Complete obstetrics hemorrhage from ten teachers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete, detailed answer on obstetric hemorrhage as covered in "Ten Teachers" style (the classical UK obstetrics approach), using the best available textbook sources.
Obstetric Haemorrhage - Complete Notes
Based on Creasy & Resnik's Maternal-Fetal Medicine, Rosen's Emergency Medicine, Roberts & Hedges' Clinical Procedures, and related authoritative sources - aligned with the Ten Teachers framework
Overview and Epidemiology
Obstetric haemorrhage is the leading cause of maternal death worldwide and the leading cause of severe maternal morbidity in resource-rich countries. In the United States, haemorrhage accounts for more than 10% of maternal deaths (cause-specific MMR: 1.6/100,000). The UK achieves a lower rate of 0.4/100,000 through systematic protocols and multidisciplinary care.
Key institutional failures identified in case reviews include:
- No haemorrhage response team or plan
- Delay and denial (assuming bleeding will self-resolve)
- Lack of familiarity with blood component therapy
Rates of haemorrhage and blood transfusion use have risen in all resource-rich countries, driven primarily by increasing uterine atony and the placenta accreta spectrum.
Part I: Antepartum Haemorrhage (APH)
APH is defined as bleeding from the genital tract after 24 weeks of gestation and before delivery. The two classic causes are placenta praevia and placental abruption.
Critical rule: Until placenta praevia is excluded, digital vaginal examination is absolutely contraindicated - it can tear or dislodge the placenta causing fatal haemorrhage. Use ultrasound first.
1. Placenta Praevia
Definition and Classification
Placenta praevia occurs when the placenta implants in the lower uterine segment, partially or completely covering the internal cervical os.
Traditional classifications (now largely replaced by ultrasound-based terminology):
- Complete (Central) praevia - placenta covers the os completely
- Partial praevia - placenta partially covers the os
- Marginal praevia - placental edge reaches the margin of the os
- Low-lying placenta - placenta is close to but not covering the os
With transvaginal ultrasound (TVUS), the diagnosis is redefined: a clinically significant abnormality exists when the placenta covers the cervix completely or extends close enough to cause bleeding during cervical dilatation or lower segment effacement.
Pathogenesis
The underlying cause is unknown, but there is a clear association with prior endometrial damage and uterine scarring:
| Risk Factor | Increased Risk |
|---|---|
| Previous placenta praevia | 8× |
| Previous caesarean section | 1.5-153× |
| Previous suction curettage for abortion | 1.33× |
| Age >35 years | 4.73× |
| Age >40 years | 9× |
| Multiparity | 1.1-1.73× |
Placental migration: At least 90% of placentas identified as low-lying in early pregnancy resolve by the third trimester. The placenta grows toward the better blood supply at the fundus (trophotropism), while the distal lower segment portions atrophy. As the uterus grows, differential growth of the lower segment further increases the distance from cervix to placental edge.
Mechanism of bleeding: As the lower uterine segment develops and the cervix effaces, the placenta is forced to separate from the underlying decidua. Prelabour contractions, intercourse, or vaginal examination can also precipitate bleeding.
Diagnosis
Classic presentation: Painless, bright-red vaginal bleeding in the third trimester - often preceded by small "herald bleeds." In up to 10% of cases, there is no bleeding until labour onset.
- Transabdominal ultrasound: 96% accuracy for placental localisation - first-line investigation
- Transvaginal ultrasound (TVUS): More precise; allows measurement of distance from placental edge to internal os
- Digital vaginal exam: CONTRAINDICATED until praevia is excluded
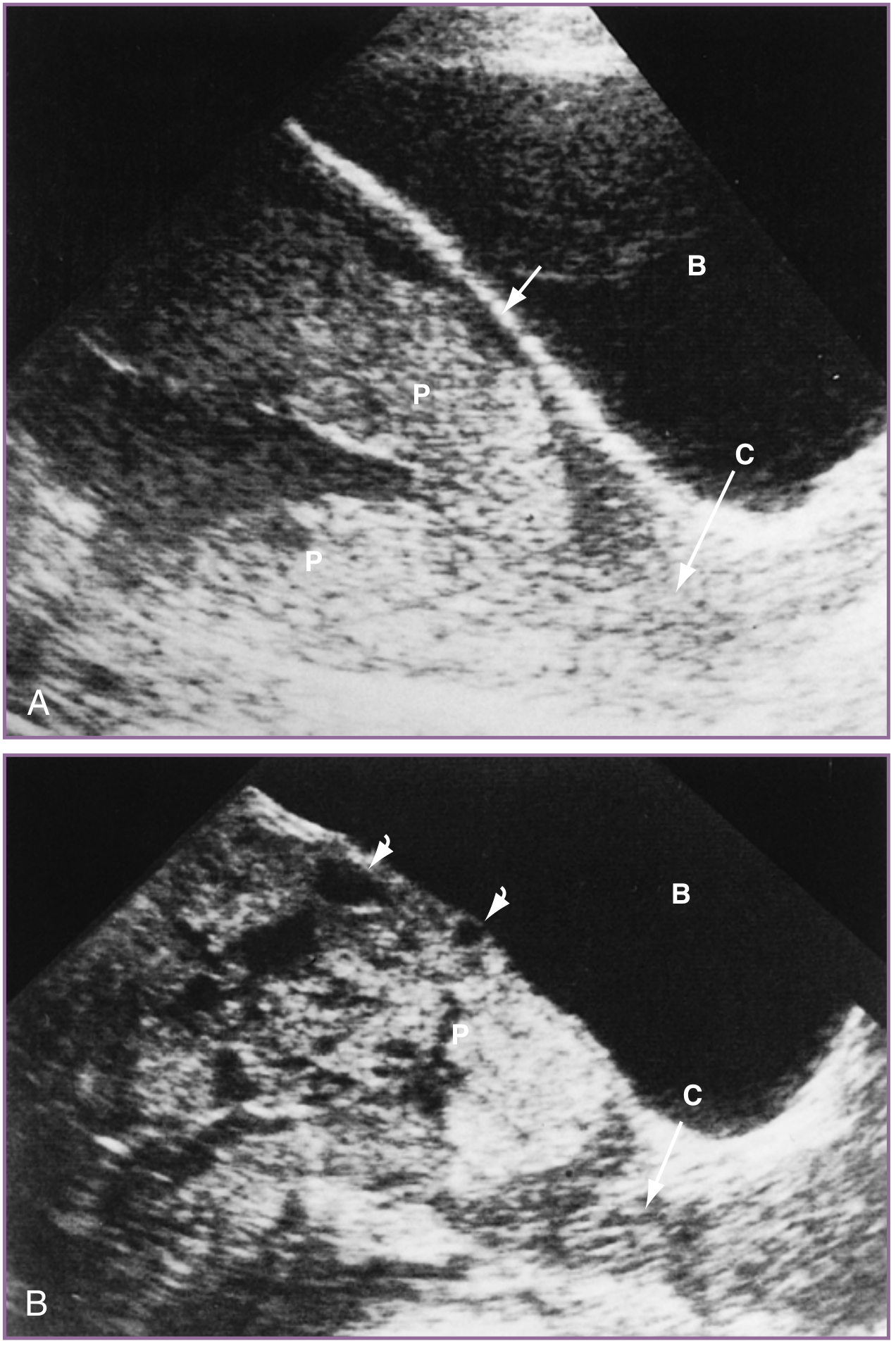
Ultrasound of normal placenta vs placenta accreta - Creasy & Resnik's Maternal-Fetal Medicine
Management
- Admit and assess haemodynamic stability
- Large-bore IV access, FBC, group & cross-match
- Corticosteroids if <34 weeks
- Delivery by caesarean section (avoid the placenta with fundal incision)
- In suspected placenta accreta spectrum (PAS): deliver in a tertiary centre with massive transfusion protocol (MTP) available; planned caesarean hysterectomy
2. Placental Abruption (Abruptio Placentae)
Definition
Premature separation of a normally sited placenta from the uterine wall before delivery of the fetus. Occurs in approximately 1 in 129 births.
Presentation - Classic contrast with praevia
| Feature | Placenta Praevia | Placental Abruption |
|---|---|---|
| Pain | Painless | Painful (sudden, severe abdominal pain) |
| Bleeding | Bright red, revealed | Dark red; may be concealed |
| Uterus | Soft, non-tender | Hard, "woody," tender |
| Fetal heart | Usually normal | Fetal distress common |
| Coagulopathy | Uncommon | Common (DIC in severe cases) |
Concealed haemorrhage is particularly dangerous - bleeding is trapped behind the placenta and does not appear vaginally, so the clinical picture (shock, hard uterus) may appear out of proportion to visible blood loss.
Risk Factors
- Hypertension (chronic or pre-eclampsia)
- Cocaine use (strong association)
- Trauma (road traffic accidents, domestic abuse)
- Smoking
- Previous abruption (recurrence risk ~10%)
- Thrombophilia (particularly prothrombin gene mutation - OR up to 8.9)
Complications
- DIC: Thromboplastin released from the retroplacental clot enters the maternal circulation, consuming clotting factors - resulting in hypofibrinogenaemia, thrombocytopenia, and elevated fibrin split products/D-dimer
- Fetal hypoxia and death
- Couvelaire uterus (extravasation of blood into myometrium - uterus appears blue-purple)
- Renal cortical necrosis (from prolonged hypoperfusion)
Diagnosis and Management
- Clinical diagnosis; ultrasound has limited sensitivity (negative predictive value 63-88% - do NOT use to exclude abruption)
- Bloods: FBC, coagulation screen including fibrinogen, urea & electrolytes, LFTs, group & cross-match, toxicology screen (cocaine)
- Immediate obstetric referral
- Aggressive resuscitation; MTP if severe
- Delivery - mode and timing depend on fetal condition and severity of abruption
Part II: Postpartum Haemorrhage (PPH)
PPH is the most common complication of labour and delivery and accounts for up to 11% of obstetric deaths.
Definition
- Primary PPH: Blood loss >500 mL within the first 24 hours after vaginal delivery (>1000 mL after caesarean section)
- Secondary PPH: Haemorrhage from 24 hours to 6 weeks after delivery
Important: Because of maternal physiological adaptations during pregnancy (increased blood volume of ~45%), the patient may not show signs of shock until more than 1500 mL of volume has been lost.
The "Four Ts" - Causes of PPH
| Cause | "T" | Frequency |
|---|---|---|
| Uterine atony | Tone | 75-90% of cases |
| Genital tract trauma | Trauma | ~20% of cases |
| Retained placental tissue / abnormal placentation | Tissue | ~10% of cases |
| Coagulopathy (DIC, dilutional) | Thrombin | Variable |
1. Uterine Atony (TONE) - Most Common Cause
Mechanism: Failure of myometrial contraction after delivery. Normally, contraction of the myometrium constricts the spiral arteries at the placental implantation site, limiting blood loss. If the uterus fails to contract, ongoing haemorrhage occurs.
Examination: Soft, boggy uterus palpable on abdominal examination (large "doughy" mass)
Predisposing factors:
- Overdistended uterus: multiple gestation, macrosomia, polyhydramnios
- Prolonged labour
- Chorioamnionitis
- Tocolytic use
- General anaesthesia with halogenated agents
- Grand multiparity
Management (stepwise):
- Bimanual uterine massage - one hand transabdominally, one through the introitus supporting the uterus
- Uterotonics:
- Oxytocin 10 units IM following placental delivery; IV: 5-10 units bolus then infusion 10 units/hr (max 40 units total)
- Ergometrine/Syntometrine (contraindicated in hypertension)
- Misoprostol (prostaglandin E1) - 800-1000 mcg rectally/sublingually
- Carboprost (prostaglandin F2α) 250 mcg IM (contraindicated in asthma)
- Tranexamic acid 1g IV - demonstrated efficacy in reducing PPH mortality in the WOMAN trial; should be given early
- Intrauterine balloon tamponade (e.g., Bakri balloon)
- Uterine compression sutures (B-Lynch suture)
- Pelvic vessel embolisation by interventional radiology (success rate 95-100%, preserves fertility)
- Uterine packing - sterile gauze or Foley catheter for tamponade
- Peripartum hysterectomy as last resort
2. Genital Tract Trauma (TRAUMA) - Second Most Common
Accounts for up to 20% of PPH cases.
Associated factors: Uncontrolled delivery, macrosomia, episiotomy, nulliparity, coagulopathy, operative delivery (forceps/ventouse), prolonged second stage, pre-eclampsia, malpresentation.
Sites of trauma:
- Perineal lacerations - classified by degree:
- 1st degree: perineal skin and vaginal mucosa only
- 2nd degree: extends into fascia and muscles of the perineal body
- 3rd degree: extends into the anal sphincter
- 4th degree: extends through all layers including rectal mucosa
- Vaginal and cervical lacerations
- Vulval and perineal haematomas (can be concealed - watch for uterine displacement)
Management:
- First- and second-degree tears: repair at bedside with absorbable sutures
- Third- and fourth-degree tears: repair in operating theatre by obstetrician
- Haematomas: expectant (small), bedside repair, or vascular embolisation depending on size/stability
3. Retained Placenta / Abnormal Placentation (TISSUE)
Retained Products of Conception
Approximately 10% of PPH cases are due to retained placental tissue. Retained fragments prevent myometrial constriction and sustain bleeding. Risk factors include aggressive cord traction during third stage, succenturiate (accessory) lobe.
Diagnosis: Incomplete placenta inspection; ultrasound shows expanded endometrium or solid echogenic mass.
Management:
- Manual removal of placenta under regional or general anaesthesia
- Digital uterine exploration/blunt dissection
- Curettage if fragments remain
Placenta Accreta Spectrum (PAS)
| Condition | Depth of Invasion | Notes |
|---|---|---|
| Placenta accreta | Adheres to myometrium, no invasion of decidua basalis | Most common (78-79%) |
| Placenta increta | Villi invade into myometrium | ~14% |
| Placenta percreta | Penetrates full thickness of myometrium (into bladder, bowel) | Most severe (~7%) |
Current incidence: ~3/1000 deliveries (rising due to increasing caesarean section rates).
Risk factors: Prior CS + placenta praevia (synergistic risk), multiparity, prior curettage, uterine anomalies.
Management:
- Prenatal diagnosis by ultrasound (absence of retroplacental clear space, intraplacental lacunae); MRI for extent
- Deliver at a tertiary centre (outcomes significantly improved)
- Planned caesarean hysterectomy at 34-35 weeks (leave placenta in situ, do not attempt manual removal)
- Massive transfusion protocol on standby
- Fundal uterine incision to avoid the placenta
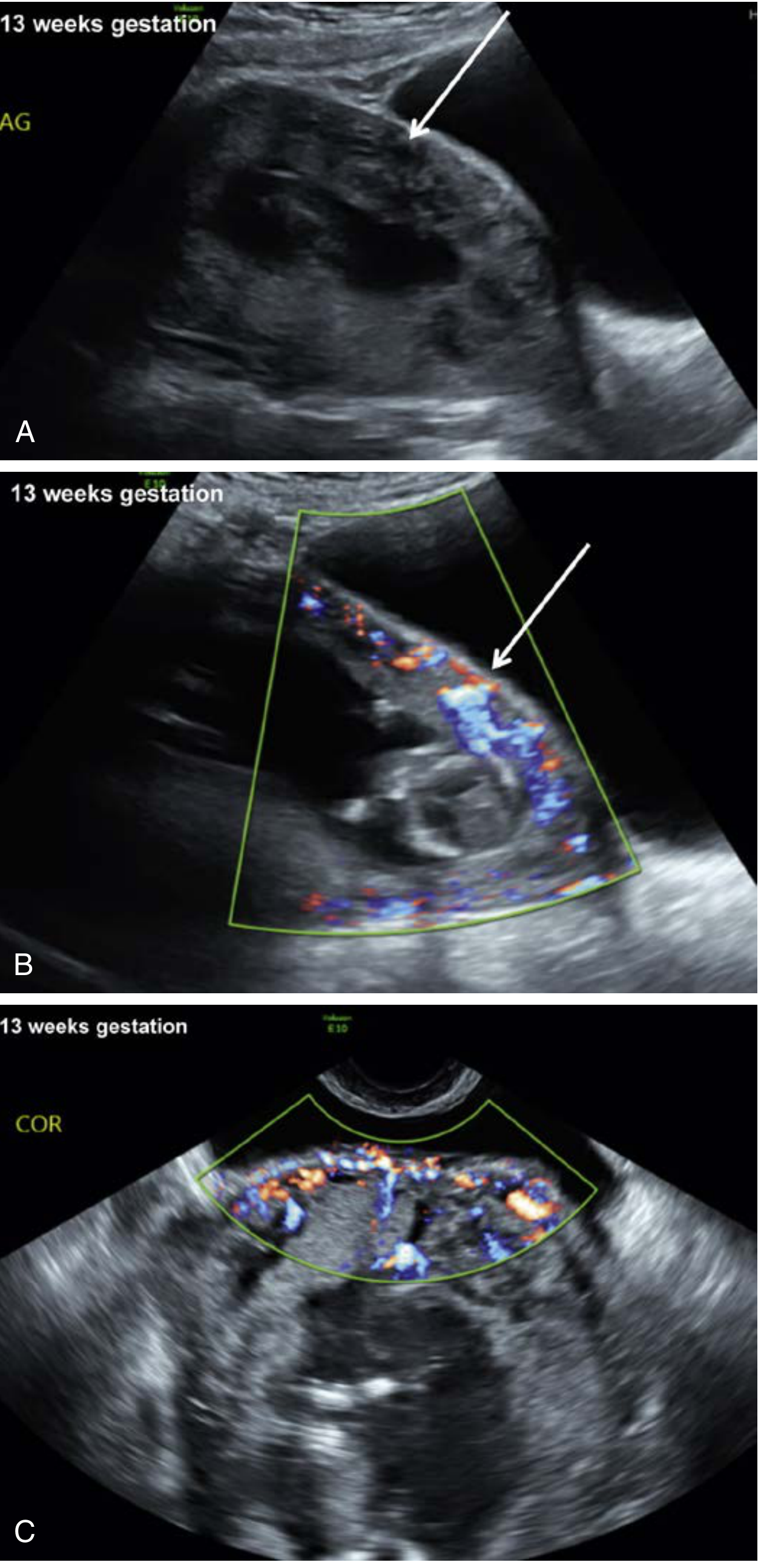
Characteristic first-trimester ultrasound of placenta accreta - Creasy & Resnik's Maternal-Fetal Medicine
4. Coagulopathy (THROMBIN)
All women with PPH should receive tranexamic acid 1g IV.
DIC can complicate PPH and can also cause it. Triggers include:
- Placental abruption
- Pre-eclampsia/eclampsia
- Amniotic fluid embolism (AFE)
- Postpartum infection/sepsis
- Dilutional coagulopathy from aggressive volume resuscitation
- Retained products / dead fetal tissue (excess thromboplastin)
Laboratory findings in DIC: Low fibrinogen, thrombocytopaenia, elevated fibrin degradation products (FDPs), elevated D-dimer, prolonged PT and APTT.
Management: Haemodynamic support + correct coagulopathy (FFP, cryoprecipitate, platelets, recombinant factor VIIa for severe refractory cases).
Part III: Other Major Causes of Obstetric Haemorrhage
Uterine Inversion
A rare but catastrophic complication where the uterus turns inside out.
Clinical features: Sudden severe abdominal pain, absence of uterine corpus on examination, profuse bleeding, haemodynamic instability, uterus visible at cervical os or introitus.
Management:
- Aggressive fluid resuscitation
- Do NOT remove the placenta if still adherent before repositioning (increases haemorrhage)
- Immediately withhold all uterotonics (cervical ring prevents repositioning)
- Manual repositioning - push fundus upward through introitus
- If cervical ring present: uterine relaxation with terbutaline 0.25 mg IV/SC or magnesium sulphate 4-6g IV over 15-20 min
- Once repositioned: restart uterotonics (oxytocin + prostaglandins), maintain firm manual pressure
- Halogenated anaesthetics (surgical option) for refractory cervical ring relaxation
Uterine Rupture
Occurs in approximately 1% of VBAC (vaginal birth after caesarean) deliveries after a single previous CS; higher with multiple prior CS.
Clinical features: Ranges from abnormal fetal heart rate patterns to frank maternal haemorrhagic shock. The most reliable sign of fetal extrusion is prolonged fetal heart rate deceleration. Pain may be absent.
Risk factors: Prior uterine surgery (most common), multiple gestation, trauma, prostaglandin administration.
Outcomes: Minimal fetal extrusion - perinatal mortality <1%; complete fetal extrusion - 10-20% mortality. Significant haemorrhage in 1/3 of cases.
Management: Emergency laparotomy, repair or hysterectomy depending on extent.
Amniotic Fluid Embolism (AFE)
Frequency: 2-6 per 100,000 live births; mortality 15-40%.
Presentation: Sudden cardiovascular collapse during labour/delivery, followed by profuse bleeding and DIC. May present with milder oxygen desaturation. 70% occur during labour, remainder immediately after delivery.
Management (Box from Creasy & Resnik):
- Consider AFE in differential for sudden cardiovascular collapse in pregnancy
- Immediate cardiopulmonary support (intubation + vasopressors)
- Initiate massive transfusion protocol (emphasise large quantities of coagulation factors)
- Early transthoracic echocardiography - treat right ventricular failure
- Consider venoarterial ECMO for refractory ventricular dysfunction
- If occurs during pregnancy with viable fetus: expedited delivery
Part IV: Prevention and Institutional Safety
NPMS Safety Bundle (Four Components)
| Component | Examples |
|---|---|
| Readiness | Haemorrhage response team, MTP in place, staff familiar with uterotonics/balloons/compression sutures |
| Recognition | Risk-assess ALL delivering women, clinical triggers identified |
| Response | Activate protocol promptly, avoid delay and denial |
| Reporting & Systems Learning | Case review, morbidity/mortality meetings |
Key evidence: A 2015-16 California study across 99 hospitals using this bundle achieved a 20.8% reduction in severe maternal morbidity in women with haemorrhage.
Risk Stratification for PPH
All delivering women should be assessed for PPH risk:
- High risk: previous PPH, PAS, placenta praevia, coagulopathy, >4 previous deliveries, large fibroids, pre-eclampsia
- Active management of third stage (oxytocin 10 IU IM routinely at delivery of anterior shoulder) is the single most effective preventive measure
Tranexamic Acid
The WOMAN trial (a major RCT) demonstrated efficacy of tranexamic acid in reducing maternal death related to PPH versus placebo. It should be integrated into institutional protocols and administered early (1g IV, can repeat if bleeding continues after 30 minutes).
Quick Reference Summary
OBSTETRIC HAEMORRHAGE AT A GLANCE
ANTEPARTUM HAEMORRHAGE (after 24 weeks)
├── Placenta Praevia
│ ├── Painless bright-red bleeding
│ ├── Soft uterus
│ ├── NO digital examination
│ └── USS → CS delivery
└── Placental Abruption
├── Painful, dark/concealed bleeding
├── Woody hard uterus, tender
├── Risk of DIC
└── Fibrinogen + coag screen essential
POSTPARTUM HAEMORRHAGE (>500 mL <24h)
The 4 Ts:
├── TONE (75-90%) → Uterine atony
│ └── Bimanual massage → Oxytocin →
│ Ergometrine → Misoprostol →
│ TXA → Balloon → Surgery
├── TRAUMA (20%) → Lacerations/Haematomas
│ └── Repair by degree
├── TISSUE (10%) → Retained placenta / PAS
│ └── Manual removal / Hysterectomy
└── THROMBIN → DIC
└── Blood products + TXA
OTHER
├── Uterine Inversion → Withhold uterotonics, reposition
├── Uterine Rupture → Emergency laparotomy
└── AFE → CPR + MTP + ECMO if needed
Sources: Creasy & Resnik's Maternal-Fetal Medicine (9780323828499); Rosen's Emergency Medicine (9780323757898); Roberts & Hedges' Clinical Procedures in Emergency Medicine (9780323354783); Barash et al. Clinical Anaesthesia (9781975199074)
Note: "Obstetrics by Ten Teachers" (20th Ed.) is the classic UK undergraduate text. The core content above aligns directly with its structure and approach. The specific textbook was not available in the library database, but all material is drawn from equivalent authoritative sources covering the identical clinical content.
This is a shared conversation. Sign in to Orris to start your own chat.