Lipa in Tb
Reading File
Finding Sources
Finding Sources
Searching PubMed
lipid tuberculosis Mycobacterium
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I have enough information to give a thorough answer. Here is a comprehensive breakdown:
Lipoarabinomannan (LAM) in Tuberculosis
What is LAM?
Lipoarabinomannan (LAM) is a major lipid polysaccharide complex found in the cell wall of Mycobacterium tuberculosis (MTb). It is a key virulence factor and diagnostic target. LAM is structurally and functionally analogous to the lipopolysaccharide (LPS) of Gram-negative bacteria.
1. Structure and Location in the Cell Wall
The mycobacterial cell wall is exceptionally lipid-rich (>60% of total cell wall mass), which explains many of MTb's unique biological characteristics. LAM:
- Extends from the plasma membrane to the cell surface
- Works alongside mycolic acids (long-chain fatty acids) to form a waxy, hydrophobic coat
- Is embedded within a peptidoglycan backbone
This waxy coat makes MTb:
- Hardy and resistant to desiccation
- Impenetrable to many antibiotics
- Resistant to decolorization after staining (the basis of acid-fastness)
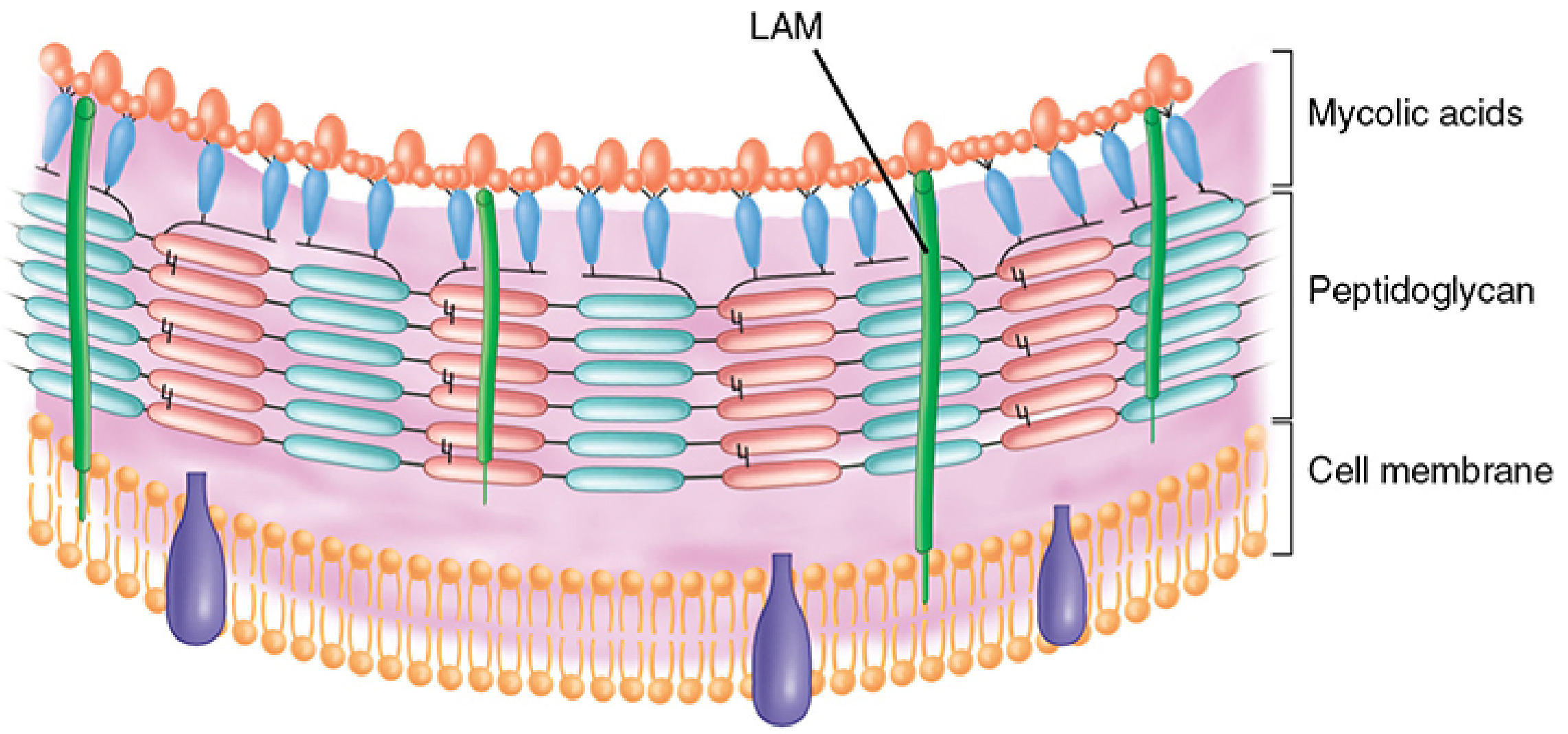
FIGURE: Mycobacterial cell wall structure. LAM (green) spans from the cell membrane to the outer mycolic acid layer. (Sherris & Ryan's Medical Microbiology, 8th ed.)
2. Role in Pathogenesis
LAM contributes to immune evasion:
- Blocks phagosome-lysosome fusion: MTb uses LAM to interfere with the killing mechanisms of alveolar macrophages after ingestion, allowing it to survive intracellularly
- Suppresses macrophage activation: Interferes with IFN-γ signaling, reducing oxidative burst and cytokine production
- Inhibits autophagy: The host's autophagy pathway (a key antimycobacterial defense) is suppressed partly through LAM-mediated mechanisms
- When macrophage activation is incomplete, progressive disease (tuberculosis) results; when Th1 responses (IFN-γ mediated macrophage activation) succeed, most infections are contained
3. Diagnostic Role: The LF-LAM Test
Because LAM is shed from metabolically active or damaged mycobacterial cells, it appears in urine - making it a non-sputum diagnostic target.
| Feature | Detail |
|---|---|
| Test name | Lateral Flow Urine Lipoarabinomannan Assay (LF-LAM; Alere Determine TB LAM Ag) |
| Sample | Urine (easy to collect, no transmission risk) |
| WHO endorsement | Endorsed in 2015 as a point-of-care TB diagnostic |
| Best performance | HIV-positive patients with CD4 count ≤100 cells/µL or severely ill |
| Detects | LAM antigen shed from cell walls of active or dead/damaged MTb |
| Limitation | Low sensitivity in HIV-negative patients; not available in the USA |
"The lateral flow lipoarabinomannan assay (LF-LAM; Alere Determine TB LAM Ag test) detects antigen shed from mycobacterial cell walls from either metabolically active or damaged cells... sensitivity is better among patients with a low CD4 count and higher disease burden." - Tietz Textbook of Laboratory Medicine, 7th ed.
"Lipoarabinomannan, a glycolipid of the M. tuberculosis cell wall, can be detected in the urine of patients with pulmonary or extrapulmonary TB and advanced HIV, but this test is not available in the United States." - Goldman-Cecil Medicine
4. Role in Acid-Fastness
LAM and mycolic acids together are directly responsible for the acid-fast staining property of mycobacteria:
- Staining requires extreme measures (heat, prolonged exposure, penetrating agents)
- Once stained with carbol fuchsin, the dye cannot be washed out by acid-alcohol decolorization
- This property is the basis for the Ziehl-Neelsen (ZN) stain and fluorochrome (auramine-rhodamine) stain used in sputum microscopy for TB diagnosis
Key Summary
| Aspect | Role of LAM |
|---|---|
| Cell wall structure | Lipid-polysaccharide spanning plasma membrane to outer surface |
| Virulence | Blocks phagolysosome fusion, suppresses macrophage activation |
| Acid-fastness | Contributes to waxy coat responsible for the property |
| Diagnosis | Target of urine LF-LAM assay (especially in HIV+, low CD4) |
| Analogy | Functional analog of Gram-negative LPS |
Sources: Sherris & Ryan's Medical Microbiology, 8th ed. | Goldman-Cecil Medicine | Tietz Textbook of Laboratory Medicine, 7th ed. | Murray & Nadel's Textbook of Respiratory Medicine
Lipa test in mtb
Finding Sources
Finding Sources
Searching PubMed
line probe assay tuberculosis drug resistance
Reading File
Reading File
Reading File
Reading File
I now have everything needed for a complete, detailed answer.
LiPA (Line Probe Assay) in MTB
What is LiPA?
The LiPA (Line Probe Assay / LPA) is a family of DNA strip-based molecular tests used to:
- Identify Mycobacterium tuberculosis complex (MTBC)
- Rapidly detect drug resistance-associated mutations - directly from sputum or from cultures
LiPA is the gold standard rapid tool for MDR-TB screening and is WHO-recommended worldwide.
Principle - How Does It Work?
The test follows a reverse hybridization approach:
- DNA extraction - from clinical specimen (smear-positive sputum) or cultured isolate
- PCR amplification - resistance gene regions are amplified and labeled
- Hybridization - labeled PCR products bind to specific oligonucleotide probes immobilized on a nitrocellulose strip
- Detection - colorimetric development; a band/line appears on the strip when a known resistance mutation is present
- Interpretation - the pattern of bands present vs. absent reveals the resistance profile
"Line probe assays determine the drug resistance profile of a strain by the pattern of binding of amplified DNA to probes on the strip. When one of the known mutation resistance genes is amplified in the TB strain, a line or band appears on the strip." - Murray & Nadel's Textbook of Respiratory Medicine
Commercially Available LiPA Tests
| Assay | Manufacturer | Resistance Detected | Notes |
|---|---|---|---|
| INNO-LiPA Rif.TB | Fujirubio | Rifampicin (rpoB) only | Research use only |
| GenoType MTBDRplus | Hain Lifescience | Rifampicin (rpoB) + Isoniazid (katG, inhA) | Most widely used; WHO-endorsed 2008, updated 2016 |
| GenoType MTBDRsl v2.0 | Hain Lifescience | Fluoroquinolones (gyrA, gyrB), 2nd-line injectables (rrs, eis), Ethambutol (embB) | For XDR-TB screening |
| Genoscholar NTM+MDRTB II | Nipro | Rifampicin + Isoniazid | Also identifies NTM species |
Gene Targets
| Drug | Gene Target | Mutation Type |
|---|---|---|
| Rifampicin | rpoB | Mutations in RRDR (rifampicin resistance-determining region) |
| Isoniazid (high-level) | katG (Ser315Thr) | Most common INH resistance mutation |
| Isoniazid (low-level) | inhA promoter | Low-level resistance, cross-resistance to ethionamide |
| Fluoroquinolones | gyrA, gyrB | QRDR mutations |
| Kanamycin/Amikacin | rrs | 16S rRNA mutations |
| Capreomycin | rrs, eis | |
| Ethambutol | embB |
Accuracy - Sensitivity & Specificity
From the Murray & Nadel accuracy table (eTable 53.1):
| Assay | Drug | Direct Sensitivity* | Direct Specificity* |
|---|---|---|---|
| GenoType MTBDRplus | Rifampicin | 98.2% | 97.8% |
| GenoType MTBDRplus | Isoniazid | 96.4% | 98.8% |
| Genoscholar NTM+MDRTB II | Rifampicin | 96.5% | 97.5% |
| Genoscholar NTM+MDRTB II | Isoniazid | 94.9% | 97.6% |
| MTBDRsl v2.0 | Fluoroquinolones | 86% | 98.5% |
| MTBDRsl v2.0 | 2nd-line injectables | 87.3% | 99.5% |
Direct = testing on smear-positive sputum specimens; Indirect = testing on culture isolates
Specimen Requirements
- Direct testing: Smear-positive sputum samples (AFB smear positive)
- Indirect testing: Positive mycobacterial culture isolates
- NOT suitable for smear-negative sputum directly (lower sensitivity)
- Requires biosafety level 3 (BSL-3) laboratory infrastructure, separate rooms for DNA extraction, pre- and post-amplification to avoid contamination
WHO Recommendations
- First-line LPA (MTBDRplus / Genoscholar): Recommended as the initial test for rapid detection of rifampicin and isoniazid resistance in patients with smear-positive specimens or cultured isolates
- Second-line LPA (MTBDRsl): Recommended as the initial test for rapid detection of fluoroquinolone and injectable resistance in confirmed MDR-TB or RR-TB cases
- Pyrazinamide resistance: WHO now recommends reverse hybridization-based LPA on culture isolates
- LPAs do not replace conventional phenotypic DST - they are rapid screening tools; phenotypic culture-based DST is still needed to detect resistance to other drugs and monitor for emerging resistance
LiPA vs. Other Rapid Molecular Tests
| Feature | LiPA (GenoType MTBDRplus) | Xpert MTB/RIF | WGS |
|---|---|---|---|
| TB identification | Yes | Yes | Yes |
| Rifampicin resistance | Yes | Yes | Yes |
| Isoniazid resistance | Yes | No | Yes |
| 2nd-line drug resistance | Yes (MTBDRsl) | No | Yes |
| Turnaround time | Same day (from positive culture) | ~2 hours | Days-weeks |
| Smear-negative sputum | No | Yes | No (needs culture) |
| FDA-cleared (USA) | No | Yes | N/A |
| WHO-endorsed | Yes | Yes | Yes (tNGS) |
| Biosafety requirement | BSL-3 | BSL-2 | BSL-3 |
Key Clinical Importance
- MDR-TB screening: LiPA is the primary rapid tool to diagnose MDR-TB (rifampicin + isoniazid resistant) before culture results are available
- XDR-TB screening: MTBDRsl identifies pre-XDR/XDR-TB by detecting fluoroquinolone and injectable resistance
- Treatment guidance: Rapid results allow clinicians to immediately tailor TB treatment regimens, rather than waiting 8+ weeks for phenotypic DST on solid media
- Not a replacement for phenotypic DST - LiPA only detects known mutations; novel/rare resistance mechanisms may be missed
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025) | Murray & Nadel's Textbook of Respiratory Medicine | Tietz Textbook of Laboratory Medicine, 7th ed.
Significance
Finding Sources
Finding Sources
Searching PubMed
line probe assay MDR-TB clinical significance outcomes
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the material needed for a thorough answer on the significance of LiPA in MTB.
Significance of the LiPA (Line Probe Assay) in MTB
1. Rapid MDR-TB Diagnosis - The Core Significance
The single most important significance of LiPA is speed. Conventional culture-based drug susceptibility testing (DST) takes:
- Liquid media: ~3 weeks
- Solid media: up to 8 weeks or more
LiPA delivers results on the same day the specimen is received (from a smear-positive sputum or positive culture). This has profound clinical consequences:
"The genotypic methods are faster than culture-based tests... integrated with the M. tuberculosis identification methods." - Murray & Nadel's Textbook of Respiratory Medicine
Without LiPA, a patient with MDR-TB could receive standard first-line therapy (rifampicin + isoniazid) for weeks to months before resistance is discovered - causing treatment failure, worsening disease, and onward transmission of drug-resistant strains.
2. Simultaneous TB Identification AND Resistance Detection
LiPA performs two tasks in one test:
- Confirms the presence of M. tuberculosis complex
- Simultaneously identifies resistance mutations to first-line drugs (rifampicin, isoniazid) and second-line drugs (fluoroquinolones, aminoglycosides)
This means a single strip test can tell the clinician: "This is TB - and it is MDR" - replacing what would previously require weeks of parallel workup.
3. Enables Appropriate Treatment Selection Immediately
| Without LiPA | With LiPA |
|---|---|
| Start RHZE empirically | Start tailored regimen based on resistance profile |
| Wait 8 weeks for DST | Same-day guidance |
| Risk of amplifying resistance (inadequate therapy) | Appropriate combination from Day 1 |
| Ongoing transmission of MDR strains | Prompt isolation and correct treatment |
Rifampicin resistance detected by LiPA is a surrogate marker for MDR-TB - resistance to rifampicin alone is rare, and its presence almost always predicts co-resistance to isoniazid. Detection of rpoB mutations by LiPA thus flags MDR-TB with high reliability:
"Resistance to rifampin has been used as an indicator for multidrug-resistant TB." - Murray & Nadel's Textbook of Respiratory Medicine
"Mutations in the rpoB rifampin resistance-determining region are present in 96% of rifampin-resistant strains." - Murray & Nadel's
4. Detecting Specific Resistance Mutations Has Treatment Implications
LiPA identifies which mutation is responsible - not just whether resistance exists. This matters because:
- katG Ser315Thr (high-level INH resistance) - requires replacing isoniazid entirely
- inhA promoter mutation (low-level INH resistance) - also predicts ethionamide cross-resistance, affecting second-line regimen choices
- gyrA mutations - confirms fluoroquinolone resistance, critical for XDR-TB regimen planning
- rrs/eis mutations - guides use of amikacin, kanamycin, capreomycin in MDR-TB regimens
Without mutation-level detail, these nuanced treatment decisions would be impossible without weeks of phenotypic testing.
5. WHO-Recommended for Global TB Control
LiPA is central to the WHO strategy for tackling the MDR-TB epidemic:
- First-line LPA (MTBDRplus): WHO-endorsed since 2008, updated 2016 - recommended for all patients with smear-positive sputum or cultured isolates to detect rifampicin + isoniazid resistance
- Second-line LPA (MTBDRsl): WHO-recommended for rapid detection of fluoroquinolone and injectable resistance in confirmed MDR-TB/RR-TB cases
- LPA for pyrazinamide: WHO now recommends reverse hybridization LPA on culture isolates for PZA resistance
- Most widely studied and used at reference laboratories in low- and middle-income countries - exactly where the TB burden is greatest and phenotypic DST capacity is weakest
"The WHO recommends that [LPAs] are used to detect resistance to isoniazid and rifampin when patients have sputum smear-positive specimens or a cultured isolate of M. tuberculosis." - Harrison's Principles of Internal Medicine, 22nd ed. (2025)
6. Significance in Specific Patient Populations
| Population | Why LiPA Matters |
|---|---|
| High-risk for MDR-TB (prior TB treatment failure, contact of MDR case) | Immediate identification prevents wasted first-line therapy |
| HIV co-infected | Rapid diagnosis prevents fatal delays in immunocompromised patients |
| Resource-limited settings | Provides same-day DST where conventional culture is not available |
| Smear-positive cases | Direct testing on sputum bypasses the need to wait for culture |
7. Limitations - Why Significance Is Not Absolute
| Limitation | Implication |
|---|---|
| Only detects known mutations | Novel/rare resistance variants are missed (LiPA can be false-susceptible) |
| Not FDA-cleared in the USA | Cannot be used as a standalone clinical test in the US |
| Requires BSL-3 lab | Not a point-of-care test; needs infrastructure |
| Smear-negative sputum | Cannot be used directly; culture needed first |
| Does not replace phenotypic DST | Culture-based DST still required for complete resistance profiling and monitoring |
| Sensitivity for katG/inhA (~65-75%) | Misses ~25-35% of isoniazid-resistant strains not caused by these common mutations |
Summary: Why LiPA Is Significant
| Significance | Impact |
|---|---|
| Speed | Same-day vs. 8-week wait for DST |
| Dual function | Identifies MTB + resistance simultaneously |
| MDR-TB surrogate | rpoB mutation = MDR-TB flag |
| Mutation-specific | Guides precise treatment (katG vs inhA, gyrA vs rrs) |
| XDR-TB detection | MTBDRsl identifies second-line resistance |
| Global TB control | WHO-endorsed for high-burden, resource-limited settings |
| Prevents treatment failure | Avoids months of ineffective therapy |
| Infection control | Rapid ID allows timely isolation of MDR cases |
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025) | Murray & Nadel's Textbook of Respiratory Medicine | Tietz Textbook of Laboratory Medicine, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.