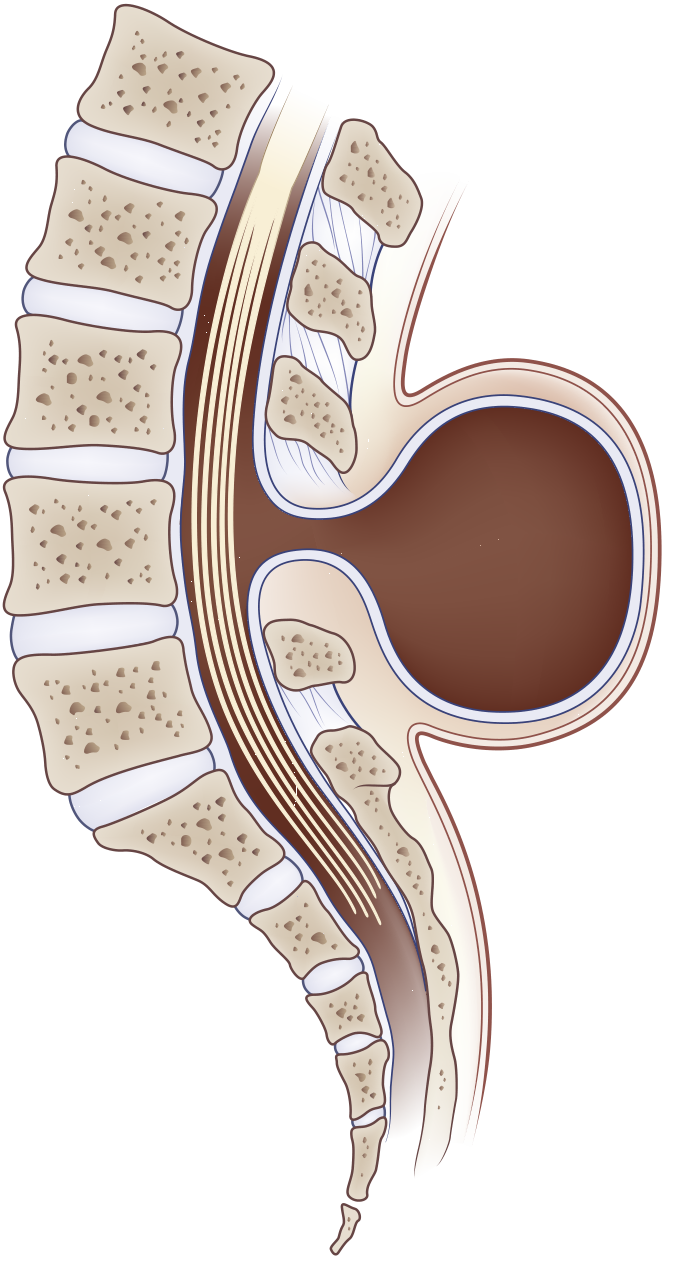
Fig. 104.11 - Bradley and Daroff's Neurology in Clinical Practice
7. Clinical photos - Infants with spina bifida cystica
A: Meningomyelocele in the lumbar region - skin-covered sac. B: Myeloschisis - open ulcerated lesion with note of lower limb involvement from nerve damage.

Fig. 17.15 - The Developing Human: Clinically Oriented Embryology
8. Clinical photo - Spina bifida occulta skin sign
A child showing the characteristic hypertrichosis (tuft of hair) in the lumbosacral region - the only external clue to an underlying spina bifida occulta.
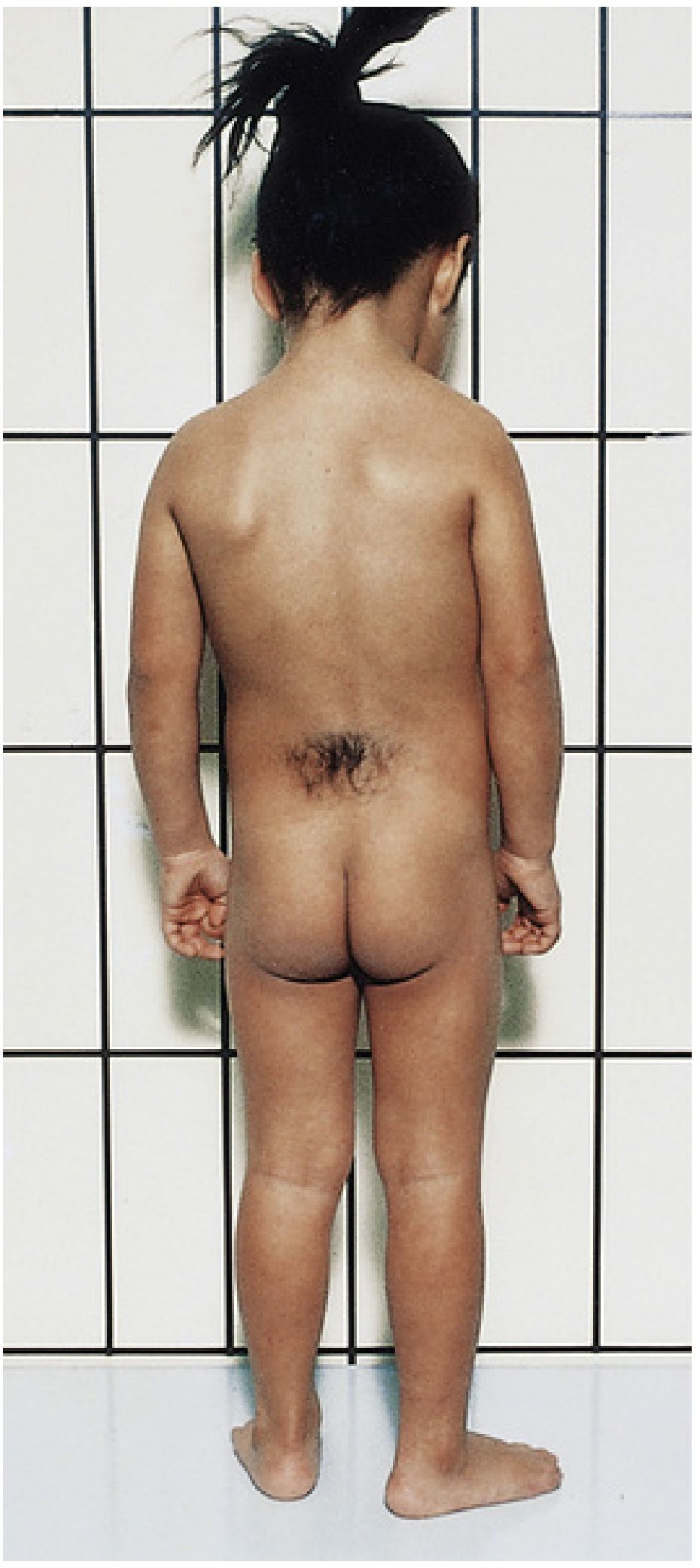
Fig. 17.14 - The Developing Human: Clinically Oriented Embryology
9. MRI comparison - Myelocele vs Myelomeningocele (from previous answer)
Sagittal T1 MRI side-by-side: left = myelocele (neural tissue flush with skin surface); right = myelomeningocele (sac extends beyond skin, contains cord + CSF).
Fig. 385-1 - Goldman-Cecil Medicine
Etiology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive etiology data from five authoritative sources. Here is the full answer:
Etiology of Spina Bifida
Spina bifida has a multifactorial etiology - most cases result from an interaction of genetic susceptibility and environmental/nutritional triggers. A small proportion have a single identifiable cause. The unifying mechanism is failure of posterior neuropore closure by day 26 of embryogenesis.
1. Nutritional Deficiencies
Folate / Folic Acid Deficiency (most important)
The single greatest environmental risk factor is low maternal folate. The risk for NTDs becomes significant when maternal serum folic acid falls below 200 µg/L.
- The mechanism involves impaired recycling of tetrahydrofolate and impaired methylation of homocysteine to methionine
- Elevated homocysteine levels co-occur in mothers of NTD-affected children
- Folic acid supplementation of 400-800 µg/day starting at least 1 month before conception and continuing for 2 months after reduces NTD incidence by >75%
- The CDC recommendation is 0.4 mg/day for all women of childbearing age
- US mandatory fortification of cereals (140 µg/100g flour since 1998) has reduced NTD births by ~1,300/year and overall incidence by 35%
- Folate supplementation is protective only if given before day 28 of pregnancy, when the neural folds are fusing
Thompson & Thompson Genetics and Genomics in Medicine, 9th ed., p. 345
Vitamin B12 Deficiency
Low maternal B12 levels significantly increase NTD risk (independent of folate levels). B12 participates in the same one-carbon metabolism pathway as folate.
Vitamin A
Vitamin A deficiency may play a role in some cases; conversely, vitamin A at pharmacologic doses is also teratogenic.
2. Genetic Factors
MTHFR Gene Mutation
The most common genetic risk factor is a missense variant in MTHFR (methylenetetrahydrofolate reductase) - the 677C>T mutation:
| Genotype | Frequency | Effect |
|---|---|---|
| Heterozygous | Common | Moderate enzyme instability |
| Homozygous | 5-15% of many populations | Significantly reduced MTHFR stability |
- Mothers homozygous for the variant allele are twice as likely to have a child with an NTD
- The variant produces a thermolabile, less stable enzyme that hinders tetrahydrofolate recycling
- Exact mechanism (elevated homocysteine vs. depressed methionine vs. other) remains undefined
- OR = 1.34 (95% CI 1.17-1.54) per Creasy & Resnik's Maternal-Fetal Medicine
Chromosomal Abnormalities
Chromosomal deletions, duplications, and trisomies can all lead to neural tube defects. Examples include trisomy 18 (Edwards syndrome) and trisomy 13.
Single-Gene Mutations
Single gene mutations are uncommon as a cause of isolated NTDs. Most cases are polygenic/multifactorial.
Familial Recurrence
- If one child is affected: recurrence risk rises from 1:1,000 to 40-50:1,000 (a ~30-fold increase per Adams & Victor's Principles of Neurology)
- Prior affected pregnancy carries a 3-5% recurrence risk per Creasy & Resnik
- Anencephaly and spina bifida frequently cluster together in families and share a common pathogenesis
3. Teratogens / Drug Exposures
| Agent | Mechanism | Risk |
|---|---|---|
| Valproic acid | Folate antagonist; disrupts neural fold fusion at day 26 | 1-2% risk of NTD if taken during early pregnancy |
| Carbamazepine | Folate antagonist | ~1% risk |
| Methotrexate | Folate antagonist | High teratogenic risk |
These drugs must be taken during the critical window of neural tube closure (days 17-28 post-conception) to cause the defect.
4. Maternal Medical Conditions
| Condition | Odds Ratio | Notes |
|---|---|---|
| Pre-gestational diabetes (Type 1 & 2) | OR 2.88 (95% CI 1.79-4.65) | Independent risk factor |
| Maternal obesity (BMI ≥30) | OR 1.79 (95% CI 1.51-2.13) | Mechanism unclear |
| Periconceptional fever (≥101°F) | OR 2.4 (95% CI 1.5-4.0) | Hyperthermia disrupts neural tube closure |
Creasy & Resnik's Maternal-Fetal Medicine, Ch. 26
5. Other / Environmental Factors
- Geographic and ethnic variation: incidence ranges from ~1% in Ireland to 0.2% or less in the USA; significant variation by region, season of birth, and social class
- Amniotic bands: a mechanical cause in a small proportion
- Potato blight (Ireland) was historically implicated; the causal factor is believed to be associated nutritional deficiency rather than a direct toxin
Summary: Multifactorial Model
Gene-gene interactions
+
Gene-environment interactions
+
Nutritional deficiency (folate, B12)
+
Teratogen exposure (valproic acid, etc.)
+
Maternal disease (diabetes, obesity)
+
Hyperthermia
=
Failure of posterior neuropore closure by day 26
=
Spina bifida
Most NTDs are isolated defects of unknown cause, but the interaction of folate-pathway genetics (especially MTHFR 677C>T) with inadequate dietary folate is the dominant etiologic model. This explains why folate supplementation, despite being a single nutritional intervention, reduces incidence by more than 75%.
- The Developing Human: Clinically Oriented Embryology, p. 1042-1043
- Thompson & Thompson Genetics and Genomics in Medicine, p. 344-346
- Goldman-Cecil Medicine, Ch. 385 & Ch. 13
- Adams and Victor's Principles of Neurology, Ch. 37
- Creasy & Resnik's Maternal-Fetal Medicine, Ch. 26
Types
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent - comprehensive material gathered. Here is the full classification:
Types of Spina Bifida
Spina bifida is classified based on two systems: (1) the bony defect (whether the posterior vertebral arch is simply unfused vs. open) and (2) the content of the herniation (bone only / meninges only / meninges + cord). The spectrum runs from entirely silent to severely disabling.
Overview Diagram (A-D, all four types)
Fig. 17.12 A-D - The Developing Human: Clinically Oriented Embryology
Type 1: Spina Bifida Occulta
"Hidden" spina bifida - bony defect only, nothing herniates
| Feature | Detail |
|---|---|
| Defect | Failure of posterior vertebral arch(es) to fuse in midline |
| Neural tube | Intact and within the spinal canal |
| Meninges | Not herniated |
| Prevalence | ~10% of the general population |
| Most common level | L5 or S1 |
| Symptoms | Usually none - incidental finding on X-ray |
When to suspect it clinically - look for dorsal midline skin signs:
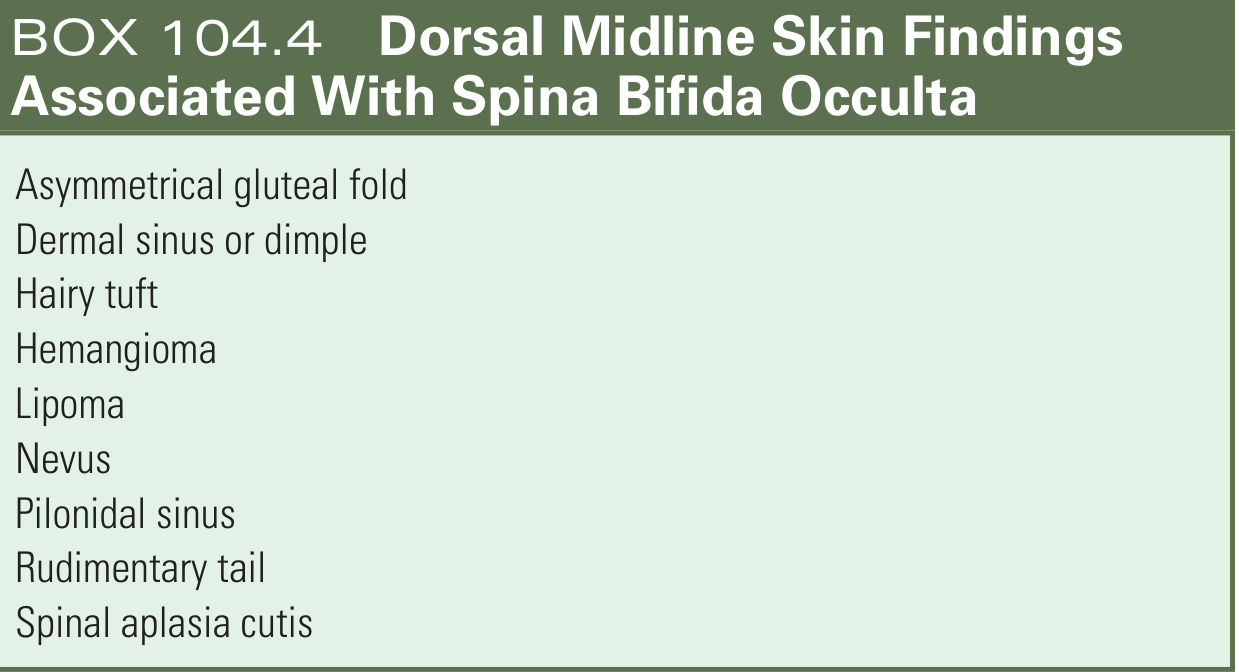
Box 104.4 - Bradley and Daroff's Neurology in Clinical Practice
Skin signs include: hairy tuft, dermal sinus/dimple, hemangioma, subcutaneous lipoma, nevus, pilonidal sinus, asymmetrical gluteal fold, rudimentary tail, spinal aplasia cutis. A few patients have subtle neurological signs if an underlying tethered cord or lipoma is present.
Plain X-ray shows absent spinous process / bifid lamina at the affected level:

eFig. 104.8 - Bradley and Daroff's Neurology in Clinical Practice
MRI showing spina bifida occulta at L5, with sagittal and axial sequences:
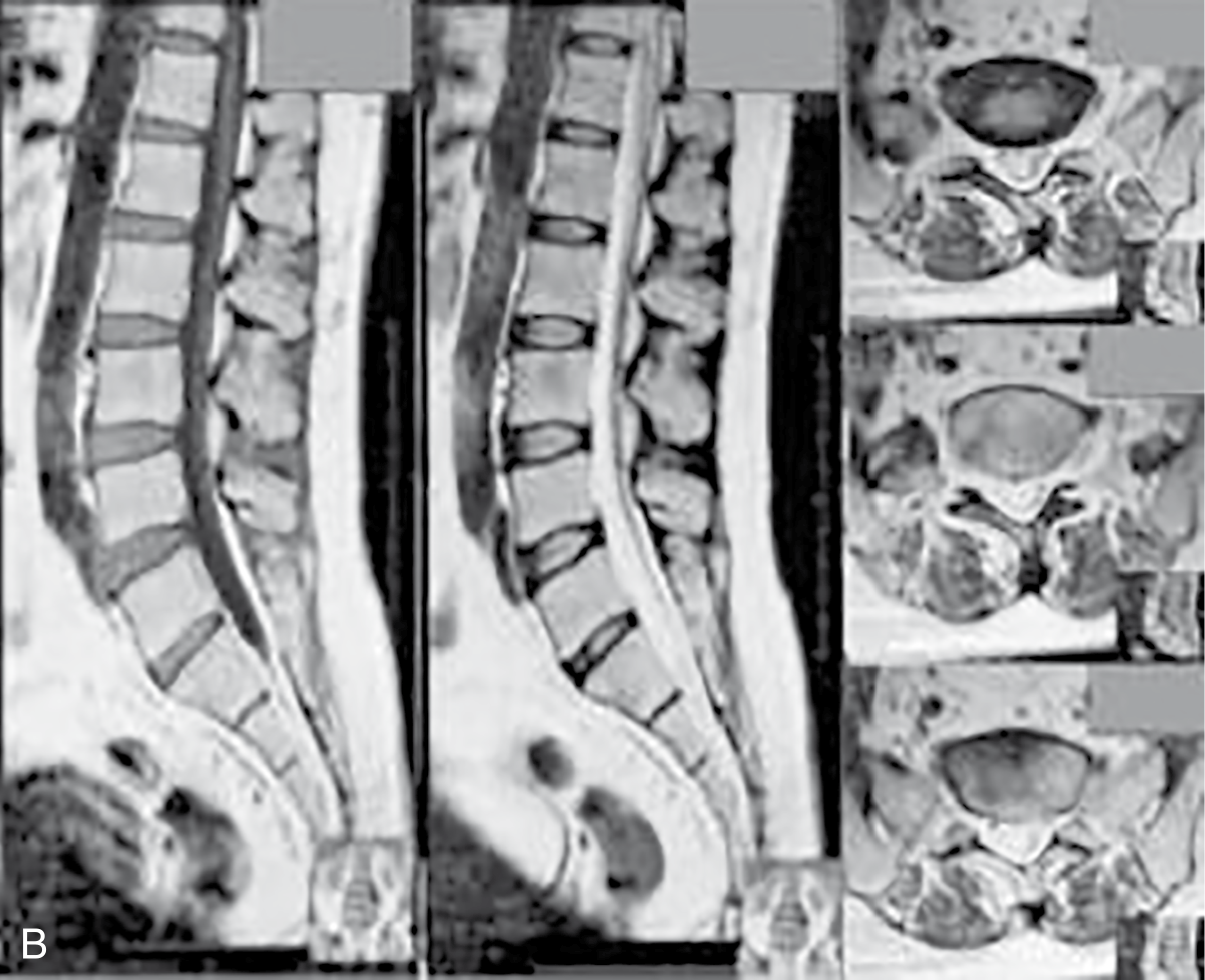
Fig. 36.1B - Campbell's Operative Orthopaedics 15th Ed. 2026
Type 2: Meningocele
Meninges + CSF herniate through the bony defect; spinal cord stays in the canal
| Feature | Detail |
|---|---|
| Defect | Bony arch defect + herniation of dura and arachnoid |
| Content of sac | CSF only (no neural tissue) |
| Spinal cord position | Normal, within canal |
| Skin | Usually covered by skin or thin membrane |
| Neurological deficit | Less common than myelomeningocele; may be none |
| Rarity | Uncommon (meningomyelocele is 10x more frequent) |
Most lesions are posterior/lumbosacral. Rarely, anterior or lateral meningoceles occur.
Sagittal diagram:
Fig. 104.11 - Bradley and Daroff's Neurology in Clinical Practice
Type 3: Myelomeningocele
The most severe and most common open form - cord AND meninges herniate
| Feature | Detail |
|---|---|
| Defect | Open posterior bony defect + herniation of cord + meninges |
| Content of sac | Spinal cord, nerve roots, CSF |
| Skin | Almost always absent over lesion - exposed neural tissue |
| Most common level | Lumbosacral (lower thoracic also possible) |
| Hydrocephalus | 75% of cases |
| Chiari II malformation | Virtually all cases |
| Neurological deficit | Motor + sensory loss below lesion; bowel/bladder dysfunction universal |
The neural placode sits atop the sac. The nerve roots arise from the ventral surface of the placode (everted interior of the neural tube). The thin arachnoid membrane covering breaks down within days, leaving an ulcerated surface.
Sagittal anatomy diagram:
Fig. 104.10 - Bradley and Daroff's Neurology in Clinical Practice
Surgical anatomy (infant + cross-section + sagittal):
Fig. 36.2 - Campbell's Operative Orthopaedics 15th Ed. 2026
MRI - sagittal view (cord + CSF in sac protruding beyond skin):
Fig. 385-1 - Goldman-Cecil Medicine
Type 4: Myeloschisis (Myelocele / Open Myelocele)
Most severe form - neural tissue fully exposed, flush with skin surface, no sac
| Feature | Detail |
|---|---|
| Defect | Wide splaying of vertebral arch, neural tube open |
| Surface | No covering - exposed, ulcerated neural plate |
| Neural position | Flush with or below skin surface (no raised sac) |
| CSF | Leaks directly - high meningitis risk |
| Prognosis | Worst; severe neurological deficit |
Myelocele = exposed neural elements at skin level. Myelomeningocele = exposed elements elevated on a sac. The distinction is visible on MRI (see Goldman-Cecil Fig. 385-1 above).
Type 5: Lipomeningocele (Occult Dysraphism variant)
Spinal cord protrudes into a fat-filled sac under intact skin
| Feature | Detail |
|---|---|
| Defect | Posterior arch defect + fatty (lipomatous) tissue attached to cord |
| Skin | Intact - covered by skin with overlying subcutaneous lipoma |
| Cord | Tethered by lipoma |
| Classification | "Closed" / occult NTD - no CSF leakage |
| Presentation | Tethered cord syndrome: progressive neurological deterioration with growth |
MRI showing lipomyelomeningocele (bright lipoma signal within canal, cord tethering, arrowheads):
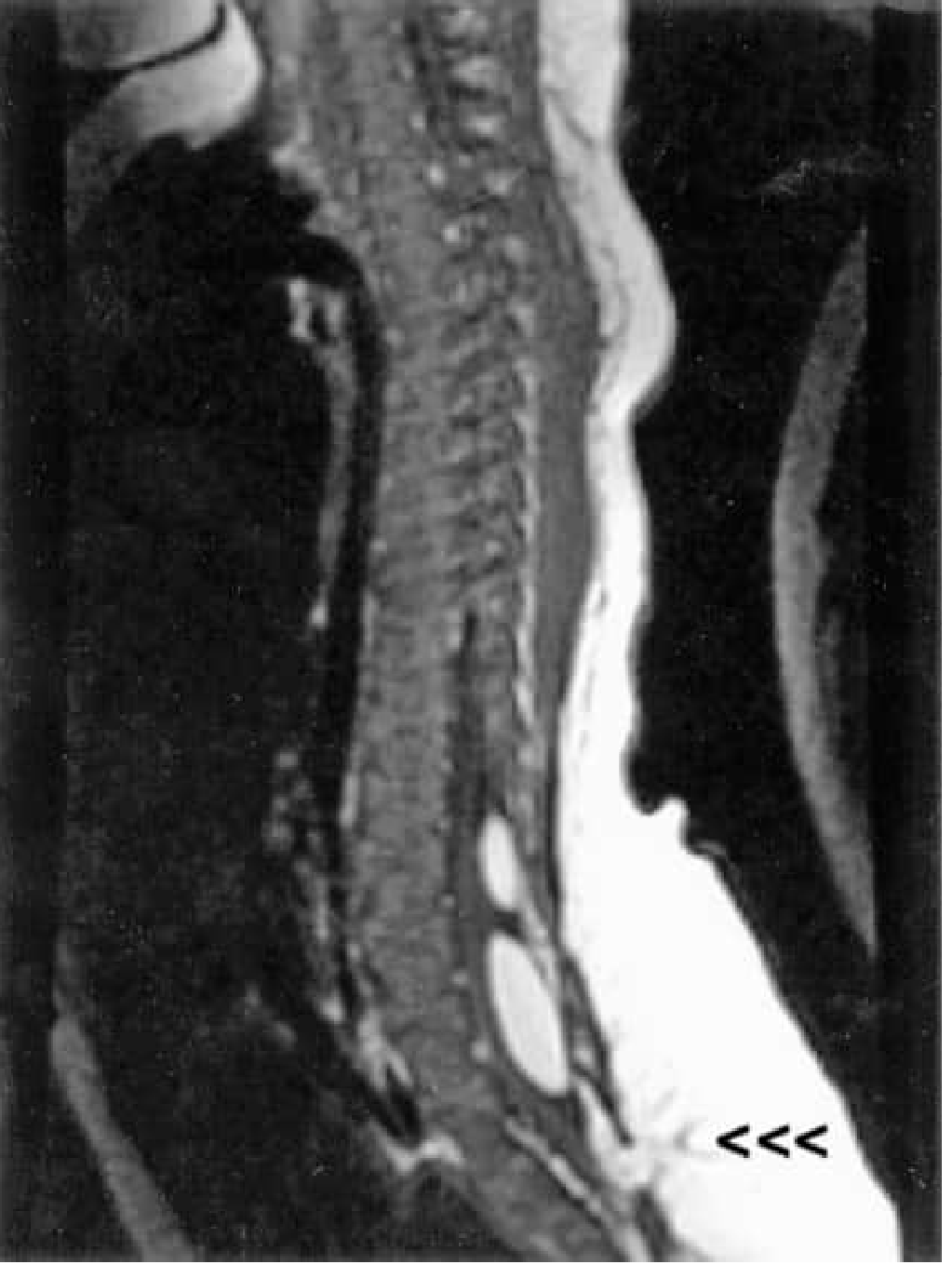
eFig. 104.9 - Bradley and Daroff's Neurology in Clinical Practice
Type 6: Caudal Regression Syndrome
Abnormal formation or agenesis of the sacrum + malformation of the spinal cord
- Associated with maternal diabetes (most strong association)
- Ranges from partial sacral agenesis to complete absence of the lumbosacral spine
- Produces variable lower limb motor/sensory deficits and sphincter dysfunction
Comparative Summary Table
(Campbell's Operative Orthopaedics 15th Ed. 2026, Table 36.2)
| Type | Bony Defect | Sac Contents | Skin | Neural Deficit | Frequency |
|---|---|---|---|---|---|
| Spina bifida occulta | Unfused arch | None | Intact | None / rare | ~10% of population |
| Meningocele | Open arch | CSF only | Skin-covered | Mild / absent | Uncommon |
| Myelomeningocele | Open arch | Cord + roots + CSF | Absent | Moderate-severe | Most common open form |
| Myeloschisis | Wide-open arch | None (cord exposed) | None | Severe | Least common, most severe |
| Lipomeningocele | Occult defect | Cord + fat | Intact | Progressive (tethered cord) | Varies |
| Caudal regression | Sacral agenesis | - | - | Lower limb + sphincter | Rare |
Classification basis (Bradley and Daroff): either the bony vertebral deformity OR the neurological lesion. No deficit = spina bifida occulta or mild meningocele. Motor/sensory/autonomic neuropathy = meningomyelocele. Cord parenchyma herniation = myelodysplasia.
- Campbell's Operative Orthopaedics 15th Ed., Table 36.2
- Bradley and Daroff's Neurology in Clinical Practice, Ch. 104
- The Developing Human: Clinically Oriented Embryology, Ch. 17
- Goldman-Cecil Medicine, Ch. 385
Investigations
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
All key images and content are now gathered. Here is the comprehensive answer:
Investigations in Spina Bifida
Investigations fall into two phases: prenatal (to detect and characterise before birth) and postnatal (to define anatomy, complications, and functional impact after birth).
A. PRENATAL INVESTIGATIONS
1. First-Trimester Screening (11-14 weeks)
Nuchal Translucency Ultrasound + Posterior Brain Assessment
During the routine 11-14 week scan, abnormal appearance of the posterior brain in the midsagittal plane can indicate high risk for open spina bifida and should prompt early anatomy imaging at 15-16 weeks.
Three fluid spaces are normally seen in the posterior brain: the brainstem (BS), fourth ventricle (4TH), and cisterna magna (CM):
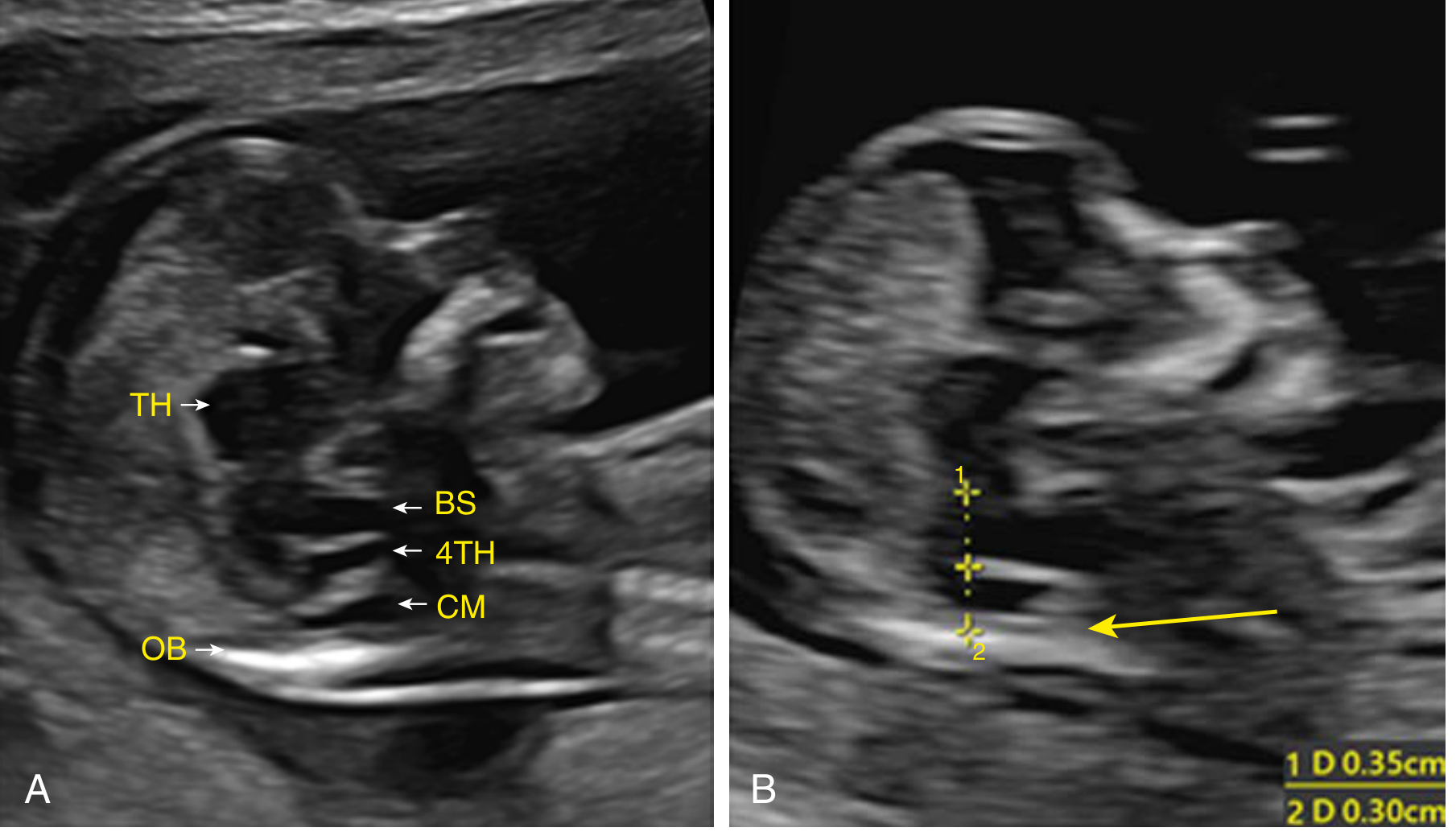
Fig. 26.57 - Creasy & Resnik's Maternal-Fetal Medicine
- Qualitative non-visualisation of cisterna magna: sensitivity 76.5%, specificity 99.6%
- Quantitative BS-BSOB ratio >1 (>95th percentile for CRL): sensitivity 84.5%, specificity 96.3%
2. Maternal Serum Alpha-Fetoprotein (AFP) (15-18 weeks)
- AFP is produced by the fetal liver and yolk sac; it normally does not pass freely into amniotic fluid
- In open NTDs, AFP leaks through the exposed neural tissue into amniotic fluid, and from there into maternal serum
- Screening cut-off: typically 2.5 multiples of the median (MoM) or 95th centile
- Detects ~75% of open spina bifida cases
- AFP is normal in closed/skin-covered lesions (spina bifida occulta, lipomeningocele)
Causes of raised maternal serum AFP (not all are NTDs):
- Anencephaly / open spina bifida
- Incorrect gestational age
- Intrauterine fetal bleed / threatened miscarriage
- Twin pregnancy
- Exomphalos / gastroschisis
- Sacrococcygeal teratoma
Emery's Elements of Medical Genetics, p. 337
3. Second-Trimester Anomaly Ultrasound (18-20 weeks) - PRIMARY TOOL
Ultrasound has superseded maternal serum AFP screening as the primary prenatal detection method. It detects >90% of NTDs at 18-20 weeks (combined with AFP >95%).
The spine is routinely imaged in axial, sagittal, and coronal planes.
Spinal (Direct) Signs
Sagittal view - disruption of the dorsal spine with an overlying cystic mass:
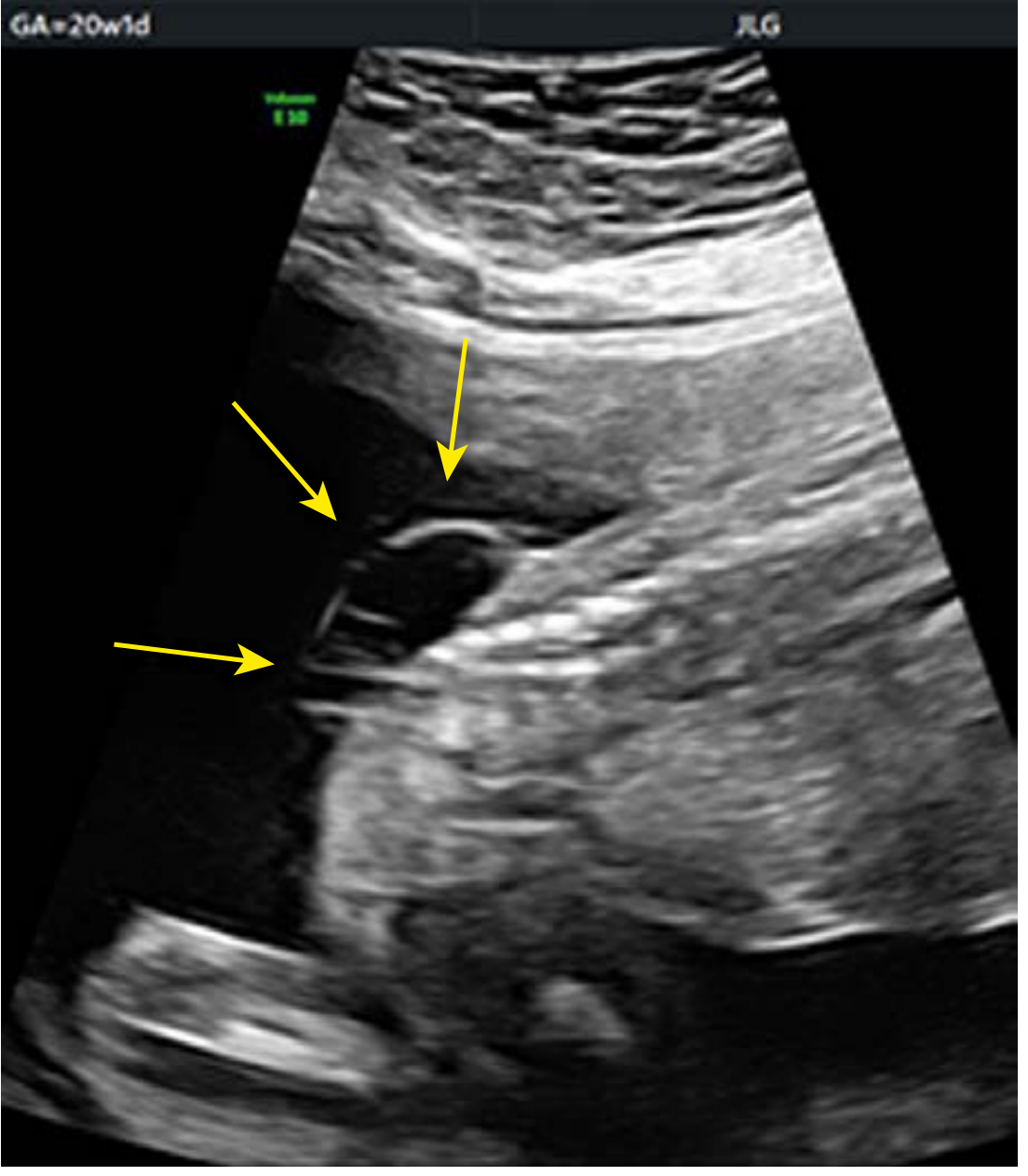
Fig. 26.49 - Creasy & Resnik's Maternal-Fetal Medicine
Axial view - V-shaped or U-shaped (splayed) posterior vertebral elements:
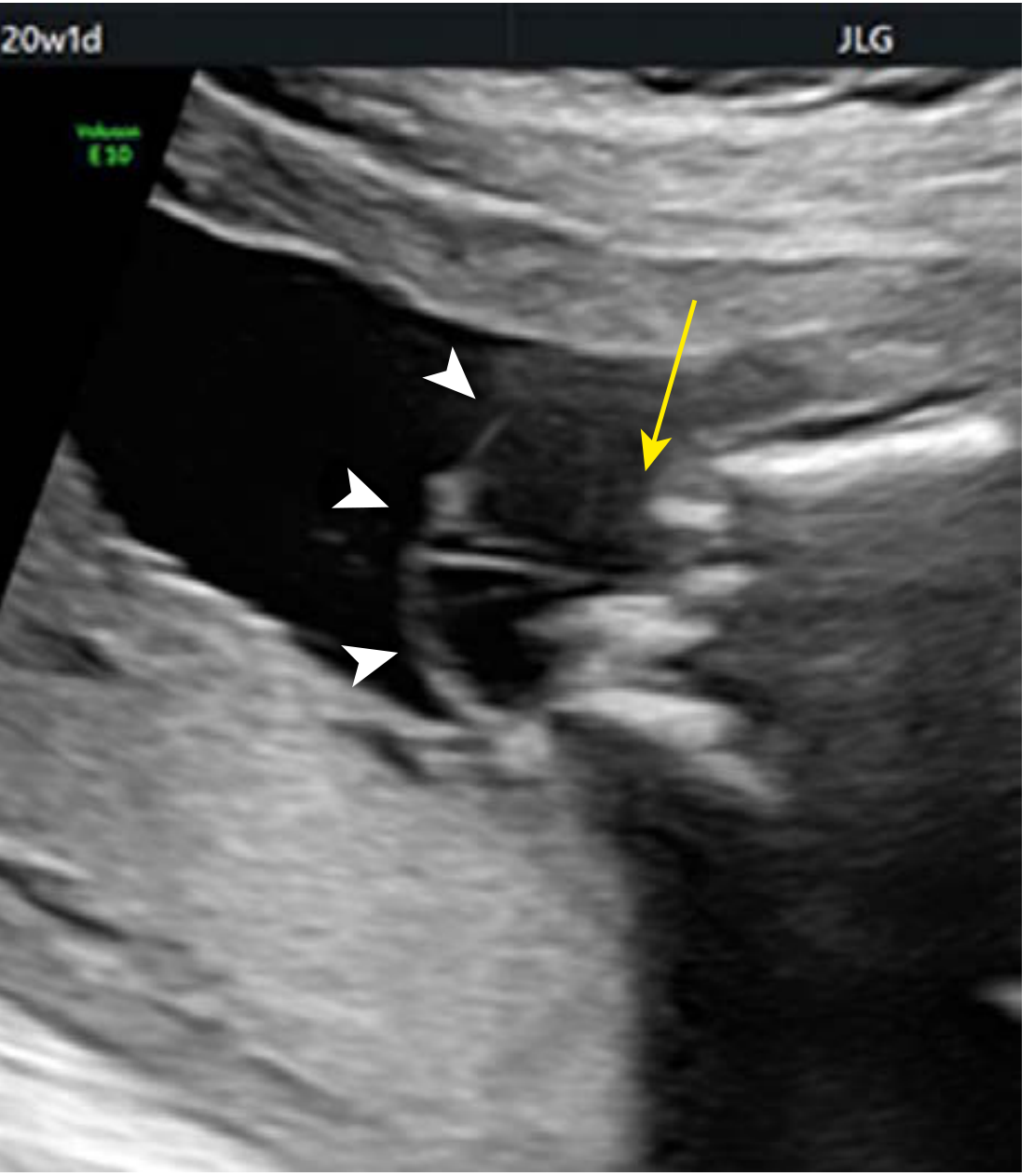
Fig. 26.50 - Creasy & Resnik's Maternal-Fetal Medicine
Myeloschisis (no sac) - sagittal view shows spine defect without a cystic covering structure:

Fig. 26.52 - Creasy & Resnik's Maternal-Fetal Medicine
Cranial (Indirect) Signs - due to Chiari II malformation
These are indirect markers of open NTDs visible on the fetal head, caused by CSF leaking downward, creating traction on the hindbrain:
| Sign | Appearance | Frequency |
|---|---|---|
| Banana sign | Cerebellar hemispheres pulled into a curved "banana" shape; effacement/obliteration of cisterna magna | 50-100% |
| Lemon sign | Frontal bone scalloping - skull appears "pinched" anteriorly, resembling a lemon | 53-100% |
| Ventriculomegaly | Atrial width ≥10 mm | 45-89% |
| Hypoplastic cerebellum | Small cerebellum | 82-96% |
| Dolichocephaly | Elongated skull shape | 53% |
| Microcephaly | Head circumference <5th percentile | 71% |
| Abnormal corpus callosum | Aberrant development | 70-90% |
Cranial ultrasound showing lemon sign + banana sign at 20 weeks:
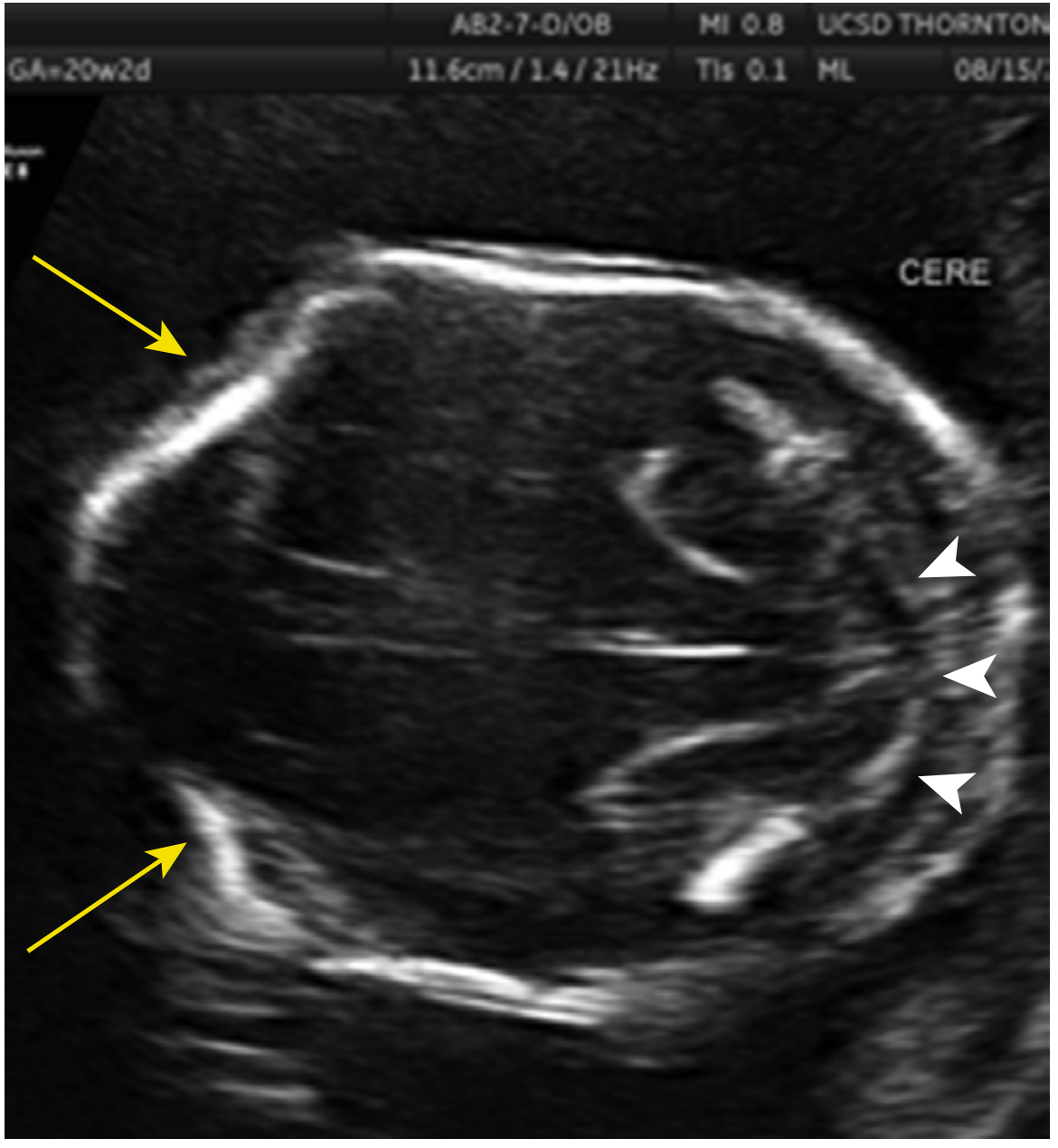
Fig. 26.58 - Creasy & Resnik's Maternal-Fetal Medicine
The lesion level is defined as the highest vertebral level at which dysraphism is visible. >80% of defects are lumbosacral; can also occur cervically or thoracically.
4. Amniocentesis
Indicated when:
- Elevated maternal serum AFP
- Ultrasound is inconclusive
- No abnormality on ultrasound despite elevated AFP
Amniotic fluid tests:
| Test | What it detects | Significance |
|---|---|---|
| AFP (amniotic fluid) | Elevated in open NTDs | Highly sensitive |
| Acetylcholinesterase (AChE) | Normally in CSF only, NOT in amniotic fluid | Confirmatory test; very specific for open NTDs |
| Karyotype / microarray | Chromosomal anomalies | Aneuploidy in ~10% (trisomy 18, 13, triploidy) |
| NIPT (cell-free DNA) | Chromosomal screening | Non-invasive alternative |
- Campbell's Operative Orthopaedics, p. 1658
- Creasy & Resnik's Maternal-Fetal Medicine, Ch. 26
5. Fetal MRI
- Used adjunctively to ultrasound when anatomy is unclear
- Superior soft-tissue resolution for neural placode, lesion level, and brain abnormalities
- Ultrafast sequences avoid movement artefact
- Helps characterise Chiari II, corpus callosum, and ventriculomegaly in detail
- 3D ultrasound and fetal MRI can precisely define bony defect span and lesion level
6. Fetal Echocardiogram
- Recommended when ONTD is confirmed
- 15-30% of euploid fetuses with ONTD have additional anomalies including cardiac defects
- VACTERL association (vertebral, anorectal, cardiac, tracheo-oesophageal, renal, limb) must be excluded
B. POSTNATAL INVESTIGATIONS
1. Clinical Examination
- Visible midline back lesion at birth confirms open NTD
- Neurological assessment: level of motor/sensory deficit, reflex testing
- Head circumference for hydrocephalus
- Skin signs for occult dysraphism (hairy tuft, dimple, lipoma)
2. MRI - Brain and Spine (first-line postnatal imaging)
- Brain MRI: confirms hydrocephalus, Chiari II malformation, corpus callosum abnormalities, cortical malformations
- Spine MRI: defines neural placode anatomy, lesion extent, tethered cord, lipoma, syrinx
- Sagittal T1 MRI (from Goldman-Cecil, Fig. 385-1) distinguishes myelocele from myelomeningocele
3. Cranial Ultrasound (neonates)
- Portable, bedside assessment of ventricular size
- Monitors for progressive hydrocephalus pre- and post-VP shunt
4. Plain X-ray - Spine
- Shows absent/bifid posterior elements
- Useful for spina bifida occulta (incidental finding)
- Monitors scoliosis, kyphosis, hip dislocation
5. Urological Investigations (all patients)
- Renal ultrasound: baseline renal anatomy, hydronephrosis from neuropathic bladder
- Urodynamic studies: bladder compliance, detrusor overactivity, sphincter dysfunction
- VCUG (voiding cystourethrogram): vesico-ureteric reflux
- Urine culture: frequent UTIs are a major long-term morbidity; can progress to renal failure
6. Electrophysiological Tests
- MRI + urodynamics are preferred over older EMG/NCS for spinal cord level determination
- Somatosensory evoked potentials may be used in complex cases
7. Neuropsychological Assessment
- Cognitive testing: ~65% of myelomeningocele patients have normal intelligence
- Learning disability and processing difficulties are common even with normal IQ
- Required before school entry and at key developmental stages
Summary Algorithm
PRENATAL
1st trimester (11-14w): Nuchal US + posterior brain assessment
↓
15-18 weeks: Maternal serum AFP
↓ (elevated or suspicious)
18-20 weeks: Anomaly USS → spinal signs + cranial signs
↓ (confirmed/uncertain)
Amniocentesis: AFP + AChE + karyotype
Fetal MRI (adjunctive)
Fetal echo
POSTNATAL
At birth: Clinical exam + cranial USS
MRI brain + spine (definitive)
Ongoing: X-ray, urodynamics, renal USS,
neuropsychological testing
- Creasy & Resnik's Maternal-Fetal Medicine, Ch. 26
- Campbell's Operative Orthopaedics 15th Ed., Ch. 36
- Goldman-Cecil Medicine, Ch. 385
- Emery's Elements of Medical Genetics, Ch. 20
- Thompson & Thompson Genetics and Genomics in Medicine, Ch. 18
Clinical features
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
This is a shared conversation. Sign in to Orris to start your own chat.