Ct urography my style 10 marks
Reading File
Finding Sources
Searching the Web
CT urography technique protocol phases radiology exam 10 marks
Reading File
Reading Web Page
https://appliedradiology.com/articles/ct-urography-review-of…
I now have comprehensive information to write a well-structured 10-mark answer. Here it is:
CT Urography (CTU)
Definition
CT urography is defined by the European Society of Urogenital Radiology (ESUR) as a diagnostic examination optimized for imaging the kidneys, ureters, and bladder using thin-slice multidetector CT (MDCT), intravenous contrast medium, and image acquisition in the excretory phase. It is the modern replacement for intravenous urography (IVU).
Indications
| Category | Examples |
|---|---|
| Primary indication | Hematuria (macro/micro) - recommended by AUA & ACR as first-line imaging |
| Urolithiasis | Suspected/known renal/ureteric calculi |
| Neoplasm | Suspected renal cell carcinoma, urothelial tumors (TCC) |
| Infection | Recurrent UTI, complicated pyelonephritis, xanthogranulomatous pyelonephritis |
| Obstruction | Hydronephrosis, UPJ/UVJ obstruction |
| Trauma | Renal/ureteric injury |
| Congenital | Duplex systems, horseshoe kidney, ectopic ureter |
| Surveillance | Post-cystectomy urothelium monitoring |
Contraindications: Iodinated contrast allergy (relative), renal insufficiency (GFR concern), pregnancy.
Technique / Protocol
Patient Preparation
- Oral hydration: 2-3 glasses of water before the scan (aids ureteric distension)
- IV hydration optional
- IV furosemide (10-20 mg) at time of contrast injection - promotes diuresis and ureteric opacification
- Empty bladder prior to scan
Equipment
- Multidetector CT (MDCT) with thin slices (2.5-5 mm)
- Reconstructions: axial, coronal, sagittal; MIP reformats for the collecting system
Phases of Acquisition (Triphasic Protocol)
Phase 1: Non-contrast Phase
- Coverage: Top of kidneys to bladder base
- Purpose:
- Detect calculi (high attenuation without contrast)
- Identify fat-containing lesions (angiomyolipoma)
- Detect parenchymal calcifications
- Provide baseline attenuation for enhancement assessment
- Slice thickness: 2-2.5 mm
Phase 2: Nephrographic Phase
- Timing: 90-100 seconds after IV contrast injection (100-150 mL of non-ionic iodinated contrast at 2-4 mL/sec)
- Coverage: Abdomen and pelvis (kidneys to bladder)
- Purpose:
- Homogeneous cortex + medulla enhancement - best phase for detecting small renal masses
- Enhancement confirmed by comparison with non-contrast images (>20 HU increase = enhancement)
- Evaluation of renal vasculature
- Key feature: Most sensitive phase for renal cell carcinoma detection
Phase 3: Excretory (Pyelographic) Phase
- Timing: 12-15 minutes after contrast injection
- Coverage: Full abdomen and pelvis
- Purpose:
- Opacification and distension of renal calyces, pelvis, ureters, and bladder
- Best phase for urothelial tumors (TCC/UTUC)
- Evaluation of collecting system anatomy and filling defects
- Limitation: Ureteric peristalsis may cause non-opacification of segments
Split-Bolus Technique (Dose Reduction Alternative)
- Contrast given in two boluses before a single post-contrast acquisition
- 1st bolus (smaller, e.g., 50 mL) → 7-9 minute delay → 2nd bolus (larger, e.g., 75-100 mL) → 120 seconds → single scan
- Cumulative effect: early bolus provides excretory information; later bolus gives nephrographic information
- Advantage: Eliminates one acquisition - reduces radiation dose significantly
- Disadvantage: Less reliable ureteric opacification compared to triphasic
Techniques to Improve Ureteric Distension
The ureter is the most challenging structure to fully opacify due to peristalsis:
- IV furosemide - most effective; promotes diuresis
- IV/oral hydration - increases urine flow
- Prone positioning - uses gravity to fill dependent ureters with contrast
- Compression belt - mechanical ureteric compression at the pelvic brim
- Log-rolling - patient rolled prior to excretory acquisition to redistribute contrast
Radiation Dose
| Protocol | Effective Dose |
|---|---|
| Four-phase CTU | ~25-35 mSv |
| Excretory urography (IVU) | ~3.6 mSv |
| Split-bolus CTU | ~15-20 mSv (reduced) |
Dose reduction strategies: low-kVp technique on non-contrast phase (calculi have high intrinsic contrast), iterative reconstruction algorithms, split-bolus technique.
Findings / Diagnostic Value
| Pathology | Best Phase |
|---|---|
| Renal calculi | Non-contrast |
| Renal mass (RCC) | Nephrographic |
| Urothelial carcinoma (TCC) | Excretory/pyelographic |
| Hydronephrosis | Excretory |
| Transitional cell filling defects | Excretory |
| Ureteric pseudodiverticulosis | Excretory (associated with risk of urothelial carcinoma) |
Limitation: CTU is not accurate enough to exclude small superficial bladder tumors - cystoscopy remains mandatory for complete bladder evaluation (biopsy/resection advantage).
CT Urography vs. IVU
| Feature | CTU | IVU |
|---|---|---|
| Sensitivity for calculi | >96% | ~60% |
| Renal mass detection | Excellent | Poor |
| Urothelial TCC | Good | Limited |
| Radiation | Higher | Lower |
| Extraurinary findings | Yes | No |
| Gold standard status | Yes (upper tract) | Largely replaced |
Summary
CT urography is the gold standard for evaluation of the upper urinary tract, particularly for hematuria workup. The standard triphasic protocol (non-contrast + nephrographic + excretory) allows complete evaluation of:
- Calculi (non-contrast phase)
- Renal masses (nephrographic phase)
- Urothelial tumors and collecting system anatomy (excretory phase)
The split-bolus technique is a dose-reducing alternative. Optimization of ureteric opacification using furosemide, hydration, and prone positioning is key to a diagnostic-quality study. It cannot replace cystoscopy for bladder lesion characterization.
Isn’t there a corticomedullary phase
Yes, absolutely - you're right to flag that. The corticomedullary phase is a real and distinct phase that I omitted from the main answer. Here's the correction:
Complete Phases of CT Urography (Four-Phase Protocol)
Phase 1: Non-contrast Phase
- Timing: Before contrast
- Purpose: Calculi, fat lesions, baseline attenuation
Phase 2: Corticomedullary Phase (CMP)
- Timing: 25-40 seconds after contrast injection (arterial/early venous)
- Purpose:
- Renal cortex enhances brightly; medulla has not yet enhanced (clear corticomedullary differentiation)
- Renal arteries and veins are well opacified - ideal for vascular anatomy, renal artery stenosis, arteriovenous malformations
- Detection of hypervascular tumors (some RCCs, angiomyolipomas)
- Pre-surgical planning (donor kidneys, partial nephrectomy)
- Limitation: Small renal masses can be missed because the medulla is relatively unenhanced, creating a heterogeneous background that obscures isodense lesions
Phase 3: Nephrographic Phase
- Timing: 90-100 seconds
- Cortex + medulla enhance uniformly - best for renal mass detection
Phase 4: Excretory Phase
- Timing: 12-15 minutes
- Collecting system, ureters, bladder opacified - best for urothelial lesions
Practical Note
Not all CTU protocols include the corticomedullary phase as a routine acquisition - many standard triphasic protocols skip it to reduce radiation dose, since the nephrographic phase is superior for mass detection. The CMP is added selectively when:
- Vascular assessment is needed (renal donor evaluation, suspected vascular lesion)
- Characterization of a known hypervascular mass
- Pre-operative planning
So the full CTU can be:
- Triphasic: Non-contrast + Nephrographic + Excretory (most common)
- Four-phase: Non-contrast + Corticomedullary + Nephrographic + Excretory (higher dose, ~25-35 mSv, used when vascular detail is required)
Good catch - in an exam answer, listing all four phases with their timings and purposes would score better.
Retroperitoneal fibrosis radiology pg ans
Finding Sources
Searching the Web
retroperitoneal fibrosis radiology CT MRI findings postgraduate exam answer
Reading File
Reading File
Reading Web Page
https://radiopaedia.org/articles/retroperitoneal-fibrosis-1?…
Reading File
Loading Image
I have all the information needed. Here is a comprehensive PG-style answer:
Retroperitoneal Fibrosis - Radiology
Definition
Retroperitoneal fibrosis (RPF) / Ormond's disease is a chronic fibro-inflammatory process in which a dense fibrotic plaque forms in the retroperitoneum, typically centered over the distal aorta and iliac vessels at L4-L5, encasing and compressing the ureters, great vessels, and adjacent structures.
Imaging Modalities
1. Plain X-Ray / IVU (Intravenous Urography)
The classic investigation historically used. Key IVU findings:
- Bilateral hydronephrosis and hydroureter (bilateral in 68%, unilateral in 20%)
- Medial deviation of the mid-ureters - the most characteristic sign
- Normally ureters course laterally; in RPF they are pulled medially toward the midline
- "Maiden waist sign" - smooth, gradual tapering of the ureter at the level of obstruction (L4-L5)
- "Pipestem ureter" - long segment of ureter is narrowed and aperistaltic due to fibrotic encasement
- Site of obstruction: usually at the level of L4-L5, where the plaque is thickest
- Proximal dilation with distal narrowing - gives the classic IVU appearance
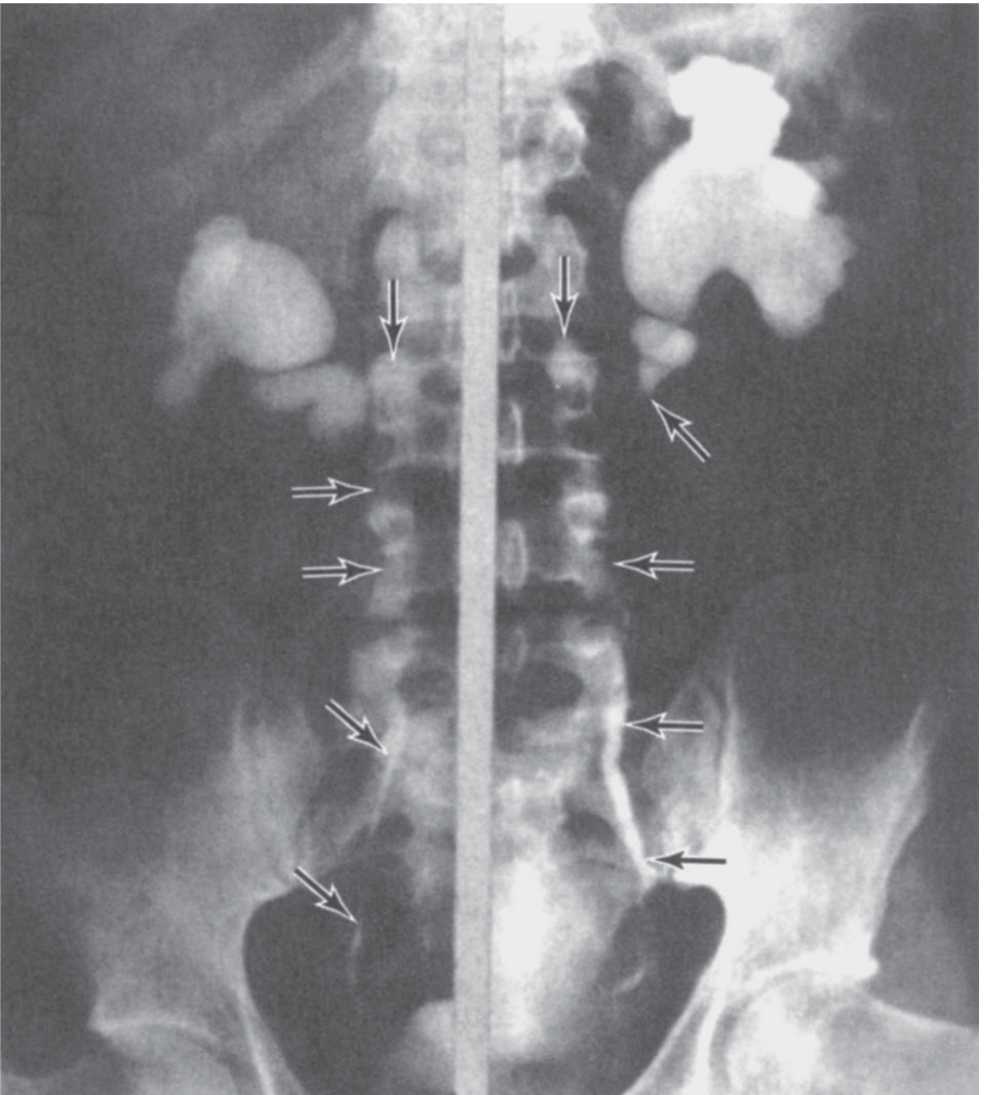
IVU showing bilateral hydronephrosis and medial deviation of both ureters with obstruction at L4-L5 level - classic RPF pattern
2. Ultrasound
- Bilateral hydronephrosis - initial finding, prompts further workup
- May show a hypoechoic periaortic soft tissue mass
- Useful for monitoring treatment response - serial assessment of hydronephrosis
- Cannot characterize the fibrotic plaque well; does not differentiate benign from malignant
- Doppler: Can detect ureteric obstruction and assess renal resistive indices
3. CT Scan (Modality of Choice for Diagnosis)
CT is the most frequently used imaging method for diagnosis and follow-up.
Key CT findings:
| Feature | Description |
|---|---|
| Location | Periaortic/periiliac soft tissue mass centered at L4-L5 |
| Density | Soft tissue attenuation (30-60 HU), homogeneous on NECT |
| Enhancement | Variable; active disease enhances post-contrast; fibrotic/inactive disease shows less enhancement |
| Shape | Plaque-like, mantle-like, encasing the aorta, IVC and ureters |
| Ureteric involvement | Bilateral medial deviation + obstruction at the level of the plaque |
| Hydronephrosis | Bilateral > unilateral |
| Aorta | Plaque hugs anterior surface of aorta - aorta not elevated from spine (key benign feature) |
| Lymph nodes | Present in ~25% of cases |
| Extent | May extend from renal hilum to iliac vessels; rarely into mediastinum |
Coronal CT reformats are pathognomonic - they best show the periaortic plaque and medial ureteric deviation simultaneously.
Contrast enhancement pattern:
- Active/inflammatory RPF: enhances on arterial and venous phase
- Inactive/fibrotic RPF: little to no enhancement
- Decreasing enhancement on serial scans = treatment response
CT-guided biopsy: CT allows percutaneous biopsy of the periaortic mass to exclude malignancy when diagnosis is uncertain.
4. MRI (Superior for Follow-Up and Tissue Characterization)
MRI is equivalent to CT for diagnosis but superior for monitoring disease activity due to higher soft-tissue contrast resolution. No ionizing radiation - preferred for serial follow-up.
Signal characteristics:
| Sequence | Signal | Significance |
|---|---|---|
| T1-weighted | Low signal intensity | Fibrotic tissue (characteristic) |
| T2-weighted | Variable | Key for activity assessment |
| T2 HIGH signal | Active, inflammatory disease (edema, cellular infiltrate) | |
| T2 LOW signal | Inactive, mature fibrosis | |
| Gadolinium (Gd) post-contrast | Enhancement in active disease | |
| Decreasing Gd enhancement | Indicates response to therapy |
Benign vs. Malignant features on MRI:
- Neither CT nor MRI reliably differentiates benign from malignant RPF
- Features suggesting malignant RPF:
- Anterior elevation of the aorta from the spine (suggests lymphoma pushing from behind)
- Lateral displacement of ureters (rather than medial)
- Localized bone destruction
- Infiltration of surrounding structures
- Irregular, lobulated margins
- Features suggesting benign RPF:
- Aorta hugging the spine (not elevated)
- Medial deviation of ureters
- Smooth, confluent plaque
5. Retrograde / Antegrade Pyelography
- Performed when CT/MRI is contraindicated (renal impairment, contrast allergy) or when endoscopic intervention is planned
- Shows:
- Long segment of ureteric narrowing at L4-L5
- Smooth tapering (not abrupt cutoff - helps distinguish from malignant stricture)
- Medial deviation of mid-ureter
- Proximal hydronephrosis
6. Nuclear Medicine / PET-CT
- FDG-PET/CT: Most sensitive imaging study for disease activity
- Active RPF shows increased FDG uptake in the fibrotic plaque
- Can differentiate active from inactive disease better than CT/MRI alone
- Distinguishes RPF from malignant mimics (metastatic lymphoma, etc.)
- May obviate the need for biopsy in typical cases
- Useful for monitoring treatment response
- MAG3/DTPA renography (differential scintigraphy): Assesses individual renal function - important for surgical planning (ureterolysis)
Differential Diagnosis on Imaging
| Condition | Distinguishing Feature |
|---|---|
| Lymphoma | Aorta elevated anteriorly, lateral ureteric displacement, discrete nodes |
| Metastatic disease | Prior malignancy history, bone destruction, irregular mass |
| Aortic aneurysm | Dilated aortic lumen, wall calcification, pulsatile mass |
| Amyloidosis | Diffuse retroperitoneal infiltration, other organ involvement |
| Desmoplastic reaction (post-RT/surgery) | Clinical history, localized to field |
Summary of Modality Use
| Modality | Role |
|---|---|
| IVU | Historic; shows medial ureteric deviation and hydronephrosis |
| Ultrasound | Initial screening; serial monitoring of hydronephrosis |
| CT | Gold standard for diagnosis; characterizes plaque, guides biopsy |
| MRI | Superior for disease activity and treatment monitoring (T2 signal) |
| Retrograde pyelogram | When CT/MRI contraindicated; pre-intervention planning |
| PET-CT | Most sensitive for activity; differentiates benign/malignant; monitors therapy |
Classic exam pointer: The combination of bilateral hydronephrosis + medial deviation of mid-ureters at L4-L5 + periaortic soft tissue plaque that hugs the anterior spine without elevating the aorta = pathognomonic for benign RPF on imaging.
This is a shared conversation. Sign in to Orris to start your own chat.