teach me ct scan brain with pathologic findings with real pics
CT brain pathology findings hyperdense hypodense examples radiology education
https://radiologykey.com/imaging-the-head-and-brain
CT brain scan pathology real images epidural subdural subarachnoid hemorrhage infarct tumor radiology teaching
CT Brain: A Complete Teaching Guide with Pathologic Findings
Before You Read a CT Brain - The Basics
How CT Works for the Brain
| Tissue | HU | Appearance |
|---|---|---|
| Air | -1000 to -600 | Black |
| Fat | -100 to -60 | Very dark |
| Water / CSF | 0-18 | Dark gray |
| White matter | 30-34 | Medium gray |
| Gray matter | 37-41 | Slightly brighter gray |
| Fresh blood (clotted) | 50-100 | White/bright |
| Bone | 600-2000 | Bright white |
- Neuroanatomy through Clinical Cases, 3rd Edition, Table 4.1
The "Blood Can Be Very Bad" Mnemonic
- B - Blood
- C - Cisterns
- B - Brain parenchyma
- V - Ventricles
- B - Bone
Normal CT Anatomy (Quick Reference)
- Gray matter (cortex, basal ganglia, thalamus): slightly hyperdense relative to white matter
- White matter: hypodense gray
- CSF (ventricles, sulci, cisterns): dark
- Falx cerebri: bright midline structure (dura)
- Skull: bright white
- The two cerebral hemispheres should be symmetric
PATHOLOGIC FINDINGS
1. Subdural Hematoma (SDH)
CT Appearance by Age:
| Stage | Time | CT Appearance |
|---|---|---|
| Acute | 0-7 days | Hyperdense (bright white), crescent-shaped |
| Subacute | 1-3 weeks | Isodense (same as brain - easy to miss!) |
| Chronic | >3 weeks | Hypodense (dark, like CSF) |
| Mixed density | Rebleed | Hyperdense + hypodense layers (hematocrit effect) |
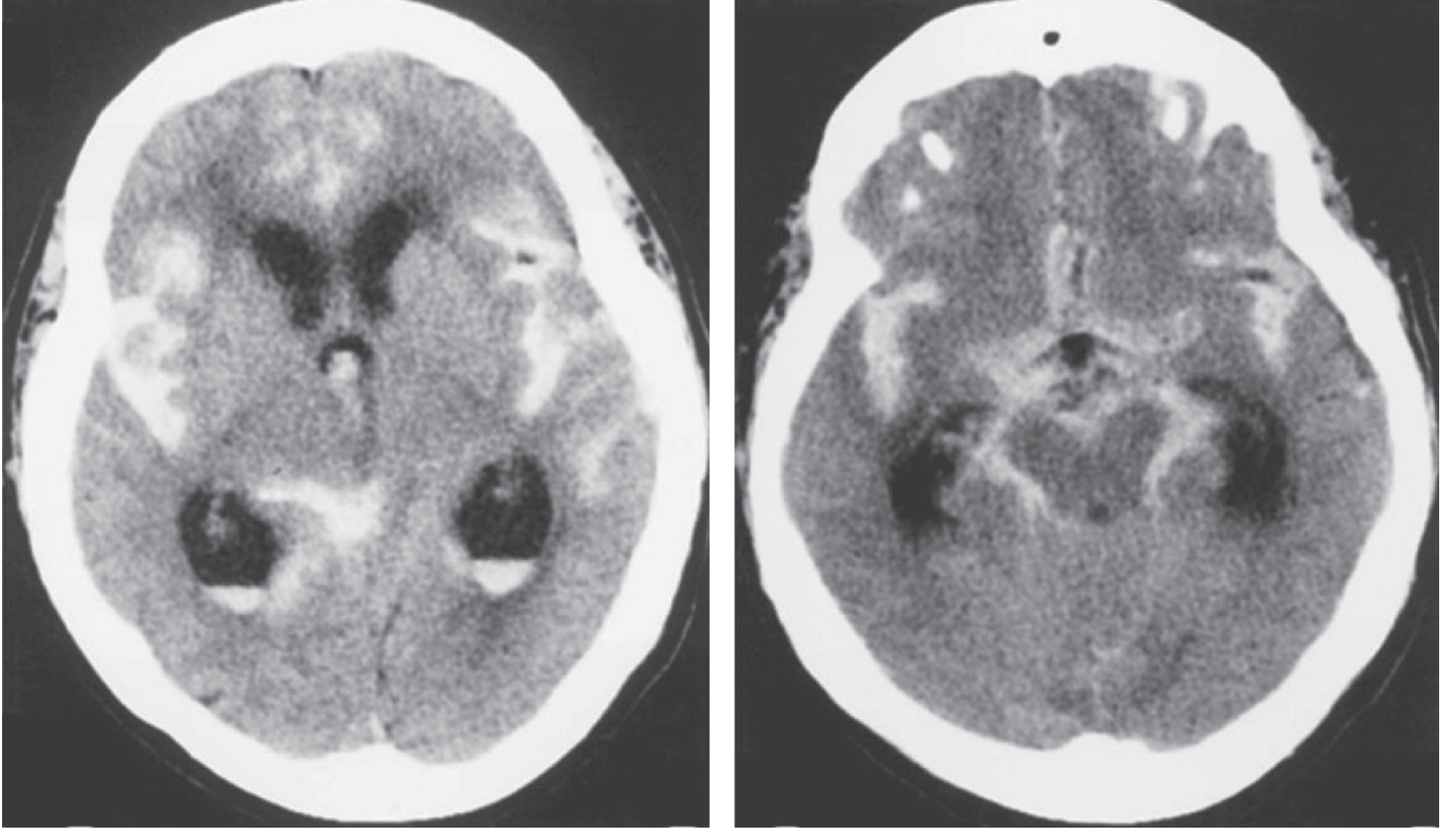
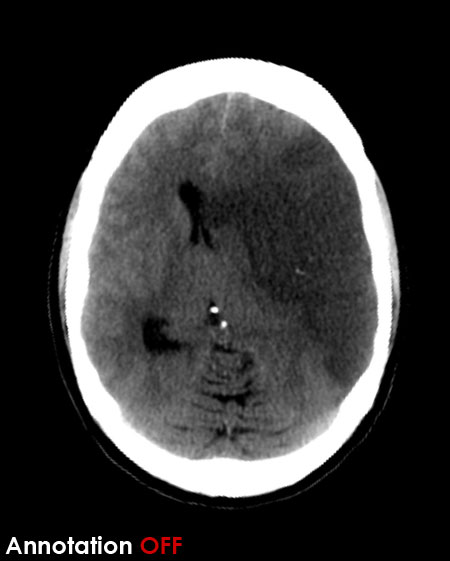
The key CT clues for bilateral isodense SDH: sulci are absent ("supraphysiologic brain"), brain looks too full.
Real CT Images from Textbooks:
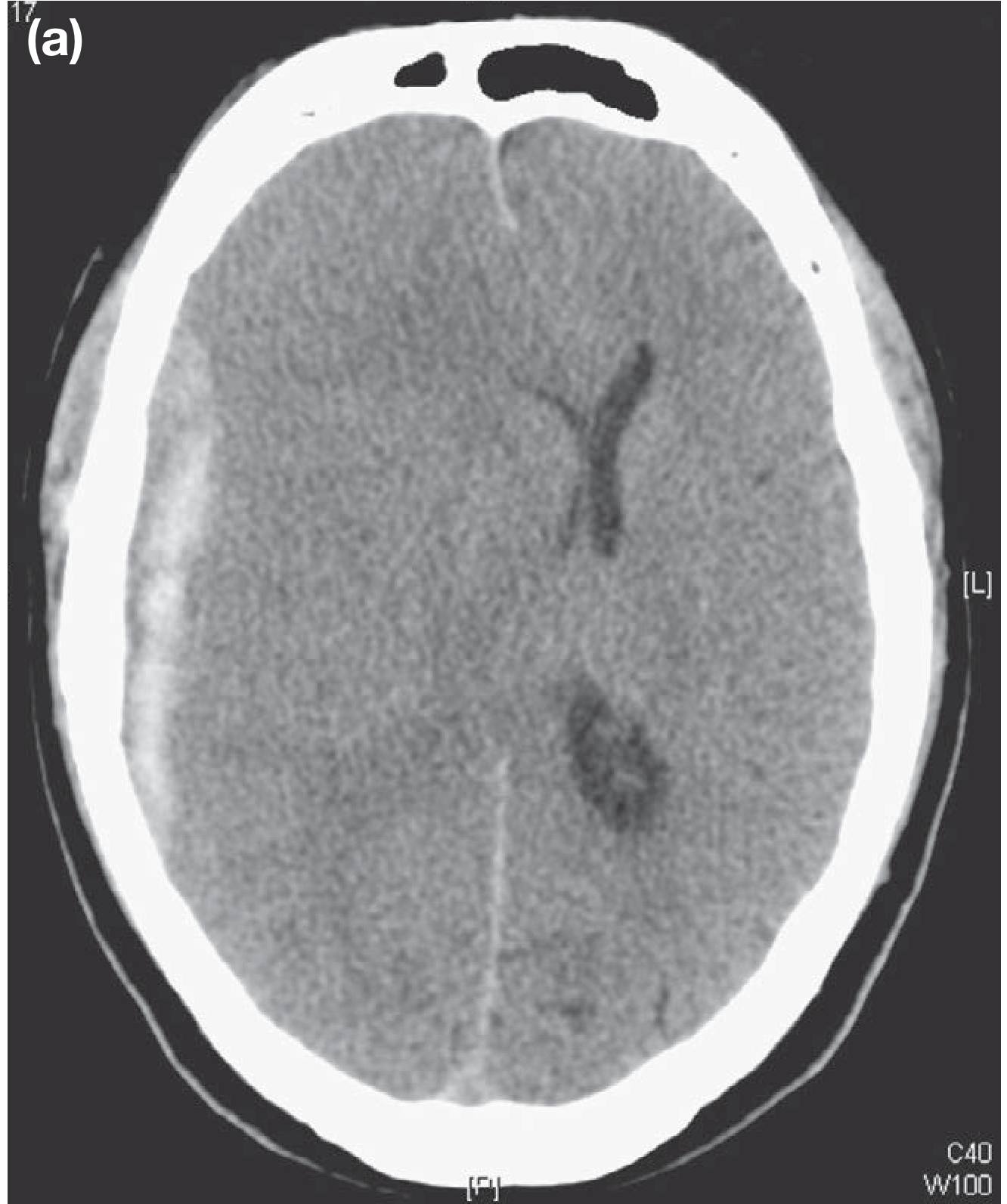
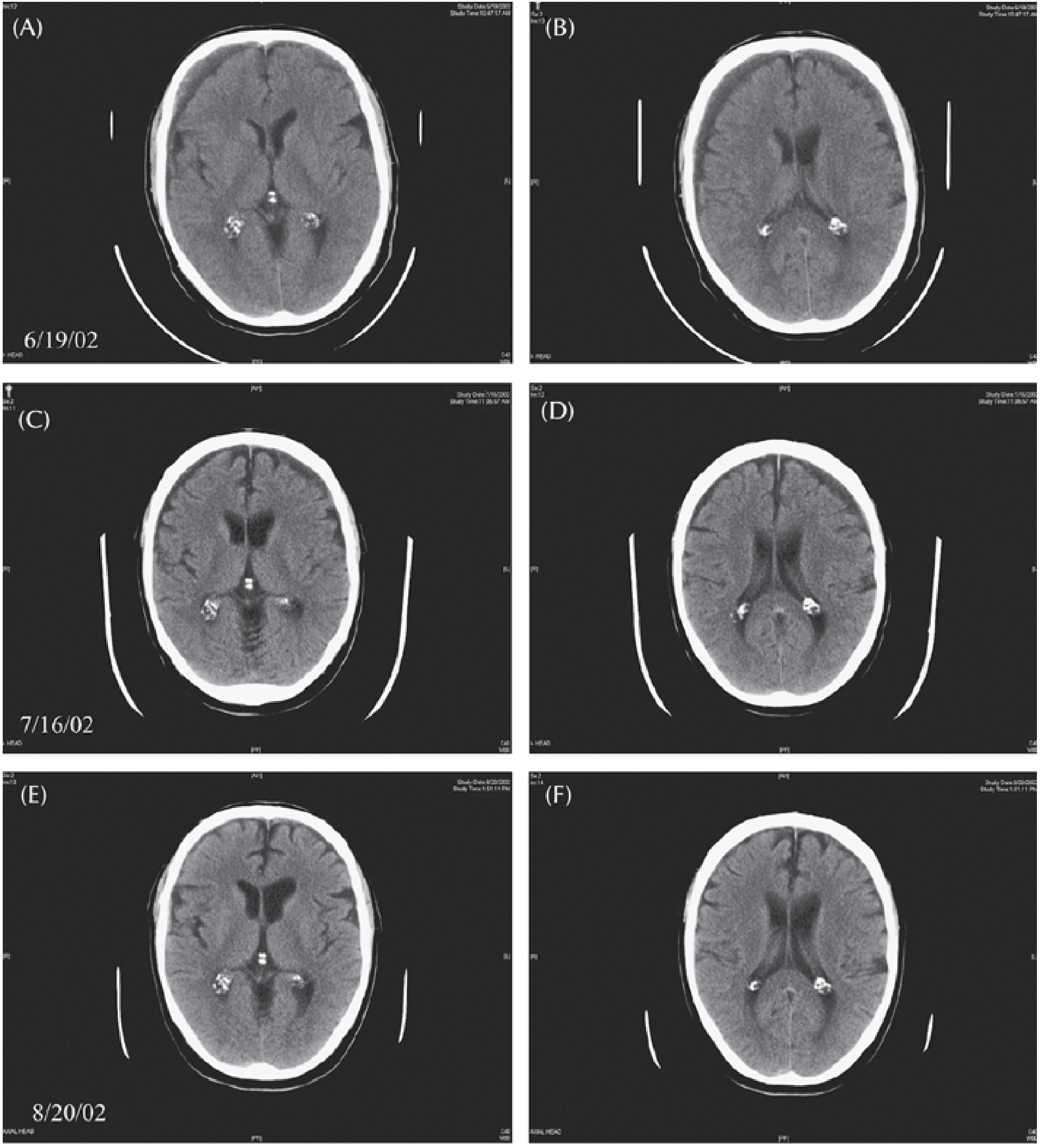
- Acute SDH - urgent craniotomy/craniectomy
- Chronic SDH in elderly/anticoagulated - may manage with burr holes once liquefied
- Bilateral isodense SDH is a diagnostic trap
- Plum & Posner, p. 252-253
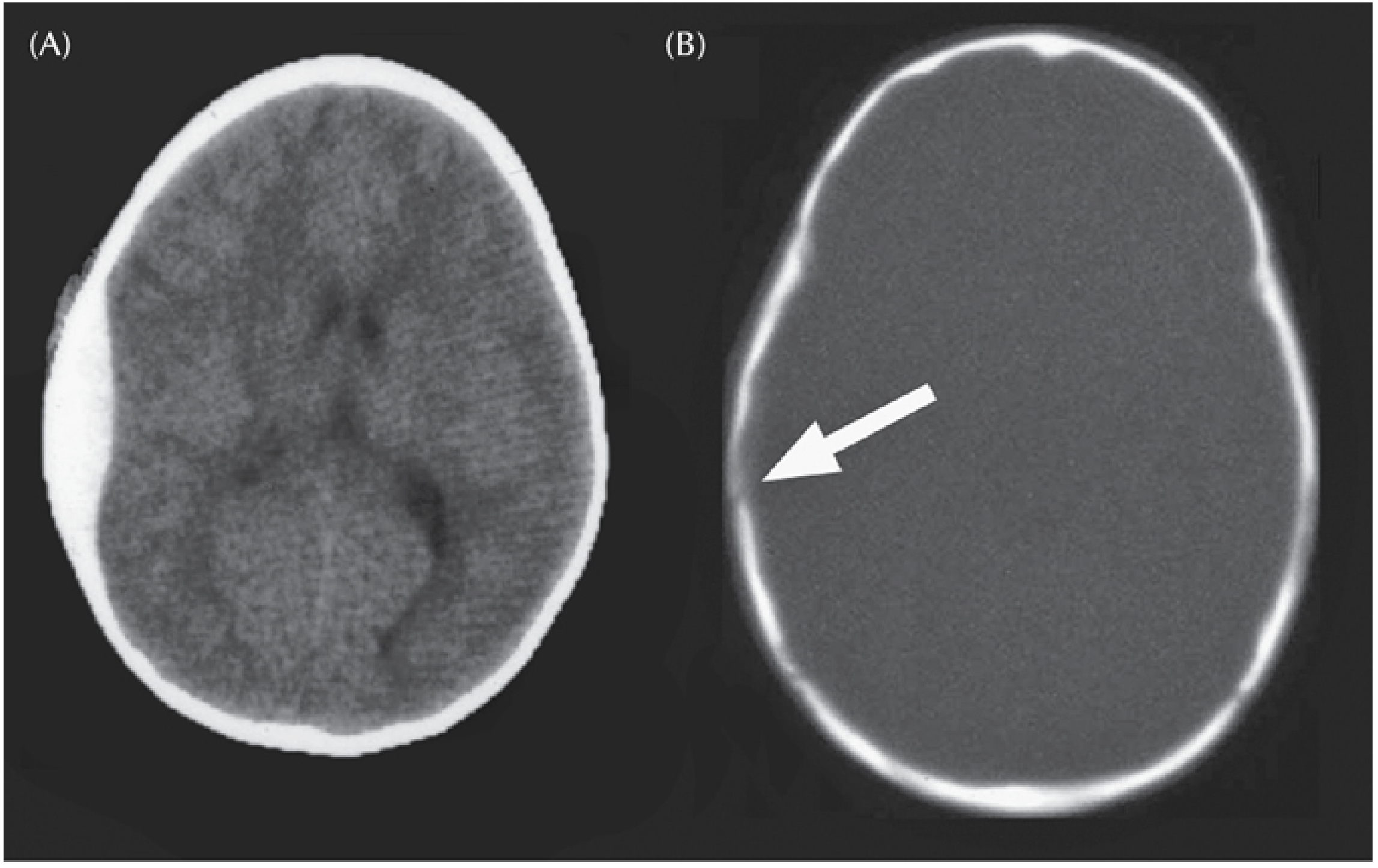
2. Epidural Hematoma (EDH)
CT Appearance:
- Biconvex (lens-shaped) hyperdense collection
- Does NOT cross suture lines (unlike SDH)
- Often associated with overlying skull fracture
- Classic clinical: lucid interval then rapid deterioration
- EDH = Biconvex, limited by sutures, arterial (rapid expansion)
- SDH = Concave/crescent, crosses sutures, venous (slower)
Emergency: Once large enough, EDH causes transtentorial herniation and death. Patients need emergent surgical evacuation.
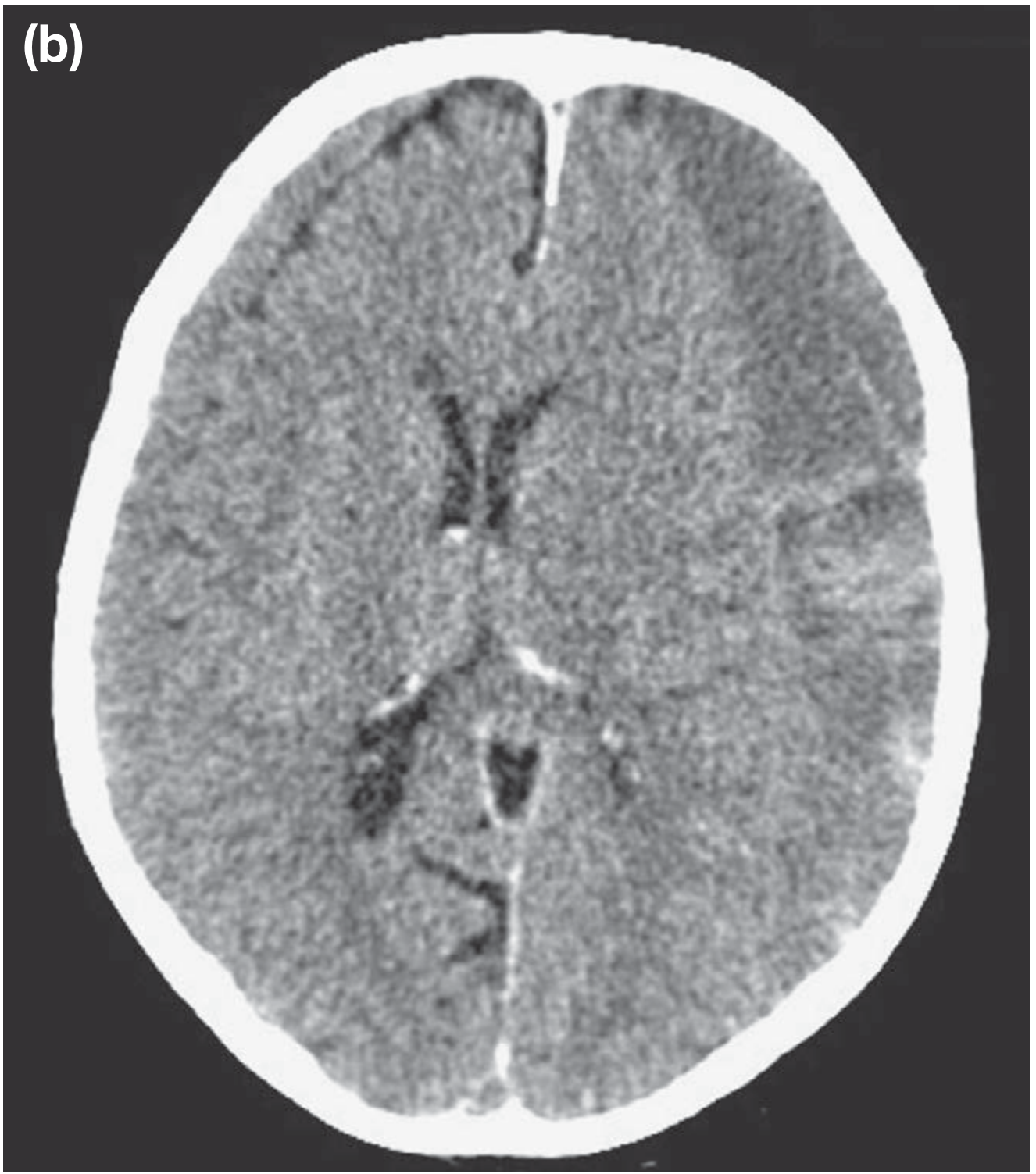
3. Subarachnoid Hemorrhage (SAH)
CT Appearance:
- Hyperdense blood filling the sulci and cisterns - blood "tracks" into sulci (unlike SDH where sulci are effaced but blood-free)
- Basal cisterns (suprasellar, sylvian, ambient) - look for bright white filling
- Intraventricular extension possible (blood in ventricles)
- CT sensitivity: ~98% within 6 hours of onset; drops to ~90% at 24h, ~70% at 1 week
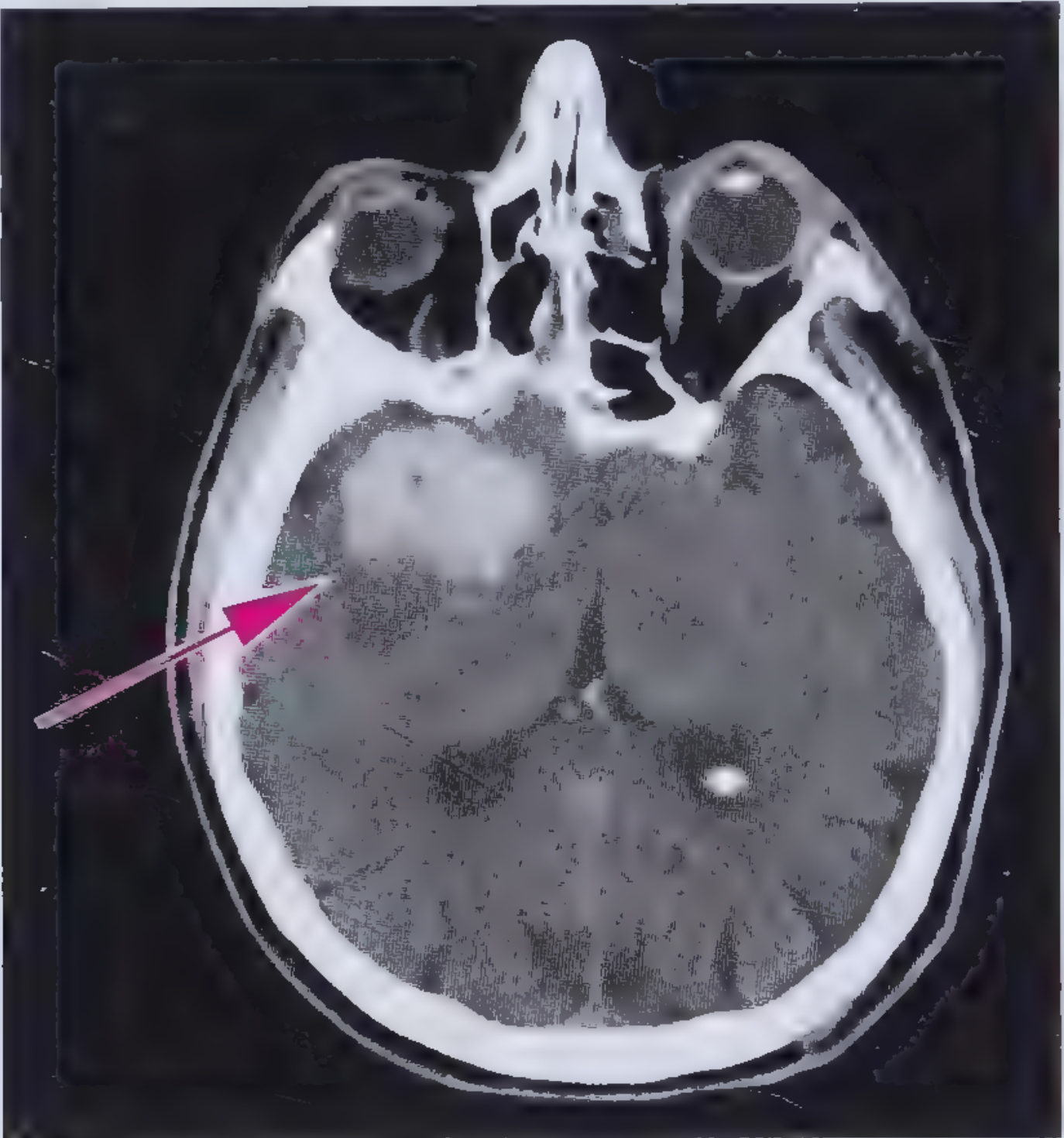
4. Intracerebral Hemorrhage (ICH)
CT Appearance:
- Well-defined hyperdense homogeneous area within brain tissue
- Hyperdense for ~7 days, then progressively loses density
- Clears periphery first; center remains hyperdense
- At 4 weeks: completely hypodense, no mass effect
- Surrounding hypodense ring = edema
Hypertensive ICH Favorite Locations:
- Putamen / Basal ganglia (most common)
- Thalamus
- Pons
- Cerebellum
- Lobar (think amyloid angiopathy in elderly)
ICH is distinguished from ischemic stroke by being hyperdense on non-contrast CT. Ischemic stroke is hypodense.
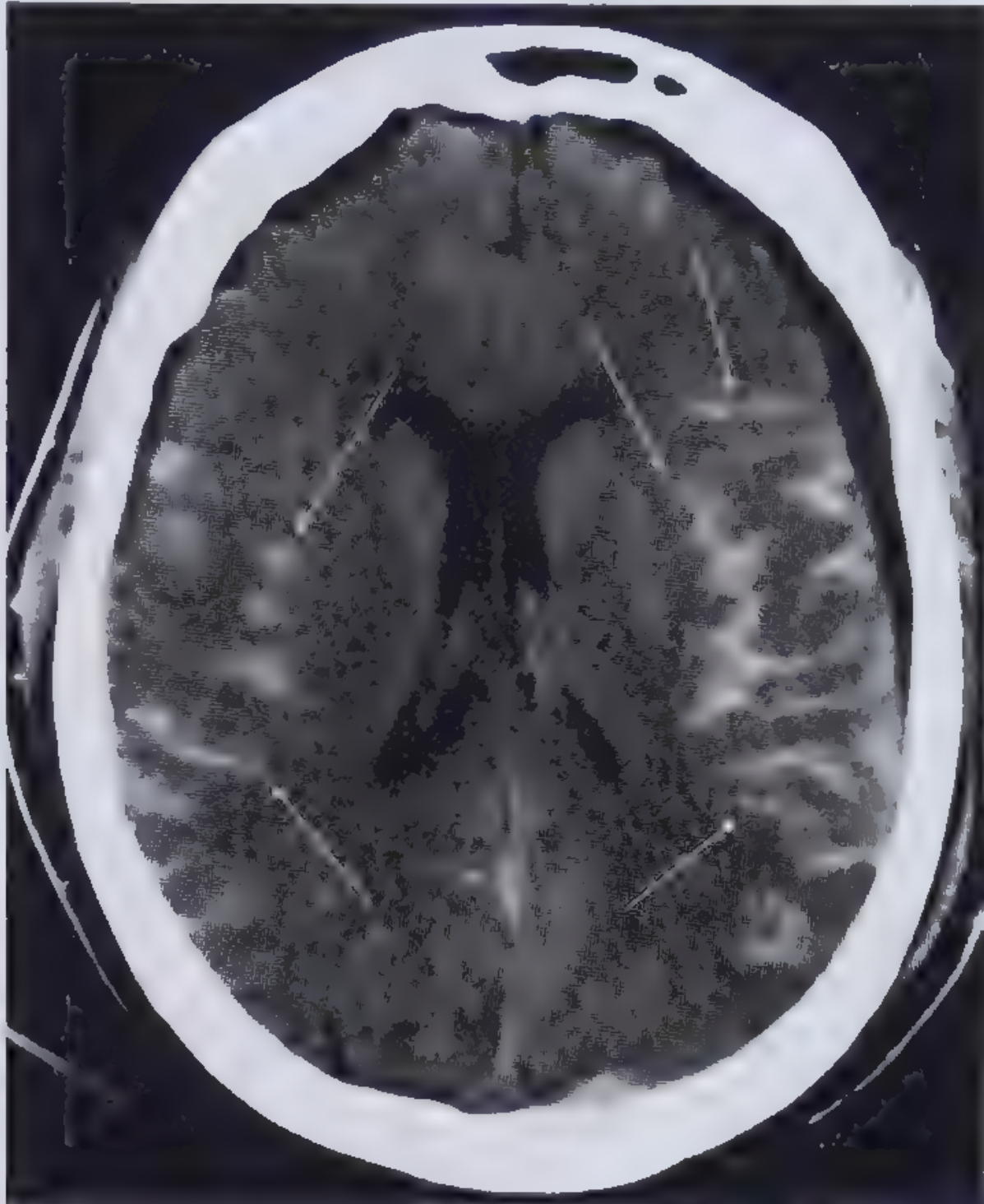
5. Ischemic Stroke / Cerebral Infarction
CT Evolution of Ischemic Stroke:
| Time | CT Finding |
|---|---|
| 0-6 hours | Normal OR subtle early signs |
| 6-24 hours | Hypodensity in vascular territory; loss of gray-white differentiation |
| 24h-3 days | Hypodense wedge-shaped area, max swelling by day 3 |
| 7-21 days | Progressive hypodensity, may show hemorrhagic transformation (gyral hyperdensity) |
| >21 days (chronic) | Gliosis, volume loss, sulcal widening adjacent to infarct |
Early CT Signs of Ischemic Stroke (within 6 hours):
- The thrombosed MCA appears as a bright white line/dot on non-contrast CT
- Seen in hyperacute MCA territory stroke
- Guides treatment decisions (e.g., thrombectomy eligibility)
- Earliest sign of CVA on CT
- Infarct edema makes gray matter hypodense, equalizing with white matter
- Look at insular cortex: Insular Ribbon Sign - loss of the normal density difference at the insula
- Edematous cortex swells and obliterates nearby sulci
- Lenticulostriate territory may show early hypodensity
A normal head CT in the first 3 hours of stroke symptoms does NOT exclude ischemic stroke. The most important role in that window is to exclude hemorrhage before giving thrombolytics (tPA/TNK).
6. Brain Tumor
- May appear hypodense (low-grade glioma, edema), hyperdense (meningioma, lymphoma, metastases with hemorrhage), or isodense
- May contain calcification (bright white foci), necrosis (dark center), cysts (fluid density), or hemorrhage
- Surrounding vasogenic edema = finger-like hypodense projections through white matter (follows white matter tracts)
- Ring enhancement on contrast CT = irregular hyperdense ring around necrotic core (GBM, abscess, mets)
- Mass effect: sulcal effacement, ventricular compression, midline shift
- Round/irregular shape (not confined to vascular territory) suggests tumor
- Waxing/waning symptoms over days-weeks (not sudden onset) = tumor
- Sparing of cortex (tumor may stay subcortical initially) vs. infarct (involves both cortex + white matter)
- MRI contrast is definitive
7. Brain Abscess
- Appears as hypodense lesion on non-contrast CT
- May contain air within (pathognomonic if present)
- Ring enhancement on contrast CT (smooth, thin ring - thinner than GBM ring)
- Differential: metastasis, toxoplasmosis, neurocysticercosis (all can ring-enhance)
- Clinical context essential: immunosuppression, fever, dental/sinus source
8. Hydrocephalus
- Enlarged ventricles (temporal horns >2mm = early sign)
- Transependymal edema in acute obstruction: periventricular hypodensity around ventricles (CSF seeping through)
- Sulci may be effaced (communicating) or normal/small (obstructive)
9. Diffuse Axonal Injury (DAI)
- High-velocity rotational injury (MVA, shaken baby)
- CT has LOW sensitivity for DAI - may appear normal or near-normal despite severe injury
- When visible: multiple tiny hemorrhagic foci at gray-white matter junction, corpus callosum, brainstem
- MRI (especially gradient echo/SWI) is far superior for detecting DAI
Key Teaching Points Summary
| Finding | Density | Shape | Key Feature |
|---|---|---|---|
| Acute SDH | Hyperdense | Crescent | Crosses sutures |
| EDH | Hyperdense | Biconvex | Stops at sutures, lucid interval |
| SAH | Hyperdense | In cisterns/sulci | Fills CSF spaces |
| ICH | Hyperdense | Round/ovoid, in parenchyma | Hypertensive locations |
| Acute infarct (>6h) | Hypodense | Wedge, vascular territory | Loss of gray-white diff. |
| Tumor | Variable | Round/irregular, any location | Ring enhancement, vasogenic edema |
| Abscess | Hypodense core | Round | Smooth ring enhancement |
| Hydrocephalus | Dark | Enlarged ventricles | Temporal horn > 2mm |
CT Windows to Use
- Brain window (W: 80, L: 40): Standard for brain parenchyma and blood
- Bone window (W: 2000, L: 600): Skull fractures
- Subdural window (W: 130, L: 30): Better detection of isodense/small SDH
- Stroke window (W: 40, L: 40): Enhances early ischemic hypodensity
ct brain normal with landmarks and pointing each structure ct brain film real time make it easy to learn
normal CT brain axial anatomy labeled landmarks real scan teaching radiology
CT brain axial levels labeled anatomy posterior fossa pons cerebellum basal ganglia ventricles cortex e-anatomy imaios
site:imaios.com CT brain axial labeled anatomy cerebellum pons midbrain cisterns
🧠 Normal CT Brain - Complete Anatomy Guide with Real Labeled Images
How to Orient Yourself on a CT Head
- Right side of image = Patient's LEFT side
- Left side of image = Patient's RIGHT side
- Slices go bottom to top (inferior to superior)
- More slices = thinner detail (standard: 5mm per slice)
LEVEL 1 - Skull Base / Cranial Base
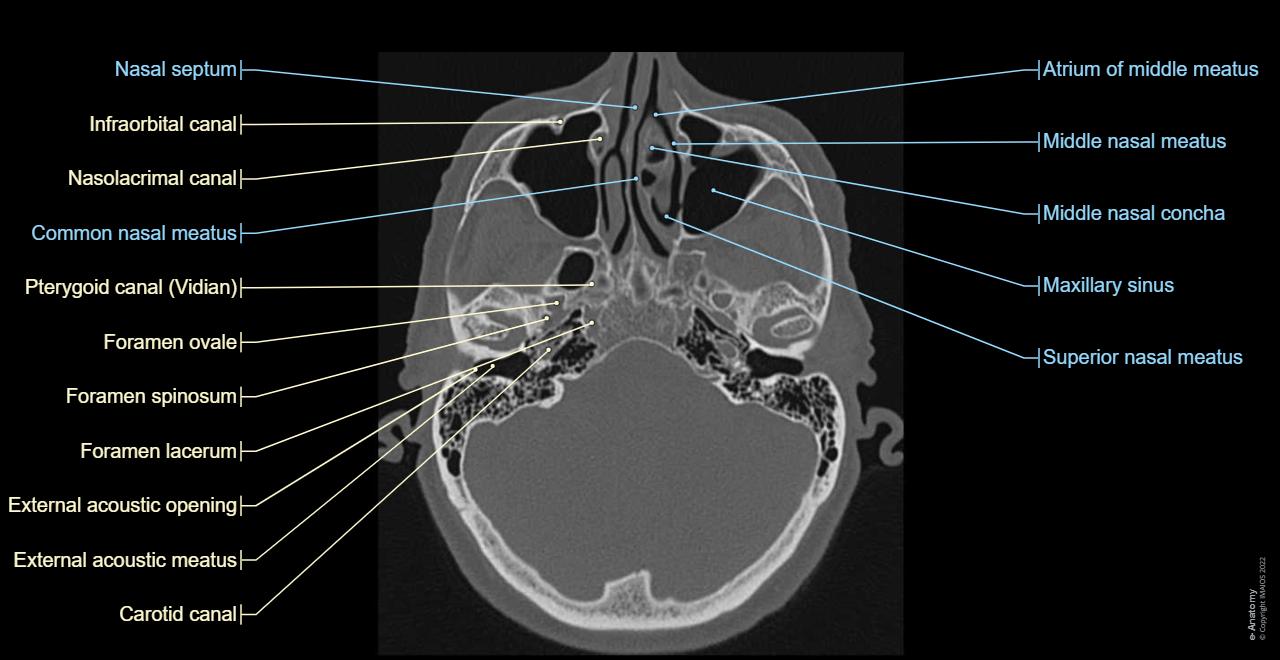
| Structure | What It Is | Clinical Relevance |
|---|---|---|
| Foramen ovale | Opening in sphenoid bone | Transmits CN V3 (mandibular nerve) |
| Foramen spinosum | Hole in sphenoid | Middle meningeal artery passes through - rupture = epidural hematoma |
| Foramen lacerum | Irregular opening at skull base | Internal carotid passes through |
| Carotid canal | Channel for ICA | ICA dissection visible here on CT-A |
| External acoustic meatus | Ear canal | Fractures here can cause hemotympanum |
| Maxillary sinus | Air-filled paranasal sinus | Dark (air-density); opacification = sinusitis/fracture |
| Nasal septum | Bony midline partition | Deviation, fractures |
Tip: Use bone window settings at this level. Brain window will not show these fine bony details.
LEVEL 2 - Posterior Fossa: Cerebellum & Pons
| Structure | Appearance | Notes |
|---|---|---|
| Pons | Gray, butterfly-shaped, anterior | Contains CN VI, VII, VIII nuclei |
| Cerebellum | Two hemispheres + vermis (midline) | Coordinates movement; look for midline symmetry |
| Fourth ventricle | Dark midline CSF space between pons and cerebellum | Obstructed = hydrocephalus |
| Cerebellopontine (CP) angle | CSF space at junction of cerebellum + pons | Site of acoustic neuromas (CN VIII tumors) |
| Basilar artery | Small bright dot anterior to pons | May appear hyperdense if thrombosed |
| Mastoid air cells | Honeycomb black (air) behind ear | Opacification = mastoiditis |
| Temporal lobes | Gray matter lateral to pons |
Tip: The posterior fossa has lots of streak artifact from dense surrounding bone (petrous bone). This is NOT pathology.
LEVEL 3 - Suprasellar / Basal Cisterns Level
| Structure | What to Look For |
|---|---|
| Suprasellar cistern | Star-shaped CSF space - should be DARK. If white = subarachnoid blood! |
| Sylvian fissures | Dark CSF-filled grooves lateral to midbrain - if white = SAH |
| Interpeduncular cistern | CSF between cerebral peduncles |
| Midbrain | Central gray structure at this level |
| Temporal horns | Thin slit lateral ventricle horns - if >2mm = early hydrocephalus |
The "5 cisterns" rule: Suprasellar, sylvian (×2), ambient (×2) = all should appear dark (CSF). Filling with blood = subarachnoid hemorrhage.
LEVEL 4 - Basal Ganglia Level (The Most Important Level!)
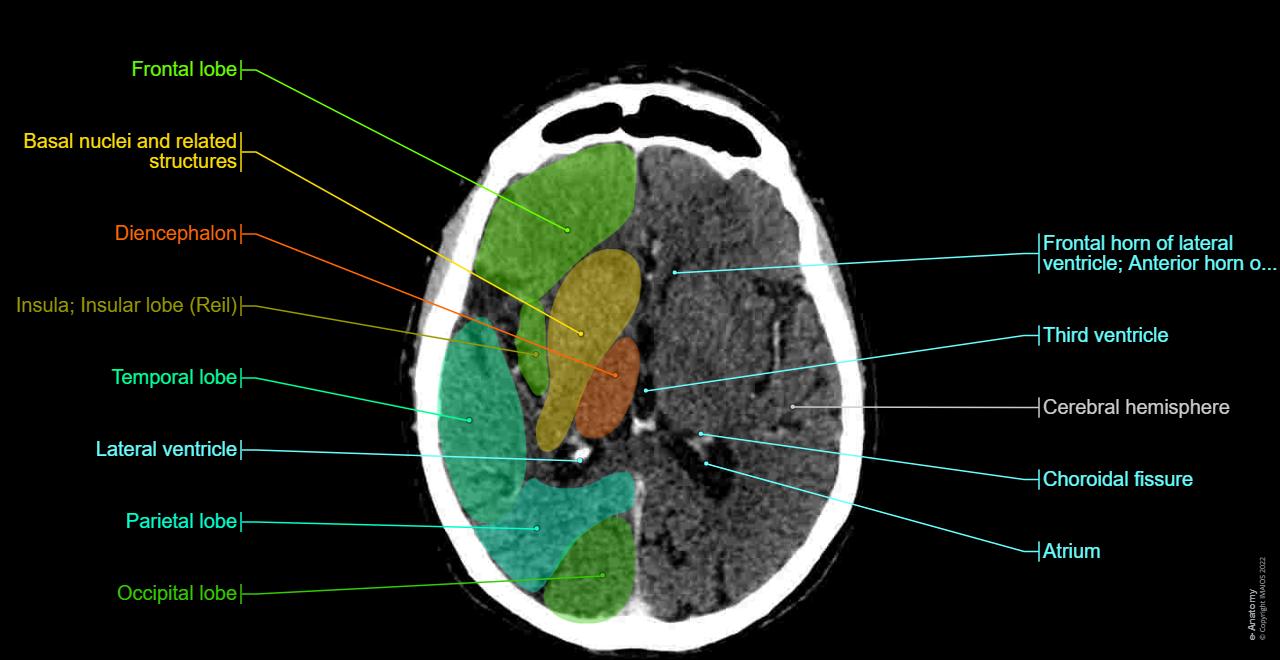
| Structure | Appearance | Clinical Notes |
|---|---|---|
| Frontal lobe | Anterior gray-white brain | |
| Temporal lobe | Lateral brain, at sides | |
| Parietal lobe | Posterior-lateral | |
| Occipital lobe | Posterior | |
| Insula (insular lobe) | Buried cortex, lateral | Insular ribbon sign - loss = early MCA stroke |
| Frontal horn of lateral ventricle | Dark CSF, anterior | Should be symmetric |
| Third ventricle | Thin dark midline slit | Widened = hydrocephalus |
| Lateral ventricle (atrium) | Posterior dark CSF space | |
| Choroidal fissure | CSF cleft near hippocampus | |
| Basal nuclei (ganglia) | Deep gray structures, slightly brighter than white matter | Hypertensive bleed favorite spot |
| Diencephalon (thalamus) | Paired gray masses on either side of 3rd ventricle |
From outside → in (lateral to medial):
Insular cortex
↓
Extreme capsule (thin white matter)
↓
Claustrum
↓
External capsule
↓
PUTAMEN (lateral basal ganglia - most common hypertensive bleed site)
↓
INTERNAL CAPSULE (posterior limb = motor/sensory tracts)
↓
GLOBUS PALLIDUS (medial to putamen)
↓
THALAMUS (next to 3rd ventricle)
↓
Third ventricle (midline CSF)
↓
CAUDATE HEAD (anterolateral wall of lateral ventricle)
Memory tip - "Hypertensive bleeds like to happen at the 4 Ps": Putamen, Pons, cerebellar Peduncle, Parieto-occipital (lobar - amyloid).
LEVEL 5 - Ventricular / Corpus Callosum Level
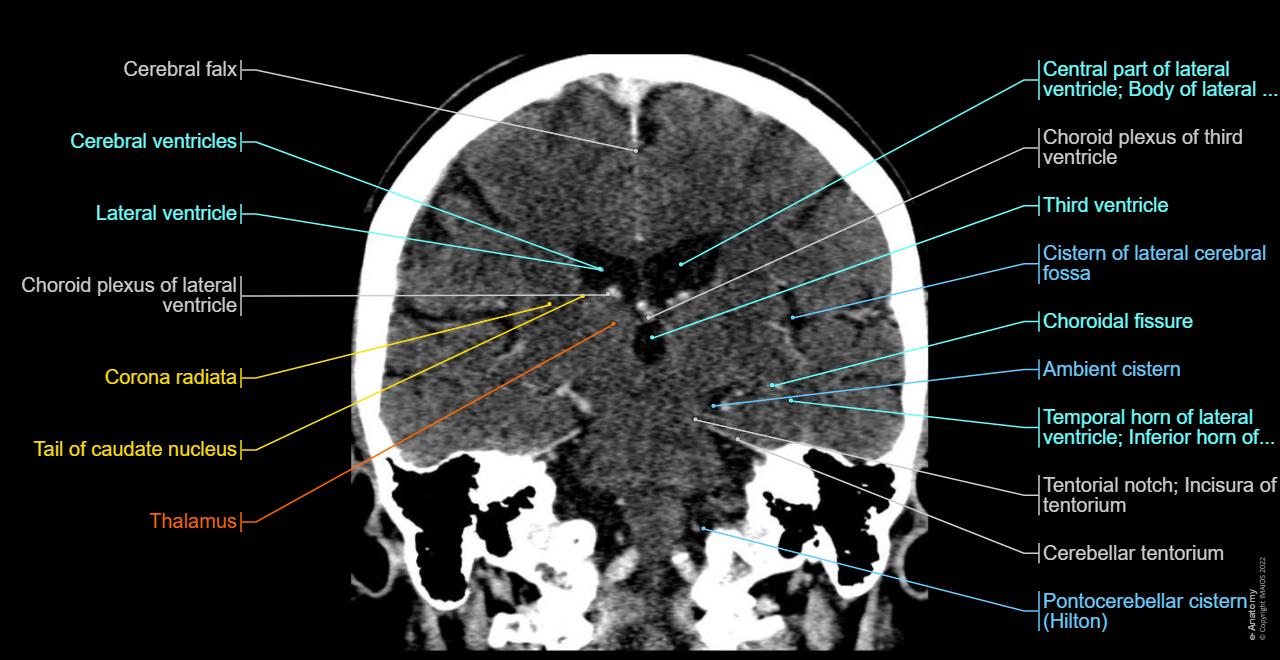
| Structure | Notes |
|---|---|
| Falx cerebri | Bright white midline dural fold - normally midline |
| Lateral ventricles (body) | Large dark CSF spaces |
| Third ventricle | Midline slit between thalami |
| Thalamus | Oval gray structures flanking 3rd ventricle |
| Temporal horn of lateral ventricle | Inferior horn - dilated = hydrocephalus or temporal lobe atrophy |
| Corona radiata | White matter tracts above basal ganglia |
| Choroid plexus | Calcified dots in ventricles (normal variant - bright white) |
| Ambient cistern | CSF around midbrain |
| Tentorium cerebelli | Bright line separating posterior fossa from supratentorial |
| Tentorial notch (incisura) | Opening in tentorium - herniation happens through here |
| Pontocerebellar cistern | CSF space below cerebellum |
LEVEL 6 - High Convexity (Top of Brain)
| Structure | Notes |
|---|---|
| Centrum semiovale | Upper white matter; where white matter lesions appear (MS, small vessel disease) |
| Falx cerebri | Midline bright dural fold |
| Superior sagittal sinus | Bright structure in midline - DO NOT confuse with subarachnoid blood |
| Sulci and gyri | Should be symmetric; effaced unilaterally = edema/mass; bilaterally widened = atrophy |
| Parietal lobe | Dominant lobe at this level |
Bone / Skull Window
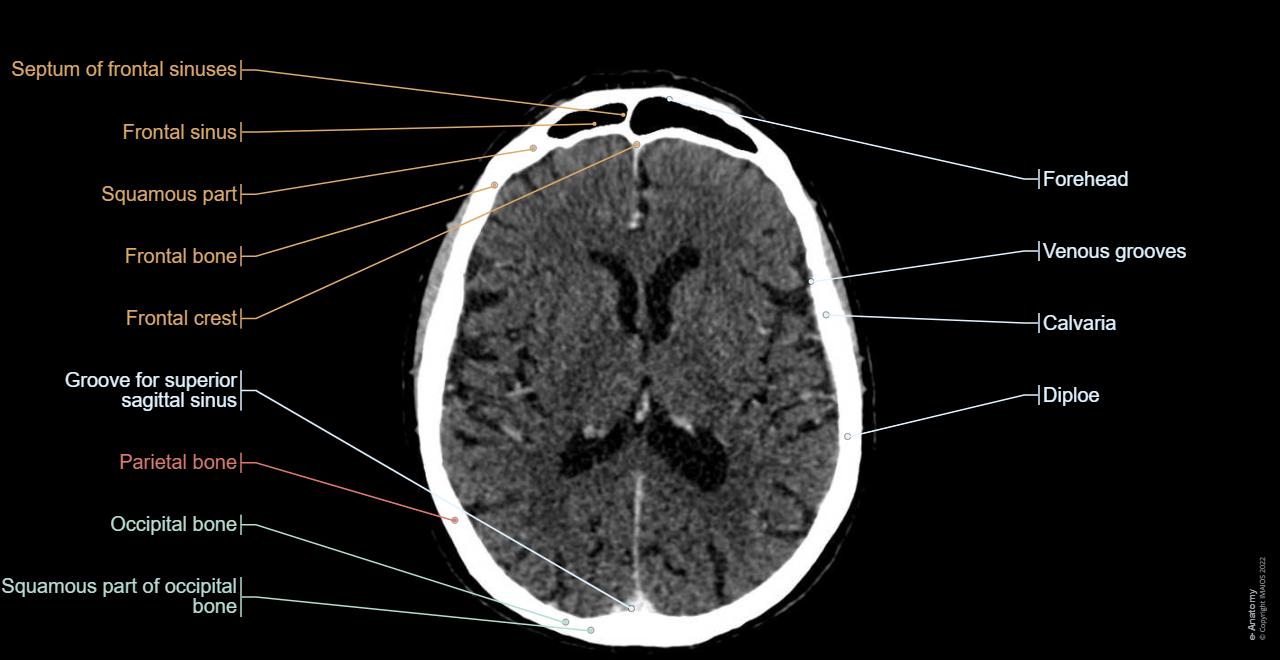
| Structure | What to Look For |
|---|---|
| Diploe | Spongy bone between inner and outer tables - appears darker than cortical bone |
| Frontal bone / Parietal bone / Occipital bone | Know which sutures separate them |
| Frontal sinus | Air-filled space in forehead - opacification = sinusitis |
| Calvaria | The skull cap - look for fractures (linear lucent lines) |
| Venous grooves | Normal channels on inner skull surface - don't mistake for fractures |
| Groove for superior sagittal sinus | Midline groove on inner calvaria |
| Frontal crest | Bony ridge where falx attaches anteriorly |
Fracture vs. venous groove: Fractures are straighter, cross sutures, and don't branch. Venous grooves branch and follow predictable paths.
Sagittal View - Cisterns & Midline Structures
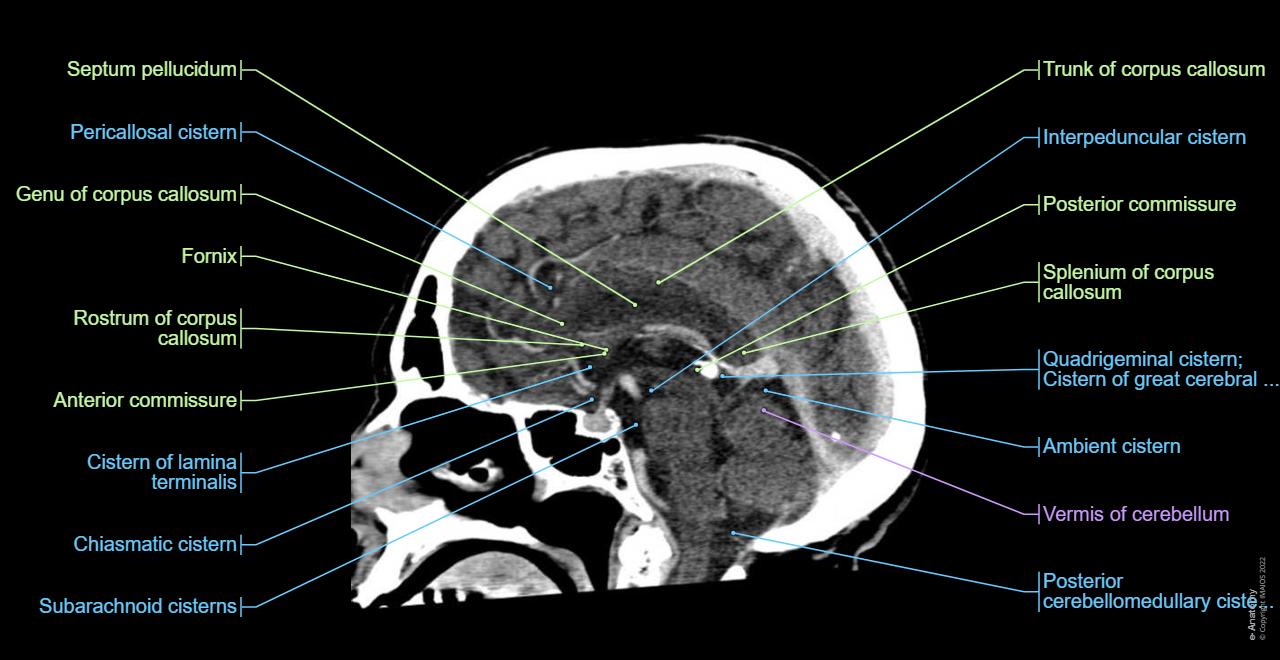
| Structure | Notes |
|---|---|
| Corpus callosum | Genu (front), trunk, splenium (back) - connects hemispheres |
| Septum pellucidum | Thin membrane between lateral ventricles |
| Fornix | Curved white matter tract; part of limbic circuit |
| Anterior & posterior commissures | Midline crossing fiber bundles |
| Pericallosal cistern | CSF above corpus callosum |
| Chiasmatic cistern | Around optic chiasm - optic neuritis/aneurysms here |
| Interpeduncular cistern | Between cerebral peduncles |
| Quadrigeminal cistern | Posterior to midbrain (tectum) |
| Ambient cistern | Around midbrain laterally |
| Vermis of cerebellum | Midline cerebellar structure |
| Posterior cerebellomedullary cistern | Large cistern (cisterna magna) posterior to cerebellum |
Vascular View (CT Angiography / CTA)
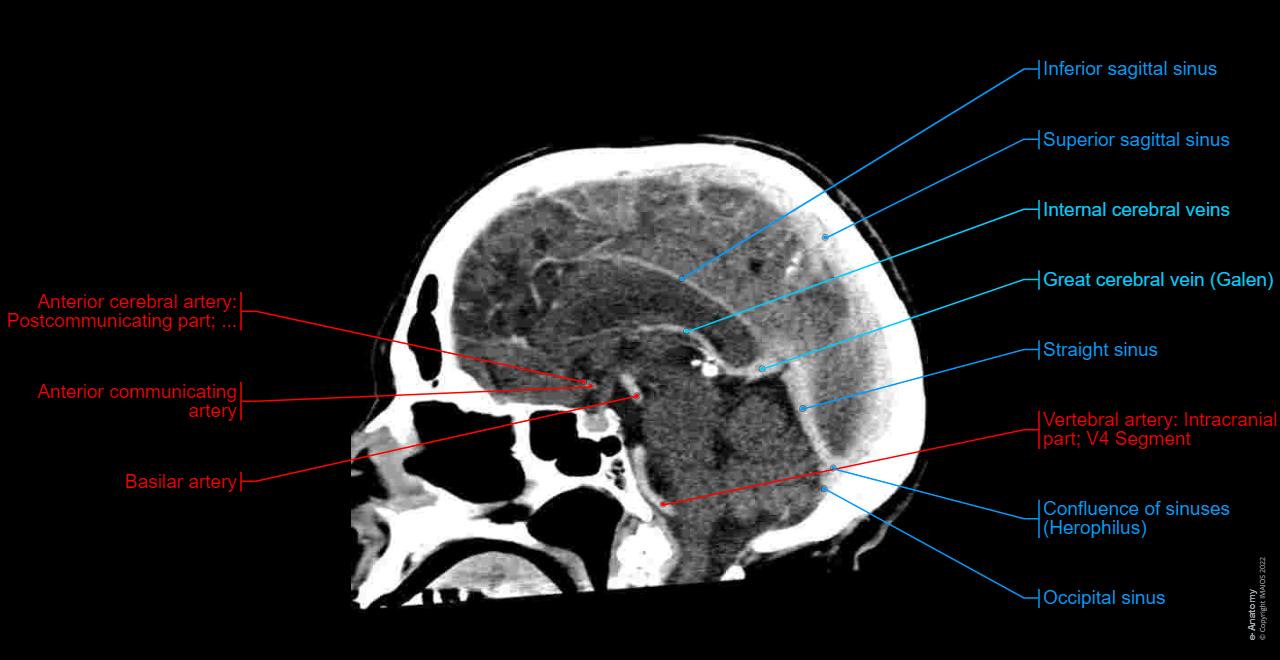
- Anterior cerebral artery (ACA) - runs over corpus callosum; supplies medial frontal/parietal
- Anterior communicating artery (ACoA) - most common aneurysm site!
- Basilar artery - midline anterior to pons; tip aneurysm = "top of basilar" syndrome
- Vertebral artery (V4 segment) - enters foramen magnum
- Superior sagittal sinus - midline on top; thrombosis = paradoxical stroke
- Inferior sagittal sinus - along free edge of falx
- Straight sinus - connects internal cerebral veins to torcular
- Confluence of sinuses (Torcular Herophili) - where sinuses meet at occipital
- Internal cerebral veins - drain deep structures
- Great cerebral vein (of Galen) - joins straight sinus
Quick Summary: "What Level Am I At?" Decision Tree
See cerebellum + pons? → POSTERIOR FOSSA level
See midbrain + suprasellar? → TENTORIAL / BASAL CISTERN level
See basal ganglia + thalamus? → BASAL GANGLIA level (most important!)
See corpus callosum only? → VENTRICULAR level
See only white matter + sulci? → HIGH CONVEXITY level
CT Density Quick Reference (Hounsfield Units)
| Tissue | HU | Looks Like |
|---|---|---|
| Air (sinuses, ventricles) | -1000 | Black |
| Fat (subcutaneous, orbit) | -100 | Very dark gray |
| CSF (ventricles, cisterns, sulci) | 0-18 | Dark gray |
| White matter | 30-34 | Medium gray |
| Gray matter (cortex, deep nuclei) | 37-41 | Slightly brighter medium gray |
| Fresh blood (clot) | 50-100 | Bright white |
| Calcification / Bone | 600-2000 | Brilliant white |
The gray-white difference is subtle but critical. Loss of this differentiation is the earliest CT sign of ischemic stroke.
ct brain point and landmark on real time film normal anatomy teach me easist way
normal CT brain annotated labeled real film axial slices all levels anatomy teaching
ls /home/daytona/workspace/ && python3 -c "import PIL; print('PIL OK')" && python3 -c "import requests; print('requests OK')"
mkdir -p /home/daytona/workspace/ct-brain-atlas/raw && cd /home/daytona/workspace/ct-brain-atlas/raw && python3 -c " import requests, os imgs = { 'axial_basal_ganglia.jpg': 'https://cdn1.imaios.com/i/images/3/3/2/2/472233-1-eng-GB/brain-ct-axial.jpg?caption=1&q=75&w=1280&s=9f4a6d0e46ac7abdfa410dd8f7907413', 'bone_skull.jpg': 'https://cdn1.imaios.com/i/images/8/6/3/2/472368-1-eng-GB/brain-ct-bones.jpg?caption=1&q=75&w=1280&s=9cbe741ff3807b36e1b7eca6994b25c6', 'cranial_base.jpg': 'https://cdn1.imaios.com/i/images/2/2/4/2/472422-1-eng-GB/brain-ct-cranial-base.jpg?caption=1&q=75&w=1280&s=d0cf67f2623720e995dbf1887c8b8554', 'coronal.jpg': 'https://cdn1.imaios.com/i/images/7/8/2/2/472287-1-eng-GB/brain-ct-coronal.jpg?caption=1&q=75&w=1280&s=34a2301a42f296a949e8f8651f9f18ac', 'sagittal_cisterns.jpg': 'https://cdn1.imaios.com/i/images/0/6/2/2/472260-1-eng-GB/brain-ct-sagittal.jpg?caption=1&q=75&w=1280&s=ba5c2bdad196e90936cfa62f93bf0441', 'sagittal_vessels.jpg': 'https://cdn1.imaios.com/i/images/1/4/3/2/472341-1-eng-GB/brain-ct-dural-venous-sinus.jpg?caption=1&q=75&w=1280&s=7f28d46a0fc4ba8612d51b1a2a617ffa', } headers = {'User-Agent': 'Mozilla/5.0 (X11; Linux x86_64) AppleWebKit/537.36'} for name, url in imgs.items(): r = requests.get(url, headers=headers, timeout=15) if r.status_code == 200: with open(name,'wb') as f: f.write(r.content) print(f'OK {name} {len(r.content)} bytes') else: print(f'FAIL {name} {r.status_code}') "
~/ct-brain-atlas/build_atlas.py
"""
CT Brain Normal Anatomy Atlas
Builds annotated teaching images for each CT level with numbered callouts.
"""
from PIL import Image, ImageDraw, ImageFont
import os, math
RAW = "/home/daytona/workspace/ct-brain-atlas/raw"
OUT = "/home/daytona/workspace/ct-brain-atlas/output"
os.makedirs(OUT, exist_ok=True)
# ── Colour palette ─────────────────────────────────────────────────────────────
DOT_COLORS = {
"yellow": (255, 230, 0),
"cyan": ( 0, 220, 255),
"lime": (100, 255, 60),
"orange": (255, 140, 0),
"pink": (255, 80, 180),
"white": (255, 255, 255),
"red": (255, 60, 60),
"sky": ( 80, 180, 255),
}
# Each annotation: (number, label_text, dot_xy_pct, label_side, color)
# dot_xy_pct = (x%, y%) as fraction of image width/height
ANNOTATIONS = {
# ── AXIAL – BASAL GANGLIA LEVEL ───────────────────────────────────────────
"axial_basal_ganglia.jpg": dict(
title="AXIAL CT – BASAL GANGLIA LEVEL\n(Most important level to master)",
bg_color=(10, 10, 30),
items=[
(1, "Frontal Lobe", (0.40, 0.12), "right", "lime"),
(2, "Temporal Lobe", (0.22, 0.42), "left", "lime"),
(3, "Parietal Lobe", (0.28, 0.78), "left", "lime"),
(4, "Occipital Lobe", (0.47, 0.88), "right", "lime"),
(5, "Insula (insular lobe)", (0.30, 0.31), "left", "yellow"),
(6, "Frontal Horn (Lat.Vent.)", (0.56, 0.22), "right", "cyan"),
(7, "3rd Ventricle", (0.55, 0.36), "right", "cyan"),
(8, "Lateral Ventricle Atrium", (0.59, 0.68), "right", "cyan"),
(9, "Choroidal Fissure", (0.62, 0.58), "right", "sky"),
(10, "Basal Nuclei (Ganglia)", (0.42, 0.34), "left", "orange"),
(11, "Thalamus (Diencephalon)", (0.47, 0.42), "left", "orange"),
(12, "Falx Cerebri (midline)", (0.50, 0.50), "right", "white"),
]
),
# ── BONE / SKULL WINDOW ───────────────────────────────────────────────────
"bone_skull.jpg": dict(
title="AXIAL CT – BONE WINDOW\n(Skull, calvaria, fractures)",
bg_color=(10, 10, 30),
items=[
(1, "Frontal Sinus (air = black)", (0.38, 0.07), "right", "cyan"),
(2, "Frontal Bone", (0.28, 0.13), "left", "white"),
(3, "Squamous Part", (0.21, 0.22), "left", "white"),
(4, "Frontal Crest", (0.31, 0.28), "left", "yellow"),
(5, "Venous Grooves", (0.74, 0.27), "right", "orange"),
(6, "Calvaria (skull cap)", (0.78, 0.34), "right", "white"),
(7, "Diploe (spongy bone)", (0.80, 0.42), "right", "yellow"),
(8, "Parietal Bone", (0.22, 0.50), "left", "pink"),
(9, "Gr. for Sup. Sagittal Sinus", (0.24, 0.62), "left", "orange"),
(10, "Occipital Bone", (0.25, 0.72), "left", "white"),
(11, "Brain Parenchyma (grey/white)", (0.56, 0.50), "right", "lime"),
]
),
# ── CRANIAL BASE ──────────────────────────────────────────────────────────
"cranial_base.jpg": dict(
title="AXIAL CT – CRANIAL BASE LEVEL\n(Foramina, sinuses, ear canals)",
bg_color=(10, 10, 30),
items=[
(1, "Nasal Septum", (0.46, 0.08), "right", "white"),
(2, "Maxillary Sinus (air)", (0.63, 0.30), "right", "cyan"),
(3, "Foramen Ovale (CN V3)", (0.32, 0.44), "left", "yellow"),
(4, "Foramen Spinosum\n(mid. meningeal a.)", (0.34, 0.51), "left", "orange"),
(5, "Foramen Lacerum", (0.35, 0.57), "left", "pink"),
(6, "Carotid Canal (ICA)", (0.30, 0.66), "left", "red"),
(7, "Ext. Acoustic Meatus", (0.25, 0.72), "left", "lime"),
(8, "Posterior Fossa\n(cerebellum)", (0.50, 0.80), "right", "sky"),
]
),
# ── CORONAL VIEW ─────────────────────────────────────────────────────────
"coronal.jpg": dict(
title="CORONAL CT – VENTRICULAR ANATOMY\n(Ventricles, thalami, white matter)",
bg_color=(10, 10, 30),
items=[
(1, "Falx Cerebri", (0.49, 0.06), "right", "white"),
(2, "Lateral Ventricle (body)", (0.36, 0.18), "left", "cyan"),
(3, "3rd Ventricle", (0.56, 0.26), "right", "cyan"),
(4, "Choroid Plexus (3rd vent)", (0.55, 0.22), "right", "yellow"),
(5, "Corona Radiata", (0.34, 0.36), "left", "lime"),
(6, "Choroid Plexus (lat.vent)", (0.30, 0.42), "left", "yellow"),
(7, "Thalamus", (0.30, 0.55), "left", "orange"),
(8, "Temporal Horn (lat.vent)", (0.64, 0.50), "right", "sky"),
(9, "Ambient Cistern", (0.60, 0.44), "right", "cyan"),
(10, "Tentorium Cerebelli", (0.58, 0.62), "right", "pink"),
(11, "Cerebellar Hemisphere", (0.46, 0.78), "right", "lime"),
(12, "Pontocerebellar Cistern", (0.55, 0.88), "right", "cyan"),
]
),
# ── SAGITTAL – CISTERNS ───────────────────────────────────────────────────
"sagittal_cisterns.jpg": dict(
title="SAGITTAL CT – CISTERNS & MIDLINE STRUCTURES\n(Corpus callosum, CSF spaces)",
bg_color=(10, 10, 30),
items=[
(1, "Trunk of Corpus Callosum", (0.69, 0.07), "right", "lime"),
(2, "Genu of Corpus Callosum", (0.31, 0.22), "left", "lime"),
(3, "Splenium Corpus Callosum", (0.71, 0.25), "right", "lime"),
(4, "Septum Pellucidum", (0.26, 0.10), "left", "yellow"),
(5, "Fornix", (0.30, 0.32), "left", "yellow"),
(6, "Anterior Commissure", (0.27, 0.44), "left", "orange"),
(7, "Pericallosal Cistern", (0.24, 0.16), "left", "cyan"),
(8, "Chiasmatic Cistern", (0.24, 0.56), "left", "cyan"),
(9, "Interpeduncular Cistern", (0.66, 0.40), "right", "cyan"),
(10, "Quadrigeminal Cistern", (0.70, 0.36), "right", "sky"),
(11, "Vermis of Cerebellum", (0.71, 0.56), "right", "pink"),
(12, "Posterior Cerebellomedullary\nCistern (Cisterna Magna)", (0.70, 0.74), "right", "cyan"),
]
),
# ── SAGITTAL – VESSELS ────────────────────────────────────────────────────
"sagittal_vessels.jpg": dict(
title="SAGITTAL CT – CEREBRAL VESSELS & DURAL SINUSES\n(CTA / contrast-enhanced)",
bg_color=(10, 10, 30),
items=[
(1, "Superior Sagittal Sinus", (0.68, 0.13), "right", "sky"),
(2, "Inferior Sagittal Sinus", (0.67, 0.07), "right", "sky"),
(3, "Internal Cerebral Veins", (0.66, 0.22), "right", "sky"),
(4, "Vein of Galen", (0.66, 0.30), "right", "sky"),
(5, "Straight Sinus", (0.66, 0.38), "right", "sky"),
(6, "Confluence of Sinuses\n(Torcular Herophili)", (0.68, 0.56), "right", "sky"),
(7, "Anterior Cerebral A. (ACA)", (0.28, 0.36), "left", "red"),
(8, "Ant. Communicating A.\n(most common aneurysm)", (0.28, 0.44), "left", "red"),
(9, "Basilar Artery", (0.27, 0.54), "left", "red"),
(10, "Vertebral A. (V4)", (0.32, 0.46), "left", "red"),
(11, "Occipital Sinus", (0.68, 0.80), "right", "sky"),
]
),
}
def try_get_font(size):
"""Try to load a TTF font, fall back to default."""
paths = [
"/usr/share/fonts/truetype/dejavu/DejaVuSans-Bold.ttf",
"/usr/share/fonts/truetype/liberation/LiberationSans-Bold.ttf",
"/usr/share/fonts/truetype/freefont/FreeSansBold.ttf",
"/usr/share/fonts/TTF/DejaVuSans-Bold.ttf",
]
for p in paths:
if os.path.exists(p):
return ImageFont.truetype(p, size)
return ImageFont.load_default()
def draw_callout(draw, dot_xy, number, label, side, color_name, font_label, font_num):
"""Draw a numbered callout: filled circle with number + line + label text."""
col = DOT_COLORS.get(color_name, (255,255,255))
cx, cy = int(dot_xy[0]), int(dot_xy[1])
# Dot (filled circle with dark border)
r = 14
draw.ellipse([cx-r, cy-r, cx+r, cy+r], fill=(0,0,0), outline=col, width=2)
draw.ellipse([cx-r+2, cy-r+2, cx+r-2, cy+r-2], fill=col)
# Number inside dot
num_str = str(number)
bbox = font_num.getbbox(num_str)
nw, nh = bbox[2]-bbox[0], bbox[3]-bbox[1]
draw.text((cx - nw//2, cy - nh//2 - 1), num_str, fill=(0,0,0), font=font_num)
# Leader line
line_len = 55
if side == "right":
lx2 = cx + r + line_len
else:
lx2 = cx - r - line_len
draw.line([(cx + (r if side=="right" else -r), cy), (lx2, cy)], fill=col, width=2)
# Label text (possibly multi-line)
lines = label.split("\n")
line_h = font_label.getbbox("A")[3] + 3
total_h = len(lines) * line_h
ty = cy - total_h // 2
for i, line in enumerate(lines):
bbox = font_label.getbbox(line)
tw = bbox[2] - bbox[0]
if side == "right":
tx = lx2 + 6
else:
tx = lx2 - tw - 6
# Shadow
draw.text((tx+1, ty + i*line_h + 1), line, fill=(0,0,0), font=font_label)
# Text
draw.text((tx, ty + i*line_h), line, fill=col, font=font_label)
def annotate_image(src_path, spec, out_path):
img = Image.open(src_path).convert("RGB")
W, H = img.size
# Add padding on right (or left+right) for labels
PAD_TOP = 85
PAD_SIDE = 0
canvas = Image.new("RGB", (W + PAD_SIDE*2, H + PAD_TOP), spec["bg_color"])
canvas.paste(img, (PAD_SIDE, PAD_TOP))
draw = ImageDraw.Draw(canvas)
font_title = try_get_font(22)
font_label = try_get_font(17)
font_num = try_get_font(13)
# Title
title_lines = spec["title"].split("\n")
for i, tl in enumerate(title_lines):
draw.text((18, 8 + i*28), tl, fill=(255,220,60), font=font_title)
# Draw each annotation
for item in spec["items"]:
num, label, (px, py), side, color = item
# Convert pct to pixel coords (offset by PAD)
cx = PAD_SIDE + int(px * W)
cy = PAD_TOP + int(py * H)
draw_callout(draw, (cx, cy), num, label, side, color, font_label, font_num)
# Legend: number list at bottom
# (skip to keep it clean)
canvas.save(out_path, quality=95)
print(f" Saved: {out_path}")
print("Building CT Brain Atlas annotations...")
for fname, spec in ANNOTATIONS.items():
src = os.path.join(RAW, fname)
out = os.path.join(OUT, fname.replace(".jpg", "_annotated.jpg"))
if os.path.exists(src):
annotate_image(src, spec, out)
else:
print(f" MISSING: {src}")
print("\nDone!")
cd /home/daytona/workspace/ct-brain-atlas && python3 build_atlas.py
~/ct-brain-atlas/build_pdf.py
"""
Assembles the annotated CT images + reference tables into a single PDF atlas.
"""
from reportlab.lib.pagesizes import A4, landscape
from reportlab.platypus import SimpleDocTemplate, Image as RLImage, Paragraph, Spacer, Table, TableStyle, PageBreak, HRFlowable
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.enums import TA_CENTER, TA_LEFT
import os
OUT_DIR = "/home/daytona/workspace/ct-brain-atlas/output"
PDF_PATH = "/home/daytona/workspace/ct-brain-atlas/CT_Brain_Normal_Anatomy_Atlas.pdf"
# Page size: A4 landscape for wide CT images
doc = SimpleDocTemplate(
PDF_PATH,
pagesize=landscape(A4),
rightMargin=1.5*cm, leftMargin=1.5*cm,
topMargin=1.2*cm, bottomMargin=1.2*cm
)
styles = getSampleStyleSheet()
# Custom styles
title_style = ParagraphStyle('AtlasTitle',
fontSize=26, fontName='Helvetica-Bold',
textColor=colors.HexColor('#FFD700'),
backColor=colors.HexColor('#0A0A1E'),
spaceAfter=6, alignment=TA_CENTER,
borderPad=8, leading=32
)
subtitle_style = ParagraphStyle('Subtitle',
fontSize=13, fontName='Helvetica',
textColor=colors.HexColor('#AADDFF'),
alignment=TA_CENTER, spaceAfter=4
)
section_style = ParagraphStyle('Section',
fontSize=16, fontName='Helvetica-Bold',
textColor=colors.HexColor('#FFD700'),
spaceBefore=8, spaceAfter=4
)
body_style = ParagraphStyle('Body',
fontSize=11, fontName='Helvetica',
textColor=colors.HexColor('#E8E8E8'),
spaceAfter=3, leading=15
)
table_header_style = ParagraphStyle('TH',
fontSize=10, fontName='Helvetica-Bold',
textColor=colors.white, alignment=TA_CENTER
)
small_style = ParagraphStyle('Small',
fontSize=9, fontName='Helvetica',
textColor=colors.HexColor('#CCCCCC'),
alignment=TA_CENTER, spaceAfter=2
)
BG = colors.HexColor('#0A0A1E')
TABLE_BG = colors.HexColor('#0D1B2A')
TABLE_HDR = colors.HexColor('#1A3A5C')
TABLE_ALT = colors.HexColor('#0F2030')
GOLD = colors.HexColor('#FFD700')
CYAN = colors.HexColor('#00DCFF')
def make_ref_table(headers, rows):
"""Build a styled reference table."""
data = [headers] + rows
col_widths = None
t = Table(data, colWidths=col_widths, repeatRows=1)
ts = TableStyle([
('BACKGROUND', (0,0), (-1,0), TABLE_HDR),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 10),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#334455')),
('ROWBACKGROUNDS', (0,1), (-1,-1), [TABLE_BG, TABLE_ALT]),
('TEXTCOLOR', (0,1), (-1,-1), colors.HexColor('#D0E8FF')),
('FONTNAME', (0,1), (-1,-1), 'Helvetica'),
('FONTSIZE', (0,1), (-1,-1), 9),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 6),
])
t.setStyle(ts)
return t
# Page width for landscape A4
PW = landscape(A4)[0] - 3*cm # usable width
story = []
# ══════════════════════════════════════════════════════════════════
# COVER PAGE
# ══════════════════════════════════════════════════════════════════
story.append(Spacer(1, 2.5*cm))
story.append(Paragraph("🧠 CT Brain – Normal Anatomy Atlas", title_style))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("Real CT Films with Labeled Landmarks • All Axial Levels • Coronal • Sagittal", subtitle_style))
story.append(Spacer(1, 0.3*cm))
story.append(HRFlowable(width="100%", thickness=1.5, color=GOLD, spaceAfter=6))
story.append(Paragraph("How to Read a Head CT", section_style))
intro_text = [
("<b>Orientation:</b> Images viewed from BELOW looking UP. Patient's LEFT = your RIGHT (like looking up from feet).", body_style),
("<b>Density basics:</b> Brighter = more dense (hyperdense). Darker = less dense (hypodense).", body_style),
("<b>Systematic approach – \"Blood Can Be Very Bad\":</b> B = Blood • C = Cisterns • B = Brain • V = Ventricles • B = Bone", body_style),
]
for txt, sty in intro_text:
story.append(Paragraph(txt, sty))
story.append(Spacer(1, 0.3*cm))
# HU Table
story.append(Paragraph("Hounsfield Units (HU) – CT Density Reference", section_style))
hu_table = make_ref_table(
["Tissue", "HU Range", "Appearance on CT", "Clinical Importance"],
[
["Air (sinuses, lungs)", "-1000 to -600", "BLACK", "Pneumocephalus if in brain"],
["Fat", "-100 to -60", "Very dark gray", "Lipoma, dermoid cyst"],
["Water / CSF", "0 to 18", "Dark gray", "Ventricles, cisterns, sulci"],
["White matter", "30 – 34", "Medium gray", "Periventricular changes in MS"],
["Gray matter (cortex)", "37 – 41", "Slightly brighter", "Earliest stroke: grey-white loss"],
["Fresh blood (clot)", "50 – 100", "BRIGHT WHITE", "Hemorrhage; SDH, EDH, SAH, ICH"],
["Calcification / Bone", "600 – 2000", "BRILLIANT WHITE", "Pineal calcification (normal)"],
]
)
story.append(hu_table)
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("Levels from Bottom to Top (Inferior → Superior)", section_style))
levels_table = make_ref_table(
["Level", "Key Structures Visible", "What to Check"],
[
["1 – Cranial Base", "Foramina, sinuses, ear canals", "Foramen ovale, spinosum, carotid canal"],
["2 – Posterior Fossa", "Cerebellum, pons, 4th ventricle", "4th ventricle open? CP angle clear?"],
["3 – Suprasellar", "Midbrain, basal cisterns, temporal horns","5-pointed cistern open = normal"],
["4 – Basal Ganglia ★", "Basal ganglia, thalamus, lat. ventricles","MOST IMPORTANT LEVEL – check symmetry"],
["5 – Body of Ventricles", "Corpus callosum, lat. ventricles, corona", "Ventricle size; midline shift?"],
["6 – High Convexity", "White matter (centrum semiovale)", "Sulci symmetric? SAH in sulci?"],
["7 – Vertex", "Cortex, sulci, superior sagittal sinus", "Bilateral atrophy vs. normal aging"],
]
)
story.append(levels_table)
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# IMAGE PAGES – one per annotated CT
# ══════════════════════════════════════════════════════════════════
image_specs = [
("axial_basal_ganglia_annotated.jpg",
"LEVEL 4 – AXIAL: BASAL GANGLIA (Most Important Level)",
"This level shows the deepest brain structures. Memorise the layout: cortex → insula → putamen → internal capsule → globus pallidus → thalamus → 3rd ventricle → caudate.",
[
["#", "Structure", "Density", "Clinical Pearl"],
["1", "Frontal Lobe", "Gray (cortex) + white", "Personality, motor planning; glioblastoma common here"],
["2", "Temporal Lobe", "Gray + white", "Memory (hippocampus); herpes encephalitis"],
["3", "Parietal Lobe", "Gray + white", "Spatial awareness, sensory cortex"],
["4", "Occipital Lobe", "Gray + white", "Visual cortex; posterior circulation stroke → vision loss"],
["5", "Insula", "Gray cortex", "Insular Ribbon Sign = earliest MCA stroke sign"],
["6", "Frontal Horn Lat.Vent.", "Dark (CSF)", "Enlarged = hydrocephalus"],
["7", "3rd Ventricle", "Dark slit (CSF)", "Widened in hydrocephalus / thalamic atrophy"],
["8", "Lateral Vent. Atrium", "Dark (CSF)", "Choroid plexus calcification = normal"],
["9", "Choroidal Fissure", "Dark (CSF)", "Dilated = temporal lobe atrophy"],
["10", "Basal Ganglia", "Slightly bright (gray)", "Hypertensive bleed favorite site (putamen)"],
["11", "Thalamus", "Slightly bright (gray)", "Deep infarcts; thalamic bleed = drowsiness"],
["12", "Falx Cerebri", "Bright (dura)", "Should be MIDLINE; shift = mass effect"],
]
),
("bone_skull_annotated.jpg",
"BONE WINDOW – SKULL ANATOMY",
"Always switch to bone window to assess the calvaria. Linear lucent lines = fractures. Diploe = spongy bone between inner and outer cortical tables.",
[
["#", "Structure", "Notes", "Pathology to Look For"],
["1", "Frontal Sinus", "Air = black", "Opacification = sinusitis; fracture → pneumocephalus"],
["2", "Frontal Bone", "Bright white", "Linear fracture = lucent line crossing sutures"],
["3", "Squamous Part", "Temporal bone squama", "Temporal bone fracture → epidural hematoma"],
["4", "Frontal Crest", "Falx attachment", "Landmark for midline"],
["5", "Venous Grooves", "Branch; don't cross sutures","Don't mistake for fracture – grooves branch"],
["6", "Calvaria", "3 layers: inner/outer/diploe","Depressed fracture → surgical elevation"],
["7", "Diploe", "Spongy, slightly darker", "Lytic lesion = metastasis / myeloma"],
["8", "Parietal Bone", "Behind temporal", "Parietal fracture can injure SSS"],
["9", "Sup. Sagittal Sinus Groove", "Midline groove", "SSS thrombosis → venous infarct"],
["10","Occipital Bone", "Posterior", "Contrecoup injury from frontal impact"],
["11","Brain parenchyma", "Gray (brain window better)", "Use brain window to assess brain, bone window for skull"],
]
),
("cranial_base_annotated.jpg",
"LEVEL 1 – CRANIAL BASE (Lowest Slices)",
"The base of the skull shows important foramina and paranasal sinuses. Essential for trauma and skull base tumour evaluation.",
[
["#", "Structure", "Contents", "Clinical Pearl"],
["1", "Nasal Septum", "Bone + cartilage", "Deviation normal; septal haematoma in trauma"],
["2", "Maxillary Sinus", "Air (black)", "Opacification = sinusitis, fracture, blood"],
["3", "Foramen Ovale", "CN V3 (mandibular nerve)", "Perineural spread of parotid tumours"],
["4", "Foramen Spinosum", "Middle meningeal artery", "Rupture = epidural haematoma"],
["5", "Foramen Lacerum", "Fibrocartilage/ICA", "Skull base tumour spread"],
["6", "Carotid Canal", "Internal carotid artery", "ICA dissection visible on CT-A"],
["7", "Ext. Acoustic Meatus","Ear canal", "Haemotympanum in temporal bone fracture"],
["8", "Posterior Fossa", "Cerebellum occupies this", "Foramen magnum = brainstem exits here"],
]
),
("coronal_annotated.jpg",
"CORONAL CT – VENTRICULAR ANATOMY",
"The coronal plane shows the relationship between ventricles, thalami, and white matter tracts. Best for assessing hydrocephalus and temporal horn dilatation.",
[
["#", "Structure", "Normal Appearance", "Pathology"],
["1", "Falx Cerebri", "Midline bright dural fold", "Shift = subdural / mass"],
["2", "Lateral Ventricle", "Symmetric dark CSF spaces", "Asymmetric = obstruction"],
["3", "3rd Ventricle", "Midline slit", "Widened = hydro / atrophy"],
["4", "Choroid Plexus", "Calcified dots (normal)", "Xanthogranulomas – benign"],
["5", "Corona Radiata", "White matter tracts", "MS plaques / lacunar infarcts"],
["6", "Caudate Tail", "Lateral ventricle wall", "Caudate atrophy = Huntington's"],
["7", "Thalamus", "Oval gray masses", "Bilateral lesions = metabolic / Wernicke's"],
["8", "Temporal Horn", "Thin slit (<2mm)", ">2mm = early hydrocephalus or atrophy"],
["9", "Ambient Cistern", "CSF around midbrain", "Effaced = transtentorial herniation!"],
["10", "Tentorium Cerebelli", "Bright dural shelf", "Landmark separating supra from infratentorial"],
["11", "Cerebellar Hemi.", "Gray-white folia pattern", "Infarct in PICA = lateral medullary syndrome"],
["12", "Pontocerebellar Cist.","CSF space", "Mass = acoustic neuroma"],
]
),
("sagittal_cisterns_annotated.jpg",
"SAGITTAL CT – CISTERNS & CORPUS CALLOSUM",
"The sagittal plane reveals midline structures and subarachnoid cisterns beautifully. Cisterns should all be DARK (CSF). White = subarachnoid haemorrhage.",
[
["#", "Structure", "Function", "Clinical Pearl"],
["1", "Corpus Callosum (trunk)", "Connects hemispheres", "Genu: frontal; Splenium: parietal/occipital"],
["2", "Genu Corpus Callosum", "Frontal connections", "Butterfly glioma crosses here"],
["3", "Splenium Corp. Call.", "Posterior connections", "Disconnection syndrome if severed"],
["4", "Septum Pellucidum", "Between lateral ventricles", "Absent = holoprosencephaly"],
["5", "Fornix", "Hippocampal output tract", "Atrophy in Alzheimer's disease"],
["6", "Anterior Commissure", "Connects temporal lobes", "Landmark for stereotactic surgery"],
["7", "Pericallosal Cistern", "CSF above corpus callosum", "SAH: blood fills this cistern"],
["8", "Chiasmatic Cistern", "Around optic chiasm", "Aneurysm of ACA / Acomm ruptures here"],
["9", "Interpeduncular Cist.", "Between cerebral peduncles", "SAH: star-shaped bleed here"],
["10", "Quadrigeminal Cistern", "Posterior to midbrain", "Effaced = upward transtentorial herniation"],
["11", "Vermis Cerebellum", "Midline coordination", "Atrophy = alcoholism"],
["12", "Cisterna Magna", "Large posterior CSF space", "Mega cisterna magna = normal variant"],
]
),
("sagittal_vessels_annotated.jpg",
"SAGITTAL CT – CEREBRAL VESSELS & DURAL SINUSES (CTA)",
"CT angiography shows arteries (bright with contrast) and dural venous sinuses. Key for stroke, aneurysm, and venous thrombosis.",
[
["#", "Structure", "Type", "Clinical Pearl"],
["1", "Superior Sagittal Sinus", "Venous sinus", "Thrombosis → headache + venous infarct (paradoxical)"],
["2", "Inferior Sagittal Sinus", "Venous sinus", "Joins straight sinus at falx free edge"],
["3", "Internal Cerebral Veins", "Deep vein", "Drains basal ganglia / thalamus"],
["4", "Vein of Galen", "Deep vein", "AVM of Galen in neonates → high-output cardiac failure"],
["5", "Straight Sinus", "Venous sinus", "Connects deep veins to torcular"],
["6", "Torcular Herophili", "Venous sinus", "Confluence at internal occipital protuberance"],
["7", "Anterior Cerebral A.", "Artery", "Supplies medial frontal/parietal; A1/A2 aneurysms"],
["8", "Anterior Communicating A.", "Artery", "Most common intracranial aneurysm site!"],
["9", "Basilar Artery", "Artery", "Top of basilar occlusion = 'locked-in' or coma"],
["10", "Vertebral A. (V4)", "Artery", "Dissection after neck manipulation"],
["11", "Occipital Sinus", "Venous sinus", "Variable; present in ~50%"],
]
),
]
for img_file, section_title, description, table_data in image_specs:
img_path = os.path.join(OUT_DIR, img_file)
if not os.path.exists(img_path):
print(f" Missing image: {img_path}")
continue
# Section header
story.append(Paragraph(section_title, section_style))
story.append(HRFlowable(width="100%", thickness=1, color=GOLD, spaceAfter=4))
story.append(Paragraph(description, body_style))
story.append(Spacer(1, 0.25*cm))
# Image — fit to available width
from PIL import Image as PILImage
pil = PILImage.open(img_path)
iw, ih = pil.size
max_w = PW
max_h = 10.5*cm
scale = min(max_w/iw, max_h/ih)
disp_w = iw * scale
disp_h = ih * scale
story.append(RLImage(img_path, width=disp_w, height=disp_h))
story.append(Spacer(1, 0.3*cm))
# Reference table
story.append(make_ref_table(table_data[0], table_data[1:]))
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# QUICK-REFERENCE BACK PAGE
# ══════════════════════════════════════════════════════════════════
story.append(Paragraph("QUICK-REFERENCE: What Am I Looking At?", section_style))
story.append(HRFlowable(width="100%", thickness=1, color=GOLD, spaceAfter=6))
story.append(Paragraph("<b>Which level am I at? → Look for these landmarks:</b>", body_style))
landmark_table = make_ref_table(
["If you see...", "You are at...", "Key structures to identify"],
[
["Cerebellum + pons + 4th ventricle", "Posterior fossa", "Cerebellum, pons, CP angles, mastoid air cells"],
["Midbrain + 5-pointed cistern", "Suprasellar level", "Basal cisterns, temporal horns, ambient cistern"],
["Basal ganglia + thalamus + lat.vent.", "Basal ganglia ★", "Putamen, caudate, internal capsule, 3rd ventricle"],
["Corpus callosum only (no BG)", "Body of ventricles", "Body lat.vent., corpus callosum, corona radiata"],
["White matter only, many sulci", "High convexity", "Centrum semiovale, superior sulci, falx"],
["Cortex only, narrow slices", "Vertex", "Superior sagittal sinus, sulci, parietal cortex"],
]
)
story.append(landmark_table)
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Density quick-reference (no numbers needed – just remember):</b>", body_style))
density_table = make_ref_table(
["If it looks...", "It is probably...", "Abnormal if..."],
[
["Black (darkest)", "Air or fat", "Air in brain parenchyma = pneumocephalus"],
["Dark gray", "CSF (ventricles, cisterns)", "Absent cisterns = brainstem compression"],
["Medium gray", "Brain tissue (normal)", "Focal hypodensity = edema / infarct"],
["Slightly brighter", "Gray matter vs white matter","Loss of contrast = early ischemic stroke"],
["Bright white", "Fresh blood / calcium", "New hyperdensity = hemorrhage"],
["Brilliant white", "Bone / iodine contrast", "Dense MCA = thrombosis!"],
]
)
story.append(density_table)
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>The 5 Cisterns to ALWAYS check (should all be DARK):</b>", body_style))
cistern_table = make_ref_table(
["Cistern", "Location", "If white/filled = "],
[
["Suprasellar cistern", "Above pituitary, star-shaped", "Subarachnoid haemorrhage (SAH)"],
["Sylvian fissure (×2)", "Between frontal + temporal lobes", "SAH or subdural spreading"],
["Ambient cistern (×2)", "Around midbrain laterally", "Herniation effacing it = emergency"],
["Quadrigeminal cistern", "Posterior to midbrain (pineal)", "Upward transtentorial herniation"],
["Interpeduncular cistern", "Between cerebral peduncles", "Aneurysm / SAH from Acomm rupture"],
]
)
story.append(cistern_table)
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("Source: e-Anatomy / IMAIOS (Micheau & Hoa, 2022) • Neuroanatomy through Clinical Cases 3rd Ed. • Brigham & Women's Head CT Guide", small_style))
# Build
doc.build(story)
print(f"\nPDF atlas saved to:\n {PDF_PATH}")
cd /home/daytona/workspace/ct-brain-atlas && python3 build_pdf.py 2>&1
ls -lh /home/daytona/workspace/ct-brain-atlas/CT_Brain_Normal_Anatomy_Atlas.pdf && ls -lh /home/daytona/workspace/ct-brain-atlas/output/
python3 -c " from PIL import Image img = Image.open('/home/daytona/workspace/ct-brain-atlas/output/axial_basal_ganglia_annotated.jpg') print(f'Size: {img.size}, Mode: {img.mode}') # Verify image content - check it is not blank import numpy as np arr = np.array(img) print(f'Min: {arr.min()}, Max: {arr.max()}, Mean: {arr.mean():.1f}') print('Image OK') "
🧠 CT Brain Normal Anatomy - Real Films with Pointers
What I built for you:
Download the Full PDF Atlas:
CT Brain Normal Anatomy Atlas
PDF Document · PDF
Download Individual Annotated Images:
| Image | Level | Structures Labeled |
|---|---|---|
axial basal ganglia annotated Image · JPG | ⭐ Most important level | 12 structures: frontal/temporal/parietal/occipital lobes, insula, ventricles, basal ganglia, thalamus, falx |
bone skull annotated Image · JPG | Skull/calvaria | 11 structures: frontal bone, diploe, venous grooves, sinuses, parietal/occipital bones, sagittal sinus groove |
cranial base annotated Image · JPG | Lowest level | 8 structures: foramen ovale, foramen spinosum, carotid canal, maxillary sinus, ear canal |
coronal annotated Image · JPG | Ventricular anatomy | 12 structures: lateral ventricles, 3rd ventricle, thalamus, corona radiata, tentorium, temporal horn |
sagittal cisterns annotated Image · JPG | Midline structures | 12 structures: corpus callosum genu/trunk/splenium, all cisterns, fornix, commissures |
sagittal vessels annotated Image · JPG | Cerebrovascular | 11 structures: ACA, AComm, basilar artery, SSS, straight sinus, vein of Galen, torcular |
The Simplest Way to Learn - 3 Rules:
- ⬛ Black = Air (sinuses, pneumocephalus)
- 🌫️ Dark gray = CSF (ventricles, cisterns - should be OPEN and dark)
- 🔘 Medium gray = Normal brain (gray > white matter, just slightly)
- ⬜ Bright white = Fresh blood OR calcification OR bone
- 🩶 Brilliant white = Bone or contrast
Show real pathology examples: hemorrhage vs infarct vs tumor on the same anatomy
CT brain ischemic stroke MCA infarct hypodense wedge real scan labeled teaching radiology
mkdir -p /home/daytona/workspace/ct-brain-atlas/pathology && cd /home/daytona/workspace/ct-brain-atlas/pathology && python3 -c " import requests imgs = { # From textbooks (orris CDN) 'ich_temporal.png': 'https://cdn.orris.care/cdss_images/7cc35d765867ed0e514c3b2c567af15ef930b966901b9e83443c259540e3b81d.png', 'sah_cisterns.png': 'https://cdn.orris.care/cdss_images/756de02eb6c0b258d6d92275421cbf02ac1c614620e157132109fb5f293892c5.png', 'sah_aneurysm.png': 'https://cdn.orris.care/cdss_images/7845f49ce847435117d63b1de4368a33ada3b7db76e8d19f16f7149873f37bc1.png', 'edh_pair.png': 'https://cdn.orris.care/cdss_images/9fd3febacd67f3f133aa40e7915c8263afe26d1a932f42074f23ecf5365172b4.png', 'sdh_acute.png': 'https://cdn.orris.care/cdss_images/f7700f44242f6eab6d2a5cff8fdefc39b93a4a29f4d263dd41f8fcf460dbc063.png', 'sdh_serial.png': 'https://cdn.orris.care/cdss_images/23625ee7d61e35212a7e6827338d698ad56d3c9168fc0fa2050f9585da55aca9.png', # MCA infarct from radiologymasterclass 'mca_infarct.jpg': 'https://www.radiologymasterclass.co.uk/images/ct/ct-brain/templates/mca_infarct/mca_large-12-02.jpg', } headers = {'User-Agent': 'Mozilla/5.0 (X11; Linux x86_64)'} for name, url in imgs.items(): r = requests.get(url, headers=headers, timeout=15) if r.status_code == 200: with open(name,'wb') as f: f.write(r.content) print(f'OK {name} ({len(r.content)//1024}KB)') else: print(f'FAIL {name} {r.status_code}') "
~/ct-brain-atlas/build_pathology_atlas.py
"""
CT Brain Pathology Comparison Atlas
Builds annotated + side-by-side comparison pages for:
Hemorrhage (ICH, EDH, SDH, SAH) vs Ischemic Infarct vs Tumor
"""
from PIL import Image, ImageDraw, ImageFont
from reportlab.lib.pagesizes import A4, landscape
from reportlab.platypus import (SimpleDocTemplate, Image as RLImage, Paragraph,
Spacer, Table, TableStyle, PageBreak, HRFlowable)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib import colors
from reportlab.lib.units import cm
from reportlab.lib.enums import TA_CENTER, TA_LEFT
import os, textwrap
RAW = "/home/daytona/workspace/ct-brain-atlas/pathology"
OUT = "/home/daytona/workspace/ct-brain-atlas/pathology_out"
PDF = "/home/daytona/workspace/ct-brain-atlas/CT_Brain_Pathology_Atlas.pdf"
os.makedirs(OUT, exist_ok=True)
# ── COLOURS ──────────────────────────────────────────────────────────────────
RED = (255, 50, 50)
YELLOW = (255, 230, 0)
CYAN = ( 0, 220, 255)
LIME = (100, 255, 60)
ORANGE = (255, 140, 0)
PINK = (255, 80, 180)
WHITE = (255, 255, 255)
SKY = ( 80, 180, 255)
GREEN = ( 60, 220, 120)
def try_font(size, bold=True):
paths = [
"/usr/share/fonts/truetype/dejavu/DejaVuSans-Bold.ttf" if bold else
"/usr/share/fonts/truetype/dejavu/DejaVuSans.ttf",
"/usr/share/fonts/truetype/liberation/LiberationSans-Bold.ttf",
"/usr/share/fonts/truetype/freefont/FreeSansBold.ttf",
]
for p in paths:
if os.path.exists(p):
return ImageFont.truetype(p, size)
return ImageFont.load_default()
def draw_arrow_label(draw, tip_xy, label, color, font, side="right", offset=60):
"""Draw a filled arrow + label. tip_xy = where arrow points."""
cx, cy = int(tip_xy[0]), int(tip_xy[1])
# Arrow line
if side == "right":
lx = cx + offset
else:
lx = cx - offset
draw.line([(cx, cy), (lx, cy)], fill=color, width=3)
# Arrowhead
ah = 8
if side == "right":
draw.polygon([(cx, cy), (cx+ah, cy-ah//2), (cx+ah, cy+ah//2)], fill=color)
else:
draw.polygon([(cx, cy), (cx-ah, cy-ah//2), (cx-ah, cy+ah//2)], fill=color)
# Label
lines = label.split("\n")
lh = font.getbbox("A")[3] + 2
th = len(lines) * lh
ty = cy - th//2
for i, line in enumerate(lines):
bbox = font.getbbox(line)
tw = bbox[2] - bbox[0]
if side == "right":
tx = lx + 4
else:
tx = lx - tw - 4
# shadow
draw.text((tx+1, ty+i*lh+1), line, fill=(0,0,0), font=font)
draw.text((tx, ty+i*lh), line, fill=color, font=font)
def draw_circle_marker(draw, xy, r, color):
cx, cy = int(xy[0]), int(xy[1])
for w in range(3, 0, -1):
draw.ellipse([cx-r-w, cy-r-w, cx+r+w, cy+r+w], outline=(0,0,0), width=1)
draw.ellipse([cx-r, cy-r, cx+r, cy+r], outline=color, width=3)
def add_title_bar(draw, text, W, col, font):
draw.rectangle([0, 0, W, 46], fill=(10,10,30))
bbox = font.getbbox(text)
tw = bbox[2]-bbox[0]
draw.text(((W-tw)//2, 8), text, fill=col, font=font)
def annotate(src, out_name, title, annotations, title_color=YELLOW, crop=None):
"""
annotations: list of (tip_xy_pct, label, color, side)
tip_xy_pct: (x%, y%) of the *image* (after any crop)
"""
img = Image.open(src).convert("RGB")
if crop:
img = img.crop(crop) # (left, top, right, bottom)
W, H = img.size
PAD = 50 # top title bar
canvas = Image.new("RGB", (W, H + PAD), (10,10,30))
canvas.paste(img, (0, PAD))
draw = ImageDraw.Draw(canvas)
font_title = try_font(20)
font_label = try_font(15)
add_title_bar(draw, title, W, title_color, font_title)
for (px, py), label, color, side in annotations:
tip = (int(px * W), PAD + int(py * H))
draw_arrow_label(draw, tip, label, color, font_label, side)
draw_circle_marker(draw, tip, 6, color)
out_path = os.path.join(OUT, out_name)
canvas.save(out_path, quality=95)
print(f" {out_path}")
return out_path
print("Building pathology annotations...")
paths = {}
# ─────────────────────────────────────────────────────────────────────────────
# 1. ICH – Intracerebral Hemorrhage (right temporal lobe)
# ─────────────────────────────────────────────────────────────────────────────
paths["ich"] = annotate(
os.path.join(RAW, "ich_temporal.png"),
"ich_annotated.jpg",
"INTRACEREBRAL HEMORRHAGE (ICH) – Right Temporal Lobe",
[
((0.30, 0.35), "HYPERDENSE MASS\n(50-100 HU = fresh blood)", RED, "right"),
((0.22, 0.28), "Round/oval shape\n= ICH characteristic", YELLOW, "right"),
((0.52, 0.50), "Contralateral\nnormal brain\n(gray = correct density)", LIME, "left"),
((0.18, 0.55), "Skull (white)\n= bone", WHITE, "right"),
],
title_color=RED
)
# ─────────────────────────────────────────────────────────────────────────────
# 2. SAH – Subarachnoid Hemorrhage (diffuse, sulci & cisterns)
# ─────────────────────────────────────────────────────────────────────────────
paths["sah"] = annotate(
os.path.join(RAW, "sah_cisterns.png"),
"sah_annotated.jpg",
"SUBARACHNOID HEMORRHAGE (SAH) – Blood fills CSF spaces",
[
((0.72, 0.22), "HYPERDENSE BLOOD\nin sulci & cisterns", RED, "left"),
((0.30, 0.18), "Blood in\nright sulci", ORANGE, "right"),
((0.47, 0.48), "Interhemispheric\nfissure blood", RED, "right"),
((0.48, 0.70), "Blood tracking\nalong gyri", ORANGE, "left"),
((0.58, 0.35), "Ventricles\nstill dark (ok)", CYAN, "left"),
],
title_color=ORANGE
)
# ─────────────────────────────────────────────────────────────────────────────
# 3. SAH (aneurysmal) – LEFT panel (basal cisterns level)
# Crop left half of the paired image
# ─────────────────────────────────────────────────────────────────────────────
img_sah2 = Image.open(os.path.join(RAW, "sah_aneurysm.png")).convert("RGB")
W2, H2 = img_sah2.size
left_half = img_sah2.crop((0, 0, W2//2, H2))
left_half.save(os.path.join(RAW, "sah_basilar_left.png"))
paths["sah_basilar"] = annotate(
os.path.join(RAW, "sah_basilar_left.png"),
"sah_basilar_annotated.jpg",
"SAH – Basilar Aneurysm Rupture (Basal Cisterns + IVH)",
[
((0.50, 0.30), "Bilateral\nhyperdense blood\nin cisterns", RED, "left"),
((0.28, 0.52), "Blood in\n3rd ventricle\n(IVH)", ORANGE, "right"),
((0.52, 0.64), "Enlarged temporal\nhorns = acute\nhydrocephalus!", YELLOW, "left"),
((0.75, 0.55), "Blood layering\nin posterior\nhorn (CSF level)", RED, "left"),
],
title_color=ORANGE
)
# ─────────────────────────────────────────────────────────────────────────────
# 4. EDH – Epidural Hematoma (left panel of pair = brain window)
# ─────────────────────────────────────────────────────────────────────────────
img_edh = Image.open(os.path.join(RAW, "edh_pair.png")).convert("RGB")
W3, H3 = img_edh.size
edh_brain = img_edh.crop((0, 0, W3//2, H3))
edh_brain.save(os.path.join(RAW, "edh_brain.png"))
paths["edh"] = annotate(
os.path.join(RAW, "edh_brain.png"),
"edh_annotated.jpg",
"EPIDURAL HEMATOMA (EDH) – Lens / Biconvex Shape",
[
((0.15, 0.35), "BICONVEX\nhyperdense\ncollection\n= EDH", RED, "right"),
((0.28, 0.52), "Brain pushed\nmedially\n(mass effect)", YELLOW, "right"),
((0.60, 0.50), "Contralateral\nnormal brain", LIME, "left"),
((0.50, 0.25), "Falx cerebri\n(midline)", WHITE, "right"),
],
title_color=RED
)
# ─────────────────────────────────────────────────────────────────────────────
# 5. SDH acute – Acute Subdural Hematoma
# ─────────────────────────────────────────────────────────────────────────────
paths["sdh"] = annotate(
os.path.join(RAW, "sdh_acute.png"),
"sdh_annotated.jpg",
"ACUTE SUBDURAL HEMATOMA (SDH) – Crescent Shape + Midline Shift",
[
((0.15, 0.38), "CRESCENT-SHAPED\nhyperdense SDH\n(crosses sutures)", RED, "right"),
((0.60, 0.40), "MIDLINE SHIFT\nto left = mass effect\n(brain swelling)", YELLOW, "left"),
((0.48, 0.48), "Falx displaced\nto left", ORANGE, "right"),
((0.78, 0.35), "Compressed\nright hemisphere", PINK, "left"),
],
title_color=RED
)
# ─────────────────────────────────────────────────────────────────────────────
# 6. MCA infarct – Ischemic Stroke
# ─────────────────────────────────────────────────────────────────────────────
paths["infarct"] = annotate(
os.path.join(RAW, "mca_infarct.jpg"),
"mca_infarct_annotated.jpg",
"ISCHEMIC STROKE – MCA Territory Infarct (HYPODENSE)",
[
((0.32, 0.35), "LARGE HYPODENSE\nwedge = MCA\nterritory infarct", CYAN, "right"),
((0.40, 0.52), "Loss of\ngray-white\ndifferentiation", YELLOW, "right"),
((0.62, 0.38), "Mass effect:\nventricle\ncompressed", ORANGE, "left"),
((0.70, 0.55), "Contralateral\nnormal\nbrain density", LIME, "left"),
((0.46, 0.22), "Falx still\nmidline (no\nlarge shift yet)", WHITE, "right"),
],
title_color=CYAN
)
print("\nAll pathology images annotated.")
print("\nBuilding PDF...")
# ─────────────────────────────────────────────────────────────────────────────
# PDF ATLAS
# ─────────────────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(PDF, pagesize=landscape(A4),
rightMargin=1.2*cm, leftMargin=1.2*cm,
topMargin=1*cm, bottomMargin=1*cm)
styles = getSampleStyleSheet()
BG = colors.HexColor('#0A0A1E')
GOLD_C= colors.HexColor('#FFD700')
CYAN_C= colors.HexColor('#00DCFF')
RED_C = colors.HexColor('#FF3232')
GRN_C = colors.HexColor('#64FF3C')
def sty(name, **kw):
return ParagraphStyle(name, **kw)
title_sty = sty('T', fontSize=24, fontName='Helvetica-Bold',
textColor=GOLD_C, alignment=TA_CENTER, spaceAfter=4, leading=30)
sub_sty = sty('S', fontSize=11, fontName='Helvetica',
textColor=colors.HexColor('#AADDFF'), alignment=TA_CENTER, spaceAfter=6)
sec_sty = sty('Sec', fontSize=15, fontName='Helvetica-Bold',
textColor=GOLD_C, spaceBefore=6, spaceAfter=3)
body_sty = sty('B', fontSize=10, fontName='Helvetica',
textColor=colors.HexColor('#E0E8FF'), spaceAfter=2, leading=14)
small_sty = sty('Sm', fontSize=8, fontName='Helvetica',
textColor=colors.HexColor('#AAAAAA'), alignment=TA_CENTER)
def make_table(headers, rows, col_widths=None):
data = [headers] + rows
t = Table(data, colWidths=col_widths, repeatRows=1)
ts = TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1A3A5C')),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 9),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#334455')),
('ROWBACKGROUNDS', (0,1), (-1,-1),
[colors.HexColor('#0D1B2A'), colors.HexColor('#0F2030')]),
('TEXTCOLOR', (0,1), (-1,-1), colors.HexColor('#D0E8FF')),
('FONTNAME', (0,1), (-1,-1), 'Helvetica'),
('FONTSIZE', (0,1), (-1,-1), 8),
('TOPPADDING', (0,0), (-1,-1), 3),
('BOTTOMPADDING', (0,0), (-1,-1), 3),
('LEFTPADDING', (0,0), (-1,-1), 5),
])
t.setStyle(ts)
return t
PW = landscape(A4)[0] - 2.4*cm # usable width
def img_flowable(path, max_w, max_h):
from PIL import Image as PILImage
pil = PILImage.open(path)
iw, ih = pil.size
scale = min(max_w/iw, max_h/ih)
return RLImage(path, width=iw*scale, height=ih*scale)
story = []
# ── COVER ────────────────────────────────────────────────────────────────────
story.append(Spacer(1, 1.5*cm))
story.append(Paragraph("🧠 CT Brain – Pathology Comparison Atlas", title_sty))
story.append(Paragraph("Real CT Films: Hemorrhage • Infarct • Tumor • Side-by-Side", sub_sty))
story.append(HRFlowable(width="100%", thickness=1.5, color=GOLD_C, spaceAfter=8))
story.append(Paragraph("The #1 Rule: Bright = Blood / Bone / Calcium | Dark = CSF / Edema / Infarct", body_sty))
story.append(Spacer(1, 0.3*cm))
# Master comparison table
story.append(Paragraph("Master Comparison: Hemorrhage vs Infarct vs Tumor", sec_sty))
comp_table = make_table(
["Condition", "CT Density", "Shape", "Location", "Time Course", "Emergency?"],
[
["ICH", "HYPERDENSE (white)", "Round/oval", "Deep: putamen, thalamus,\npons, cerebellum", "Sudden onset", "YES – urgent BP control"],
["EDH", "HYPERDENSE (white)", "BICONVEX\n(lens-shaped)", "Between skull & dura\n(temporal most common)", "Minutes-hours\n(lucid interval)", "SURGICAL EMERGENCY"],
["Acute SDH", "HYPERDENSE (white)", "CRESCENT\n(concave)", "Between dura & arachnoid\n(crosses sutures)", "Trauma → rapid", "Often surgical"],
["Chronic SDH", "HYPODENSE (dark)", "Crescent", "Same as SDH", "Weeks-months", "Conservative vs burr hole"],
["SAH", "HYPERDENSE (white)", "Fills sulci &\ncisterns", "CSF spaces: Sylvian,\nbasal cisterns, sulci", "Thunderclap HA\n'worst of life'", "YES – secure aneurysm"],
["Ischemic Stroke", "HYPODENSE (dark)", "WEDGE (vascular\nterritory)", "Cortex + white matter\n(respects vascular territory)", ">6h for CT change\nfirst 3h often normal", "YES – tPA window"],
["Tumor (GBM)", "Mixed/ring", "Round, irregular", "Any location – no\nvascular territory pattern", "Weeks of\nwaxing symptoms", "Neurosurgery referral"],
["Abscess", "Hypodense core\n+ ring enhance", "Round, smooth ring", "Any – often frontal\nor temporal", "Days-weeks\nfever + neuro signs", "Drain + antibiotics"],
]
)
story.append(comp_table)
story.append(PageBreak())
# ── HEMORRHAGE SECTION ────────────────────────────────────────────────────────
story.append(Paragraph("SECTION 1: HEMORRHAGE – 'Bright White = Blood'", sec_sty))
story.append(HRFlowable(width="100%", thickness=1, color=RED_C, spaceAfter=6))
story.append(Paragraph(
"All hemorrhages appear <b>HYPERDENSE (bright white)</b> on non-contrast CT in the acute phase "
"because clotting blood has high HU (50-100). They differ in <b>SHAPE and LOCATION</b>.",
body_sty))
story.append(Spacer(1, 0.3*cm))
# 4 hemorrhage images in 2x2 grid
hem_imgs = [
(paths["ich"], "ICH – Round hyperdense mass\nIN brain parenchyma\nHypertensive bleed (putamen)"),
(paths["edh"], "EDH – Biconvex lens shape\nBETWEEN skull & dura\nArterial (middle meningeal a.)"),
(paths["sdh"], "SDH – Crescent shape\nOver brain convexity\nVenous (bridging veins)"),
(paths["sah"], "SAH – Fills cisterns & sulci\nIN subarachnoid space\nAneurysm rupture"),
]
cell_w = PW / 2 - 0.5*cm
cell_h = 8.5*cm
grid_data = [[],[]]
for i, (p, cap) in enumerate(hem_imgs):
cell = [img_flowable(p, cell_w, cell_h - 1.2*cm),
Paragraph(cap, small_sty)]
grid_data[i//2].append(cell)
# Flatten for table
t_data = []
for row in grid_data:
t_data.append(row)
grid = Table(t_data, colWidths=[cell_w, cell_w])
grid.setStyle(TableStyle([
('ALIGN', (0,0),(-1,-1),'CENTER'),
('VALIGN', (0,0),(-1,-1),'TOP'),
('GRID', (0,0),(-1,-1), 1, colors.HexColor('#334455')),
('BACKGROUND',(0,0),(-1,-1), colors.HexColor('#05050F')),
('TOPPADDING',(0,0),(-1,-1),4),
('BOTTOMPADDING',(0,0),(-1,-1),4),
]))
story.append(grid)
story.append(PageBreak())
# ── SAH BASILAR – separate page ───────────────────────────────────────────────
story.append(Paragraph("EXTRA: SAH from Basilar Artery Aneurysm + Hydrocephalus", sec_sty))
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor('#FF8C00'), spaceAfter=6))
story.append(Paragraph(
"Basilar artery aneurysm rupture fills the <b>basal cisterns</b> and can cause <b>intraventricular hemorrhage (IVH)</b> "
"and <b>acute hydrocephalus</b> (enlarged temporal horns). Life-threatening emergency.",
body_sty))
story.append(Spacer(1, 0.2*cm))
story.append(img_flowable(paths["sah_basilar"], PW * 0.55, 11*cm))
story.append(Spacer(1, 0.3*cm))
story.append(make_table(
["Finding on CT", "Meaning", "Why it happens"],
[
["Blood in basal cisterns", "SAH – subarachnoid hemorrhage", "Blood fills CSF space around brainstem"],
["Hyperdense 3rd ventricle", "Intraventricular hemorrhage (IVH)", "Blood enters via foramen of Monro"],
["Enlarged temporal horns", "ACUTE HYDROCEPHALUS", "Blood blocks arachnoid granulations → CSF backup"],
["Blood-CSF level in vent.", "Hematocrit effect", "Dense blood sinks below lighter CSF"],
]
))
story.append(PageBreak())
# ── ISCHEMIC INFARCT ──────────────────────────────────────────────────────────
story.append(Paragraph("SECTION 2: ISCHEMIC STROKE / INFARCT – 'Dark Wedge = Dead Brain'", sec_sty))
story.append(HRFlowable(width="100%", thickness=1, color=CYAN_C, spaceAfter=6))
story.append(Paragraph(
"Ischemic stroke appears <b>HYPODENSE (dark)</b> because dead neurons swell with water. "
"Key: the hypodensity follows a <b>VASCULAR TERRITORY</b> (wedge-shaped), not random. "
"First 3-6 hours CT may be <b>completely normal</b> – this does NOT exclude stroke!",
body_sty))
story.append(Spacer(1, 0.2*cm))
infarct_time_table = make_table(
["Time Since Stroke", "CT Appearance", "What You See", "Action"],
[
["0 – 3 hours\n(Hyperacute)", "NORMAL or subtle", "Loss of gray-white diff.\nInsular ribbon sign\nHyperdense MCA sign", "Give tPA if eligible!\nCT normal ≠ no stroke"],
["3 – 6 hours\n(Early acute)", "Subtle HYPODENSITY", "Faint dark area in\ncortex/basal ganglia", "Still tPA window\nConsider thrombectomy"],
["6 – 24 hours\n(Acute)", "Clear HYPODENSITY", "Wedge dark area\nSulcal effacement\nMass effect", "Thrombectomy if LVO\nAntiplatelets/anticoag"],
["1 – 7 days\n(Subacute)", "Dense hypodensity\n+ mass effect", "Max swelling, midline\nshift if large\n'Fogging' = isodense", "Monitor for herniation\nHemicraniectomy if needed"],
["> 3 weeks\n(Chronic)", "VERY HYPODENSE\n(CSF-like)", "Encephalomalacia\nEx vacuo ventricle\nwidened sulci", "Rehab, secondary\nprevention"],
]
)
story.append(infarct_time_table)
story.append(Spacer(1, 0.3*cm))
story.append(img_flowable(paths["infarct"], PW * 0.5, 10*cm))
story.append(PageBreak())
# ── KEY DIFFERENTIATORS ────────────────────────────────────────────────────────
story.append(Paragraph("SECTION 3: HOW TO TELL THEM APART – Quick Differentiator", sec_sty))
story.append(HRFlowable(width="100%", thickness=1, color=GRN_C, spaceAfter=6))
diff_table = make_table(
["Question to Ask", "Hemorrhage", "Infarct", "Tumor"],
[
["What color?", "WHITE (hyperdense)", "DARK (hypodense)", "Variable (mixed/ring)"],
["What shape?", "Round / crescent / fills\ncisterns (depends on type)", "WEDGE following\nvascular territory", "Round, irregular –\nNOT vascular pattern"],
["Is it in the cortex only?", "No – all layers involved", "Yes (cortex + white matter)", "May spare cortex early"],
["Any surrounding edema?", "Rim of dark edema in\ndays 2-3", "IS the edema", "Prominent\nfinger-like vasogenic edema"],
["Midline shift?", "Yes if large", "Yes if large + swollen", "Yes if large"],
["Ring enhancement\n(with contrast)?", "No", "No (except subacute gyral)", "YES – irregular ring\n= GBM / mets / abscess"],
["Fits vascular territory?", "No (except\nhemorrhagic infarct)", "YES – always", "No – random location"],
["Onset?", "Sudden (seconds)", "Sudden (seconds-minutes)", "Gradual (days-weeks)"],
["Fever?", "No", "No", "Possible if abscess"],
]
)
story.append(diff_table)
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph("<b>The 3 Golden Questions when you see an abnormality on CT:</b>", body_sty))
q_table = make_table(
["Question", "Answer → Diagnosis"],
[
["Is it WHITE (hyperdense)?", "→ Think BLOOD (hemorrhage of any type)"],
["Is it DARK (hypodense)?", "→ Think INFARCT (if wedge/vascular) or TUMOR EDEMA (if finger-like)"],
["Does it have a ring on contrast?", "→ Think GBM, metastasis, or brain abscess"],
],
col_widths=[PW*0.38, PW*0.58]
)
story.append(q_table)
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph(
"Sources: Frameworks for Internal Medicine | Adams & Victor's Neurology 12e | "
"Plum & Posner's Stupor and Coma | Bailey & Love's Surgery 28e | "
"Radiologymasterclass.co.uk | PMC CT Imaging in Neurocritical Care",
small_sty))
doc.build(story)
print(f"\nPDF saved: {PDF}")
cd /home/daytona/workspace/ct-brain-atlas && python3 build_pathology_atlas.py 2>&1
ls -lh /home/daytona/workspace/ct-brain-atlas/CT_Brain_Pathology_Atlas.pdf && ls -lh /home/daytona/workspace/ct-brain-atlas/pathology_out/
🧠 CT Brain Pathology Comparison Atlas - Complete
Download the Full PDF (5 pages, landscape, dark theme):
CT Brain Pathology Atlas
PDF Document · PDF
Individual Annotated Real CT Films:
🔴 HEMORRHAGE — "White = Blood"
ich annotated
Image · JPG
edh annotated
Image · JPG
sdh annotated
Image · JPG
sah annotated
Image · JPG
sah basilar annotated
Image · JPG
🔵 ISCHEMIC STROKE — "Dark Wedge = Dead Brain"
mca infarct annotated
Image · JPG
The 3 Golden Questions (Memorise These)
| Question | Answer |
|---|---|
| Is it WHITE? | → BLOOD (ICH = in brain, EDH = biconvex, SDH = crescent, SAH = fills cisterns) |
| Is it DARK + wedge-shaped? | → ISCHEMIC INFARCT (follows vascular territory) |
| Ring on contrast CT? | → TUMOR (GBM/mets = thick irregular ring) or ABSCESS (thin smooth ring) |
Shape = Diagnosis (One-Liner Rule)
| Shape | = Diagnosis |
|---|---|
| Round white blob IN brain | = ICH |
| Biconvex (lens) white at skull edge | = EDH (arterial, lucid interval) |
| Crescent white over convexity | = SDH (venous, crosses sutures) |
| White filling sulci/cisterns | = SAH (aneurysm until proven otherwise) |
| Dark wedge in vascular territory | = Ischemic stroke |
| Dark area + finger-like extensions | = Tumor with vasogenic edema |
| Dark core + bright ring + contrast | = GBM or abscess |
Generate a clinical decision tree: 'How to read a head CT in 60 seconds'
ls /home/daytona/workspace/ct-brain-atlas/ && python3 -c "import PIL, reportlab; print('deps OK')"
teach me in easy way multiple myeloma consultant level and at the end of discussion arrange mcqs for better understanding
Multiple Myeloma - Consultant-Level Teaching Guide
The Big Picture First
1. Pathogenesis
- Rearrangements of IGH locus on chromosome 14q32 with various oncogenes (cyclin D1, cyclin D3)
- NF-κB pathway mutations - support B cell survival
- IL-6 is the critical growth/survival cytokine (produced by tumor cells AND stromal cells; high serum IL-6 = poor prognosis)
- MIP-1α (CCL3) from myeloma cells drives osteoclast activation
- Wnt pathway inhibitors from tumor cells suppress osteoblasts
- Result: massive osteolysis - osteoclasts up, osteoblasts down → bone pain, fractures, hypercalcemia
MGUS (monoclonal gammopathy of undetermined significance)
↓ ~1%/year progress
Smoldering MM (asymptomatic)
↓ ~10%/year progress
Symptomatic MM (active myeloma - treat!)
- Robbins & Kumar Basic Pathology / Robbins, Cotran & Kumar Pathologic Basis of Disease
2. Morphology - What You See Under the Microscope
Bone Marrow Aspirate: Neoplastic Plasma Cells
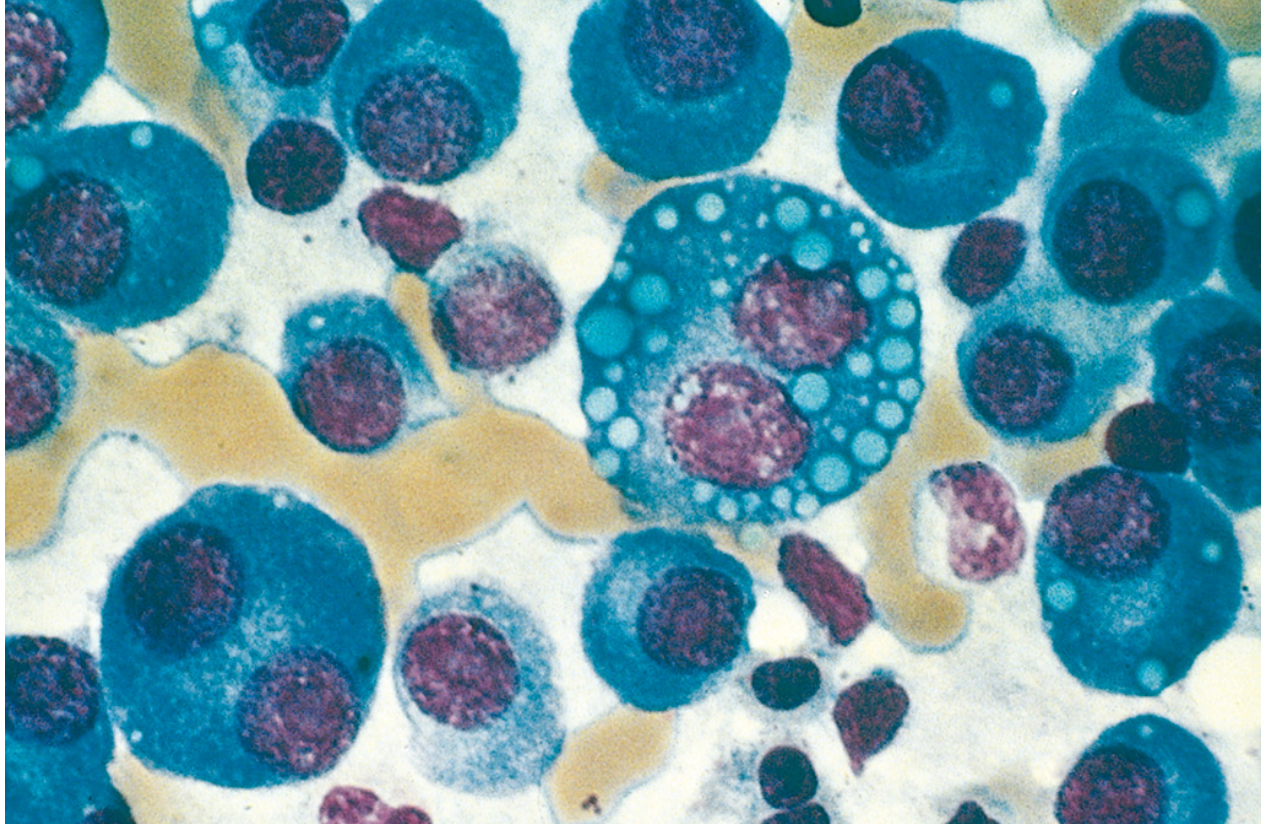
| Variant | Description |
|---|---|
| Typical | Eccentric nucleus, perinuclear clearing (Golgi), "clock-face" chromatin |
| Plasmablast | Vesicular chromatin, single prominent nucleolus - aggressive |
| Flame cell | Fiery red cytoplasm |
| Mott cell | Multiple "grape-like" cytoplasmic droplets (Russell bodies) |
| Russell bodies | Cytoplasmic Ig globules |
| Dutcher bodies | Nuclear Ig inclusions |
3. The Spectrum of Plasma Cell Disorders
| Condition | Plasma Cells in BM | M Protein | Symptoms | Action |
|---|---|---|---|---|
| MGUS | <10% | IgG/A/M <30g/L or urine <500mg/24h | None | Watch: 1%/year → MM |
| Smoldering MM | 10-30% | IgG/A ≥30g/L or urine ≥500mg/24h | None (no CRAB) | Watch or trial |
| Symptomatic MM | ≥10% or plasmacytoma | Present (or nonsecretory) | CRAB / SLiM | Treat now |
| Solitary plasmacytoma | Normal BM | Usually none | Single bone/soft tissue lesion | Radiotherapy |
| Plasma cell leukemia | >20% circulating PCs | Present | Aggressive | Treat urgently |
| POEMS syndrome | Present | VEGF elevated | Polyneuropathy, organomegaly, endocrinopathy, M-protein, skin | Complex Rx |
4. Diagnostic Criteria (IMWG 2014)
CRAB = End-organ Damage (Classic Myeloma-Defining Events)
| Letter | Criterion | Threshold |
|---|---|---|
| C - Hypercalcemia | Ca >0.25 mmol/L above ULN | or >2.75 mmol/L (>11 mg/dL) |
| R - Renal insufficiency | CrCl <40 mL/min | or creatinine >177 μmol/L (>2 mg/dL) |
| A - Anemia | Hb >20g/L below LLN | or Hb <100 g/L |
| B - Bone lesions | ≥1 osteolytic lesion | on X-ray, CT, or PET-CT |
SLiM = Biomarkers of Malignancy (Even WITHOUT CRAB - these still define symptomatic MM)
| Letter | Criterion | Value |
|---|---|---|
| Sixty | Clonal BM plasma cells | ≥60% |
| Light chains | Involved:uninvolved FLC ratio | ≥100 |
| MRI | Focal lesions on MRI | >1 focal lesion |
Key teaching point: A patient with ≥60% plasma cells in the marrow but NO CRAB = still symptomatic myeloma and needs treatment - this is the SLiM criteria update (IMWG 2014).
- Harrison's Principles of Internal Medicine 22E (2025)
5. Clinical Features
The Five Clinical Pillars:
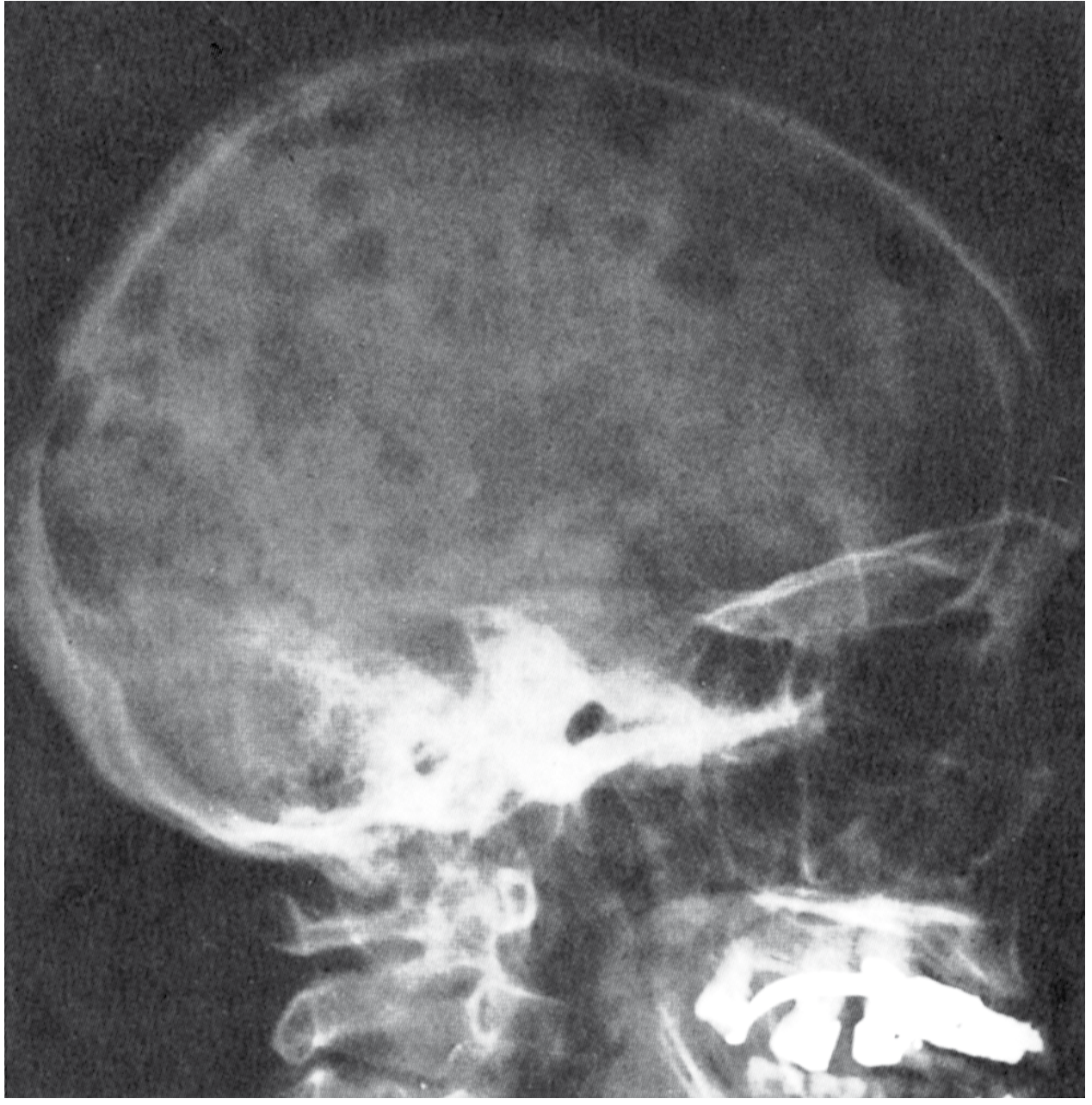
- Pathologic fractures (vertebrae most common → spinal cord compression)
- Bone pain (lower back most frequent complaint)
- Note: ALP is NORMAL or only mildly elevated (osteoblasts suppressed - no new bone formed around lesions)
- PET-CT or whole-body MRI now preferred over plain skeletal survey
- Most important: Bence Jones protein toxicity to tubular epithelium → cast nephropathy ("myeloma kidney")
- Light chain λ types prone to AL amyloidosis
- Other mechanisms: hypercalcemia (nephrocalcinosis), hyperuricemia, NSAIDs/contrast nephrotoxicity, hyperviscosity
- 30-day mortality if on dialysis ≈ 50% without treatment
- Marrow infiltration → reduced erythropoiesis
- Cytokine suppression (IL-1β, TNF)
- Haemolysis, renal EPO deficiency
- Most common presenting symptom (fatigue, dyspnoea)
- Hypogammaglobulinaemia - myeloma cells suppress normal B-cell Ig production
- Predominantly bacterial (Streptococcus pneumoniae, Haemophilus influenzae)
- Cellular immunity relatively preserved
- Leading cause of death alongside renal failure
- Vaccinations and prophylactic IVIG in selected patients
- From osteoclast-mediated bone resorption
- Symptoms: "Bones, groans, stones, psychic moans" - confusion, constipation, polyuria, weakness, renal stones
- Treat: IV fluids + bisphosphonates ± calcitonin acutely
Other Important Complications:
- Hyperviscosity syndrome (more with IgA, IgM) - headache, visual disturbance, bleeding
- AL amyloidosis - restrictive cardiomyopathy, macroglossia, nephrotic syndrome
- Spinal cord compression - oncological emergency
- Coagulopathy - M protein interferes with clotting factors
6. Investigations - The Consultant's Workup
Confirming the Diagnosis:
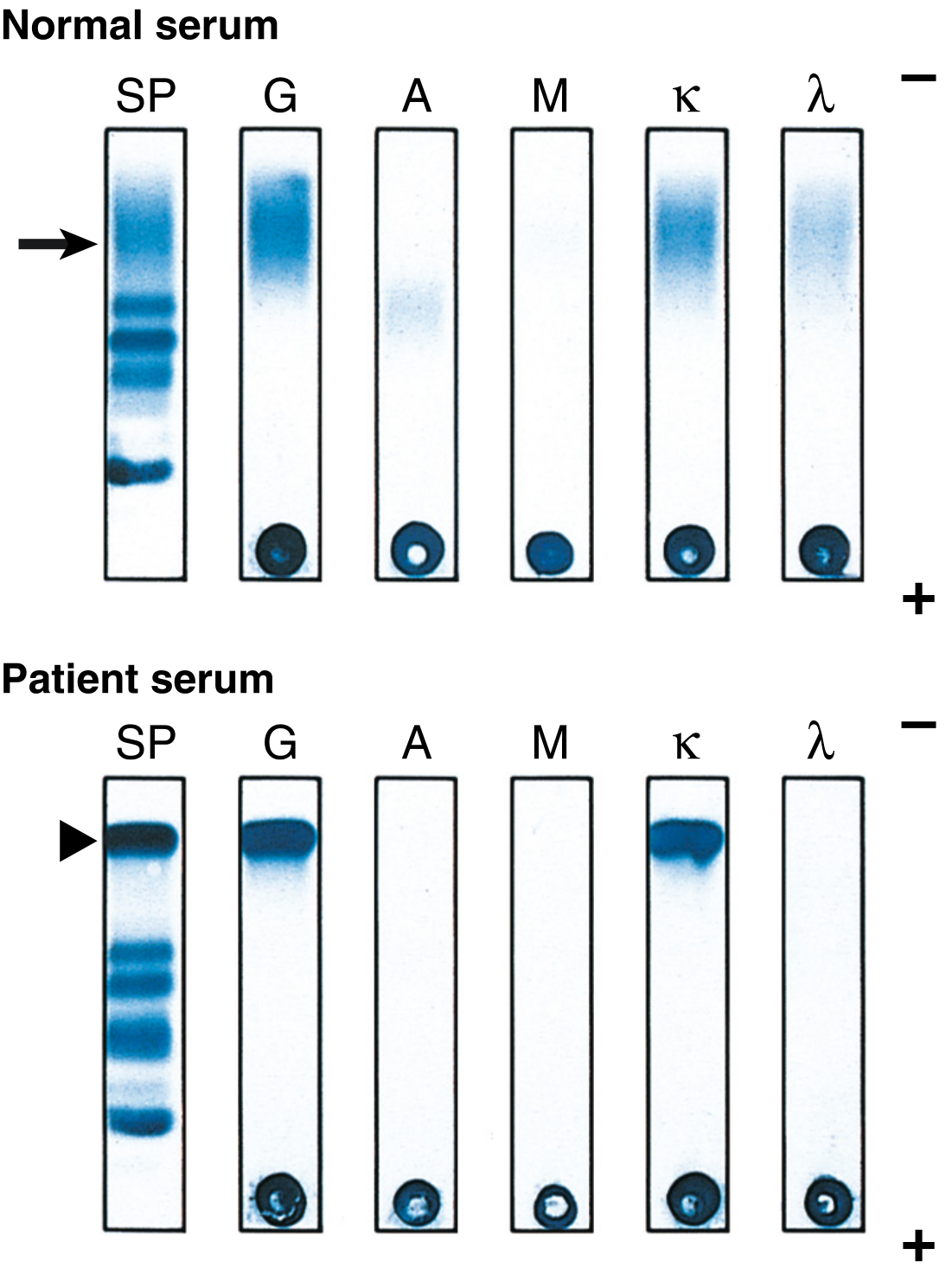
| Test | Finding | What It Means |
|---|---|---|
| SPEP | M-spike in gamma region | Monoclonal protein - proceed to immunofixation |
| Serum immunofixation | Confirms class (IgG/A/M/D/E) + light chain (κ or λ) | IgG most common (~55%), IgA (~20%) |
| Serum free light chains | Κ or λ, ratio (normally 0.26-1.65) | High ratio = light chain restricted, ratio ≥100 = SLiM criteria |
| Urine SPEP + immunofixation (24h) | Bence Jones protein | Free light chains excreted in urine |
| Bone marrow biopsy/aspirate | Plasma cell % (≥10%), clonality | Gold standard for diagnosis |
For Risk Stratification (ISS/R-ISS Staging):
| Stage | β2-Microglobulin | Albumin | Median OS |
|---|---|---|---|
| I | <3.5 mg/L | ≥35 g/L | 62 months |
| II | Neither I nor III | - | 44 months |
| III | ≥5.5 mg/L | - | 29 months |
- High-risk FISH cytogenetics: del(17p), t(4;14), t(14;16), t(14;20) → worse prognosis
- Elevated LDH → R-ISS Stage III
- del(17p) → TP53 loss → most aggressive
- t(4;14) → FGFR3/MMSET overexpression
- t(14;16) → MAF overexpression
- t(14;20) → MAFB overexpression
- amp(1q) → CKS1B amplification
- del(1p) → additional risk
Note: Chromosome 13q deletion and t(11;14) alone do NOT predict high-risk disease.
Full Investigations Summary (Harrison's 22E):
7. Management
Management Flowchart from Goldman-Cecil Medicine:
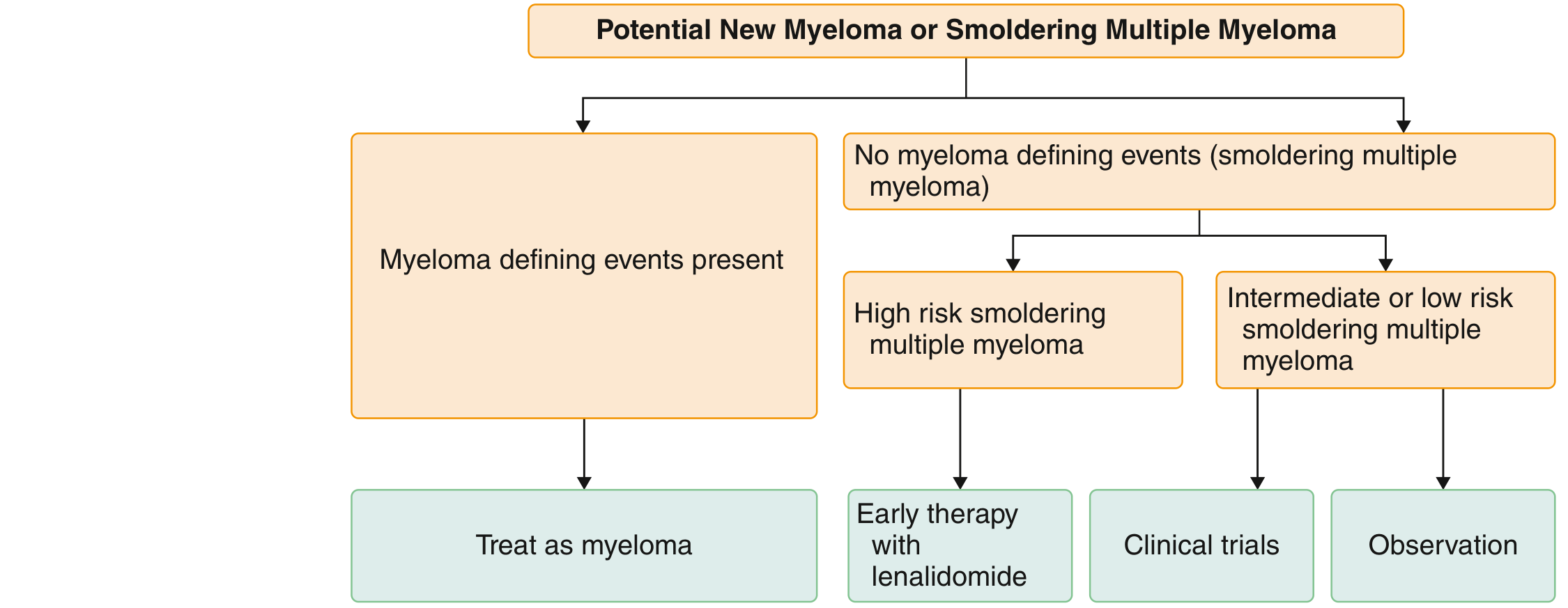
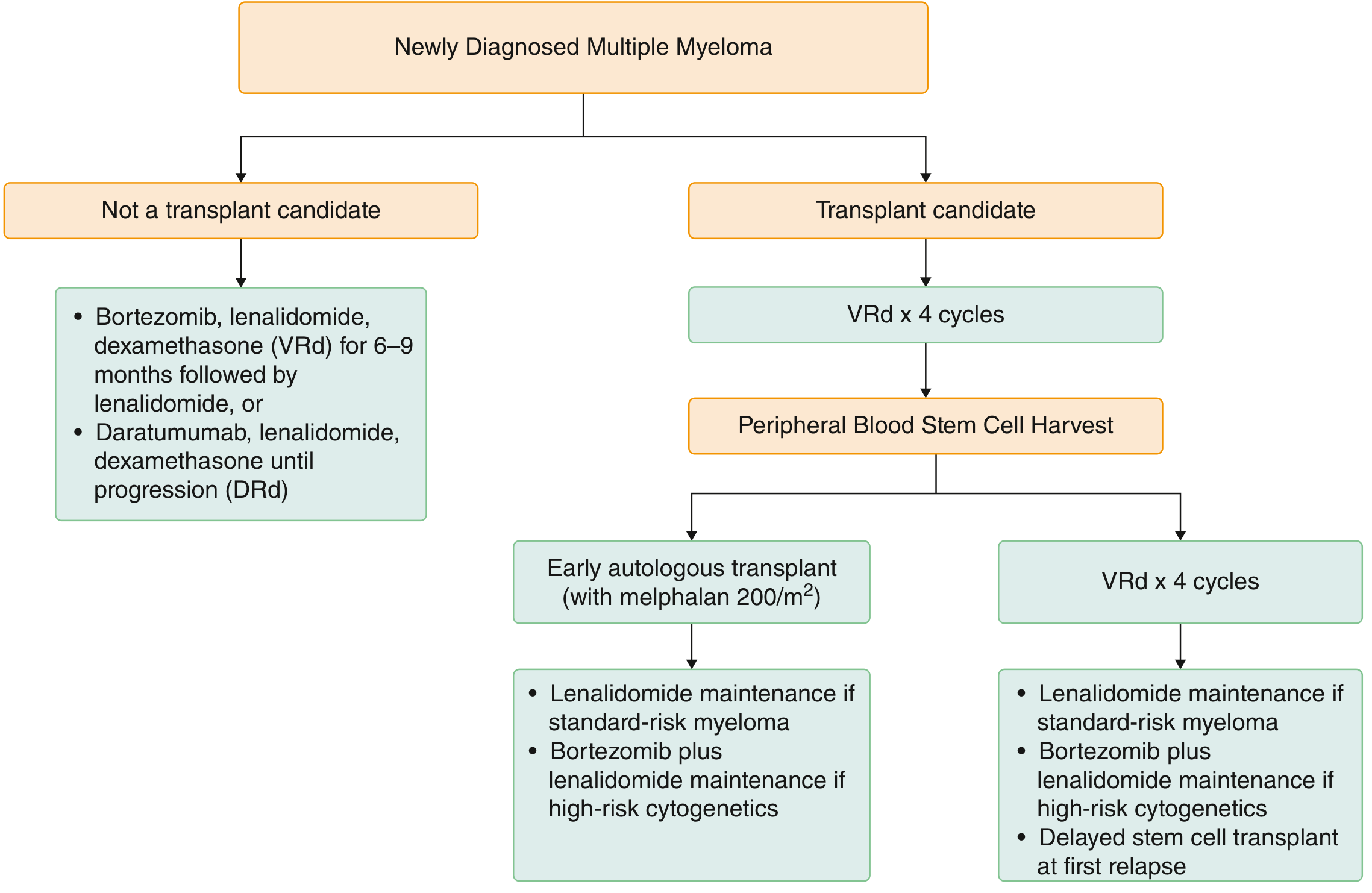
Key Drug Classes:
| Class | Agent | Mechanism | Key Toxicity |
|---|---|---|---|
| Proteasome inhibitor (PI) | Bortezomib (V) | Blocks 26S proteasome → unfolded protein accumulation → apoptosis | Peripheral neuropathy, thrombocytopenia |
| PI (2nd gen) | Carfilzomib (K) | Irreversible PI - more potent | Cardiotoxicity, hypertension |
| PI (oral) | Ixazomib | Oral PI | Nausea, diarrhoea |
| IMiD | Lenalidomide (R) | Cereblon binding → Ikaros/Aiolos degradation → anti-MM effect | DVT! (give prophylactic aspirin/anticoag), myelosuppression |
| IMiD | Thalidomide | Older agent, more neuropathy | Neuropathy, DVT, teratogenesis |
| IMiD (3rd gen) | Pomalidomide | Used in relapsed/refractory | Cytopenias |
| Anti-CD38 Ab | Daratumumab (D) | CD38 is highly expressed on plasma cells | Infusion reactions (premedicate), infections |
| Anti-SLAMF7 Ab | Elotuzumab | Immune-activating via NK cells | Infusion reactions |
| Alkylating agent | Melphalan | DNA cross-linking | Myelosuppression |
| Corticosteroid | Dexamethasone | Anti-myeloma + anti-inflammatory | Hyperglycaemia, Cushingoid features |
| BCL-2 inhibitor | Venetoclax | For t(11;14) patients specifically | Tumour lysis syndrome |
| BCMA-targeted | Teclistamab, Carvykti (CAR-T) | Bispecific T-cell engager / CAR-T | CRS, neurotoxicity |
Standard Regimens (Goldman-Cecil):
- Induction: VRd (bortezomib + lenalidomide + dexamethasone) × 3-4 cycles
- OR Daratumumab-VRd (DaraVRd) for high-risk
- Stem cell mobilisation: G-CSF ± plerixafor (or cyclophosphamide)
- Conditioning: Melphalan 200 mg/m²
- Autologous SCT (ASCT) - mortality <1%
- Maintenance: Lenalidomide (standard-risk) | Bortezomib + lenalidomide (high-risk cytogenetics)
- VRd × 6-9 months then lenalidomide maintenance
- OR DRd (Daratumumab-lenalidomide-dexamethasone) until progression
- Add carfilzomib or pomalidomide or daratumumab to backbone
- CAR-T (Carvykti/Abecma) for heavily pre-treated patients
- Bispecific antibodies (teclistamab) targeting BCMA
Allogenic SCT is rarely used - high treatment-related mortality; reserved for very young high-risk patients on clinical trials.
Supporting Therapies (Never Forget):
| Complication | Treatment |
|---|---|
| Bone disease | Bisphosphonates (zoledronic acid) for all with bone involvement; RANKL inhibitor (denosumab) if renal failure |
| Spinal cord compression | Dexamethasone immediately + urgent radiotherapy/surgery |
| Hypercalcaemia | IV saline + bisphosphonates ± calcitonin |
| Renal failure | Hydration; avoid nephrotoxins; bortezomib-based Rx (not renal dose-adjusted); dialysis if severe |
| Anaemia | EPO agents; blood transfusions |
| Infections | Prophylactic acyclovir (with bortezomib), IVIG if recurrent serious infections; pneumococcal/influenza vaccines |
| DVT (with IMiDs) | Aspirin or LMWH depending on risk |
| Hyperviscosity | Plasmapheresis |
8. Prognosis
- Median OS with modern therapy: 7-10+ years for standard-risk; <3-4 years for high-risk cytogenetics
- β2-microglobulin = single most powerful predictor of survival
- MRD (minimal residual disease) negativity = strongly associated with better survival but does not currently change therapy outside trials
- Cure is not achieved with current therapy - disease is controlled, not eliminated
- Death most commonly from: infection > renal failure > disease progression
9. Rouleaux Formation on Blood Film
Rouleaux formation is characteristic but NOT specific - also seen in lupus, early HIV, other hypergammaglobulinaemia states.
10. POEMS Syndrome (High-Yield Variant)
- Polyneuropathy (mandatory)
- Monoclonal plasma cell disorder (mandatory)
- One of: sclerotic bone lesions / Castleman's disease / elevated VEGF
- One minor: organomegaly, endocrinopathy, skin changes (hyperpigmentation), papilledema, extravascular fluid, thrombocytosis
📝 MCQs - Multiple Myeloma (Consultant Level)
- A) His haemoglobin is below 100 g/L (anemia criterion)
- B) His bone marrow plasma cells exceed 10%
- C) He meets CRAB criteria for myeloma-defining events
- D) His ESR is elevated above normal
- E) He has a high-burden M-spike on SPEP
Answer
- A) Trisomy of odd-numbered chromosomes (hyperdiploidy)
- B) t(11;14)
- C) del(13q)
- D) del(17p) / TP53 mutation
- E) t(4;14)
Answer
- A) CHOP chemotherapy
- B) Melphalan + prednisone alone
- C) Bortezomib + lenalidomide + dexamethasone (VRd) OR Daratumumab + lenalidomide + dexamethasone (DRd)
- D) High-dose melphalan 200 mg/m² alone
- E) Thalidomide monotherapy
Answer
- A) ALP is produced only by hepatocytes, not osteoblasts
- B) Myeloma cells secrete inhibitors of osteoclast activity
- C) Wnt pathway inhibitors from myeloma cells suppress osteoblast activity, resulting in little new bone formation
- D) Bence Jones protein directly inhibits ALP enzyme activity
- E) Lytic lesions are too small to stimulate osteoblasts
Answer
- A) Lenalidomide-induced DVT - start anticoagulation
- B) Bortezomib-induced peripheral neuropathy - consider dose reduction or switch to subcutaneous administration
- C) Dexamethasone-induced myopathy - reduce dexamethasone
- D) AL amyloidosis neuropathy - stop all therapy
- E) Hypercalcaemia-related neurological effect - treat hypercalcaemia
Answer
- A) Lenalidomide at full dose (25 mg daily)
- B) Bortezomib-based regimen (dose not significantly adjusted for renal impairment)
- C) Carfilzomib at standard dosing
- D) Melphalan at full dose
- E) Thalidomide as monotherapy
Answer
- A) Symptomatic multiple myeloma - start VRd immediately
- B) MGUS - observe annually, no treatment
- C) Smoldering multiple myeloma - risk-stratify; low/intermediate risk = observe, high risk = consider lenalidomide
- D) Plasma cell leukaemia - urgent treatment
- E) Solitary plasmacytoma - radiotherapy
Answer
- A) It is based on serum M-protein level and percentage of plasma cells
- B) β2-microglobulin is the single most powerful predictor of survival
- C) The Durie-Salmon staging system is now preferred over ISS for guiding therapy
- D) LDH level forms the basis of the original ISS (not R-ISS)
- E) ISS Stage I has a median OS of approximately 20 months
Answer
- A) Intact monoclonal IgG secreted directly into urine
- B) Free monoclonal light chains (κ or λ) that pass the glomerular filter due to their small size
- C) Albumin fragments degraded by myeloma cells
- D) β2-microglobulin shed from plasma cell surface
- E) Denatured IgA M-protein that precipitates in the cold
Answer
- A) Carfilzomib-induced pulmonary hypertension - avoid carfilzomib
- B) Lenalidomide-induced deep vein thrombosis / pulmonary embolism - prophylactic aspirin or anticoagulation should have been prescribed
- C) Bortezomib-induced peripheral neuropathy affecting the leg - physiotherapy
- D) Hypercalcaemia-induced venous stasis - treat hypercalcaemia
- E) AL amyloidosis causing restrictive cardiomyopathy
Answer
- A) Hypercalcaemia
- B) Cardiac amyloidosis
- C) Infection (bacterial)
- D) Hepatic failure from amyloid
- E) Haemorrhagic stroke
Answer
- A) Emergency bone marrow biopsy to check plasma cell percentage
- B) Immediate high-dose intravenous dexamethasone + urgent MRI spine + neurosurgical/radiotherapy consultation
- C) Start bortezomib-based chemotherapy and monitor
- D) Bisphosphonate therapy and physiotherapy
- E) Plasmapheresis for hyperviscosity
Answer
- 12/12 = Consultant material
- 9-11 = Registrar level
- 6-8 = Senior house officer level
- <6 = Review the guide and retry!
teach me diabetes mellitus briefly with types and with complications specially focu on diabetic foot thier examination investigation and management with classfifcation get materal from harrison and more other books if relevant make it precise detailed and relavant
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.13.content.30.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.