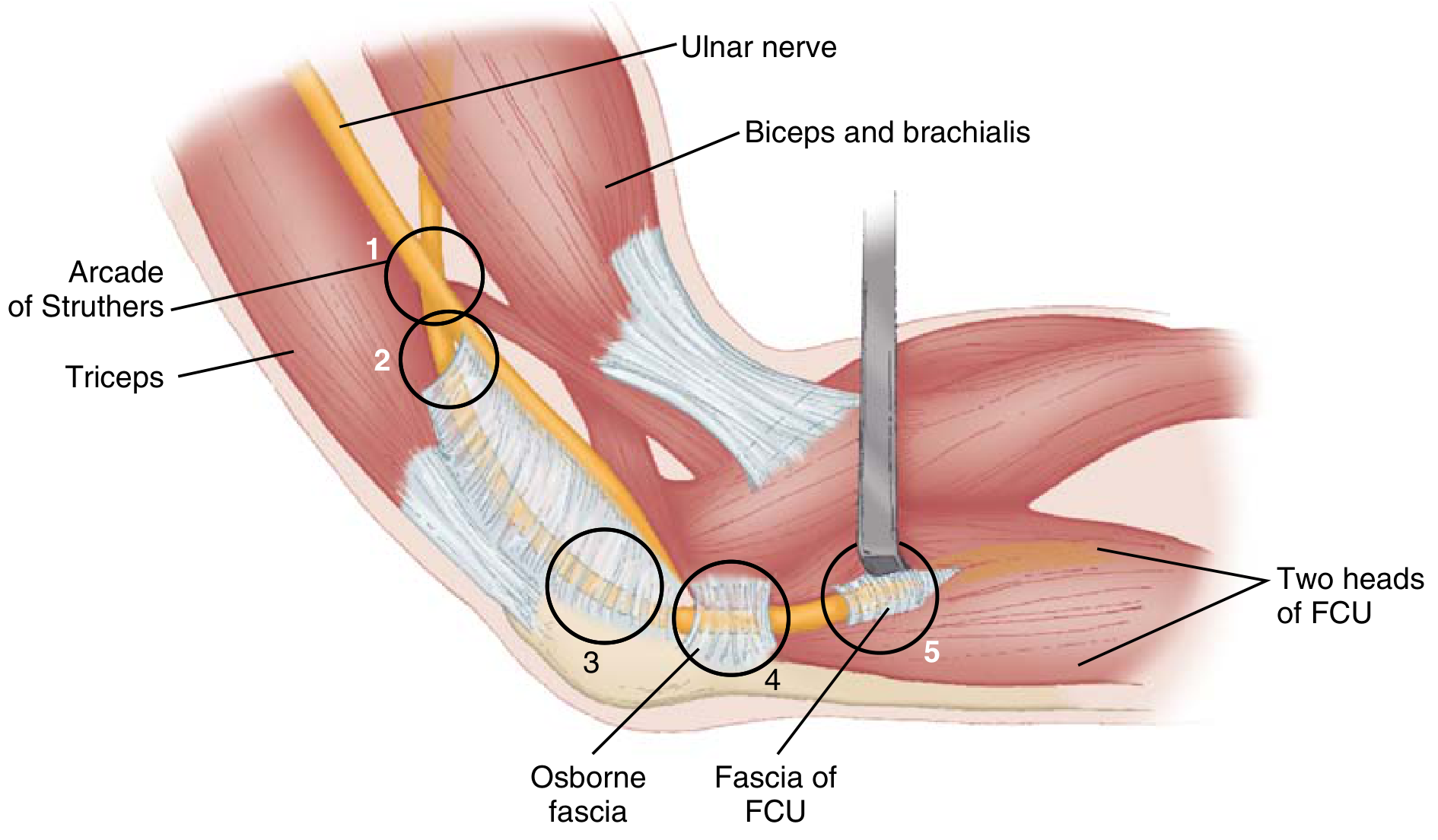
Sites of compression of ulnar nerve from proximal to distal
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from multiple authoritative surgical and neurology textbooks. Here is the complete answer:
Sites of Compression of the Ulnar Nerve (Proximal to Distal)
The ulnar nerve (C8, T1 - medial cord of brachial plexus) has multiple potential compression sites along its course. A useful mnemonic from Miller's Review of Orthopaedics is AO TEAM for elbow-level sites.
IN THE ARM
1. Arcade of Struthers
- A fascial thickening at the hiatus of the medial intermuscular septum, located approximately 8 cm proximal to the medial epicondyle, where the ulnar nerve passes from the anterior to the posterior compartment of the arm.
- This is the most proximal significant compression site.
2. Medial Intermuscular Septum
- As the nerve pierces this septum to travel posterior to the medial head of triceps, the sharp edge of the septum itself can compress the nerve.
3. Medial Head of Triceps
- The nerve runs alongside the medial head of triceps and can be compressed here, particularly with anatomical variations or hypertrophy.
AT THE ELBOW (Cubital Tunnel Region)
4. Medial Epicondyle / Ulnar Groove (Sulcus Ulnaris Syndrome)
- The nerve lies in the groove between the medial epicondyle and the olecranon in a superficial, exposed position.
- Compression occurs from direct external pressure (e.g., leaning on elbow), fracture/dislocation, osteophytes, or the nerve subluxing forward over the medial epicondyle during elbow flexion ("snapping ulnar nerve").
- Tardy ulnar palsy: chronic compression years after a previous elbow injury causing cubitus valgus.
5. Osborne's Ligament (Arcuate Ligament)
- A fibrous band (also called the humeral-ulnar aponeurosis) that forms the roof of the cubital tunnel, running from the medial epicondyle to the olecranon.
- Thickening or fibrosis of this structure is the most common cause of cubital tunnel syndrome.
6. Anconeus Epitrochlearis
- An anomalous muscle (variant present in some individuals) originating from the medial olecranon and inserting on the medial epicondyle; it can compress the nerve at the cubital tunnel roof.
7. Fascia/Aponeurosis of Flexor Carpi Ulnaris (FCU) - Two Heads
- Just distal to the cubital tunnel, the nerve passes under the tendinous arch between the two heads (humeral and ulnar) of the FCU.
- This is cubital tunnel syndrome proper and is a very common compression site.
- Fascial bands within the FCU muscle belly can also constrict the nerve.
IN THE FOREARM
8. Deep Flexor-Pronator Aponeurosis
- Fascial bands between the FCU and FDP can compress the nerve as it runs in the forearm. (Less common.)
AT THE WRIST / HAND (Guyon's Canal - Ulnar Tunnel)
The Guyon (ulnar) canal is bounded by: volar carpal ligament (roof), TCL (floor), hook of hamate (radial wall), pisiform and ADM muscle belly (ulnar wall).
The canal is divided into three zones, each producing a distinct clinical picture:
| Zone | Location | Clinical Deficit |
|---|---|---|
| Zone I | Proximal to bifurcation of ulnar nerve | Mixed motor + sensory |
| Zone II | Around deep motor branch | Pure motor (interossei, hypothenars) - no sensory loss |
| Zone III | Distal sensory branches | Pure sensory |
Common causes at the wrist:
- Ganglion cyst (80% of nontraumatic cases)
- Hook of hamate fracture/nonunion
- Ulnar artery thrombosis
- Lipoma, palmaris brevis hypertrophy, anomalous muscle
- Chronic repetitive pressure (bicycle handlebars, canes, tools)
- Rheumatoid arthritis, degenerative changes
IN THE PALM (Most Distal)
9. Deep Branch in the Palm
- The deep branch of the ulnar nerve, after exiting the Guyon canal, can be compressed by chronic pressure from hand tools (e.g., air hammers, screwdrivers) - "hypothenar hammer syndrome".
- Produces a pure motor deficit (claw hand) with no sensory disturbance because the superficial branch is intact.
Summary Table
| Level | Structure | Syndrome |
|---|---|---|
| Arm, ~8 cm above medial epicondyle | Arcade of Struthers | Arcade of Struthers compression |
| Arm | Medial intermuscular septum | - |
| Arm | Medial head of triceps | - |
| Elbow | Medial epicondyle/ulnar groove | Sulcus ulnaris syndrome, tardy ulnar palsy |
| Elbow | Osborne's (arcuate) ligament | Cubital tunnel syndrome |
| Elbow | Anconeus epitrochlearis (variant) | Cubital tunnel syndrome |
| Forearm (proximal) | FCU two-head aponeurosis/arch | Cubital tunnel syndrome |
| Wrist | Guyon's canal (Zone I/II/III) | Ulnar tunnel syndrome |
| Palm | Deep branch in palm | Hypothenar hammer / pure motor palsy |
Key clinical correlations:
- Elbow compression: claw hand + dorsal ulnar hand sensory loss (dorsal cutaneous branch intact, exits above wrist)
- Wrist/Guyon canal compression: claw hand + palmar sensory loss (dorsal cutaneous branch spared, exits in distal forearm)
- Deep palmar branch compression: pure motor claw hand, no sensory loss at all
Sources: Miller's Review of Orthopaedics 9th Ed., Table 7.8 (Fig. 7.53); Bradley and Daroff's Neurology in Clinical Practice; Bailey & Love's Surgery 28th Ed.; THIEME Atlas of Anatomy
Provide the original paper in which chiene’s parallelogram of hip was first mentioned
Searching the Web
Chiene's parallelogram hip original paper publication John Chiene
Searching PubMed
Chiene parallelogram hip
Searching the Web
John Chiene surgeon Edinburgh "parallelogram" hip 1870s original publication
Searching the Web
Chiene "Complete System of Surgery" OR "Edinburgh Medical Journal" parallelogram hip trochanter
Reading Web Page
https://en.wikipedia.org/wiki/John_Chiene
Searching the Web
Chiene 1870 "parallelogram" hip dislocation fracture neck femur Edinburgh "greater trochanter" ASIS original
I need to be transparent with you here.
The original paper by John Chiene in which the parallelogram of the hip was first described cannot be reliably identified from available sources.
Here is what I was able to confirm:
- John Chiene (1843-1923) was a Scottish surgeon and Professor of Surgery at the University of Edinburgh (1882-1909), who trained under James Syme and worked as an anatomy demonstrator under John Goodsir.
- He is known for Chiene's lines (used in cerebral localisation for neurosurgical procedures) as well as the parallelogram of the hip.
- He published several surgical works and papers, primarily in Edinburgh-based journals of the late 19th century.
- The Edinburgh Medical Journal from this era references his anatomical work, but no specific paper describing the parallelogram of the hip is indexed in PubMed or readily accessible in digitised archives.
What is likely: Given the era and his career trajectory, the description of the parallelogram almost certainly appeared in one of the following:
- The Edinburgh Medical Journal (1870s-1880s)
- His own surgical textbook or anatomical manual published in the late 19th century
- Possibly as part of his anatomy demonstrating work under Goodsir in the 1860s
The honest answer is that this is a 19th-century eponymous clinical sign whose original primary source is not digitally indexed and is not traceable through PubMed, Google Scholar, or readily accessible archives. Most modern orthopaedic and surgical textbooks that cite it do not provide a primary reference, simply attributing it to "Chiene."
To find the original paper, you would need to search:
- The physical archives of the Edinburgh Medical Journal (circa 1865-1890)
- The Royal College of Surgeons of Edinburgh library
- The Wellcome Collection or British Library holdings of 19th-century Scottish surgical literature
If you have access to any of these institutional archives, that would be the most productive avenue.
This is a shared conversation. Sign in to Orris to start your own chat.