Role of core needle biopsy in the breast pathology
Reading File
Finding Sources
Searching PubMed
"core needle biopsy" AND "breast" AND pathology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks to write a thorough answer. Let me compile everything.
Role of Core Needle Biopsy in Breast Pathology
1. Overview and Why CNB is Preferred
Core needle biopsy (CNB) is the preferred standard of care for pathologic diagnosis of breast lesions, recommended by both the NCCN and the American Society of Breast Surgeons. It has largely replaced surgical excisional biopsy for purely diagnostic purposes because it is:
- Less invasive and less expensive than excisional biopsy
- Performed under local anaesthesia as an outpatient procedure
- Able to preserve tissue architecture - enabling histological (not just cytological) diagnosis
- Able to discriminate between invasive and non-invasive breast cancer (a distinction FNA cannot reliably make)
- Capable of providing sufficient material for ancillary biomarker testing (ER, PR, HER2, Ki-67)
As summarized in Mulholland and Greenfield's Surgery, "Core needle biopsy is the preferred strategy for breast cancer diagnosis. Core needle biopsy is less invasive and less expensive than excisional biopsy and facilitates definitive breast cancer treatment planning."
2. CNB vs Fine-Needle Aspiration (FNA)
| Feature | FNA | Core Needle Biopsy |
|---|---|---|
| Needle gauge | 21-25G | 14G (breast), 18G (axillary nodes) |
| Tissue obtained | Cells only (cytology) | Tissue cores (histology) |
| Architecture assessed | No | Yes |
| Invasive vs. in situ distinction | Cannot reliably distinguish | Yes |
| Biomarker testing (ER/PR/HER2) | Limited | Reliable |
| False-negative rate | Higher | Very low |
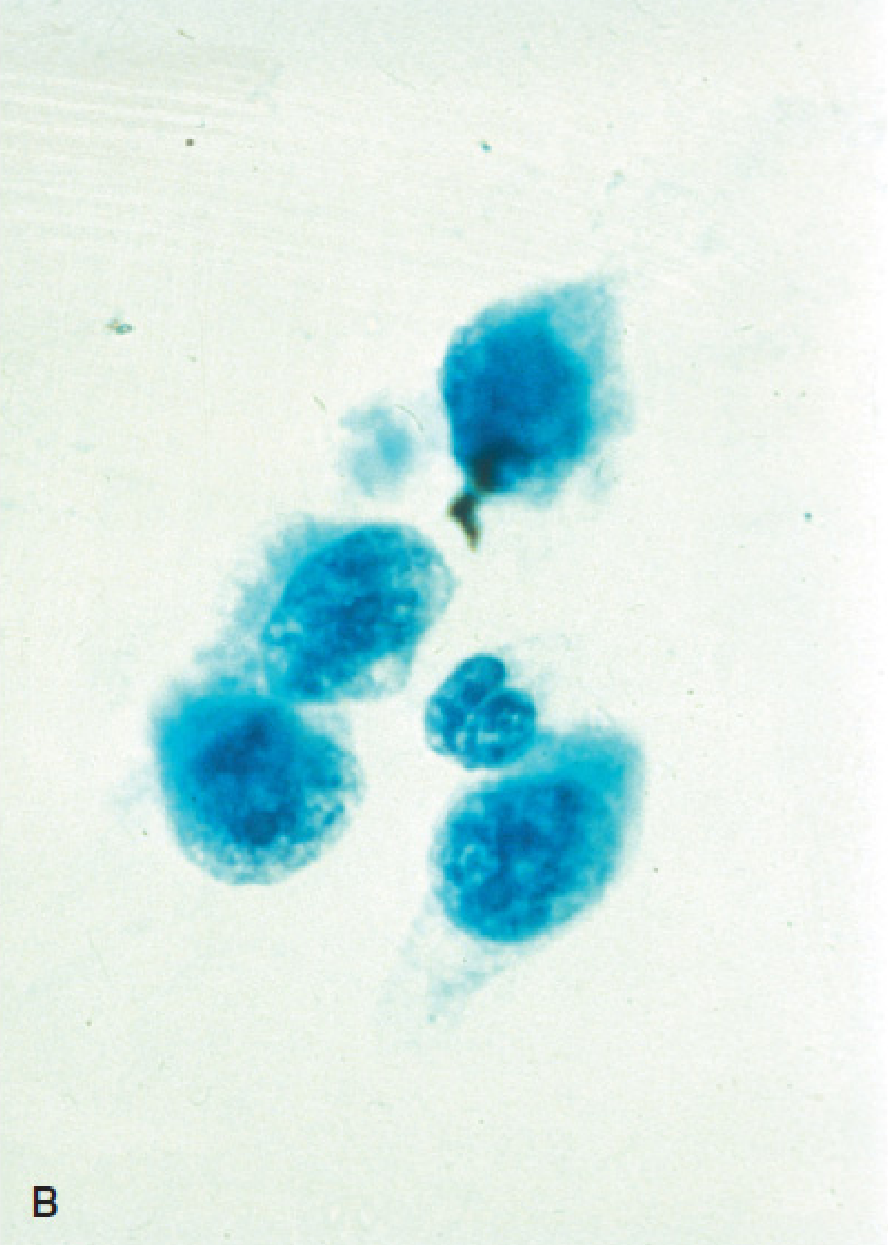
FNA of the breast has reported sensitivity 98% and specificity 97% in experienced centers, but because tissue architecture cannot be evaluated, a definitive diagnosis of invasive cancer cannot be made by FNA alone. High-suspicion lesions must be sampled by CNB.
Figure: FNA specimen (Panel B) showing isolated malignant cells - architecture is lost (from Mulholland and Greenfield's Surgery)
3. Technical Aspects of CNB
Needle Size and Device
- Standard CNB uses 14-gauge needles for breast tissue and 18-gauge for axillary lymph nodes
- Spring-loaded automated devices are standard
- Vacuum-assisted biopsy (VAB) uses 7-12 gauge needles (9G most popular), allowing multiple samples (up to 12) with a single insertion, rotating 360° around the lesion
Image Guidance - Always Required
CNB should always be performed under image guidance. Three modalities are used:
- Ultrasound-guided CNB - first choice for most breast lesions; avoids radiation, real-time needle visualization; used for palpable and non-palpable masses
- Stereotactic (mammography-guided) CNB - used for non-palpable lesions visible only on mammogram, especially microcalcifications. Uses triangulation to localize the lesion in 3D. Patient is prone on a dedicated table.
- MRI-guided CNB - reserved for lesions visible only on MRI
Freehand CNB (without imaging) should be reserved for rare cases with no imaging correlate. The needle tip should sample only the solid part of the lesion, avoiding cystic areas and blood vessels.
Specimen Imaging
When stereotactic biopsy is performed for microcalcifications, the cores must be specimen-imaged to confirm the presence of calcifications within the biopsy sample.
4. Role in Diagnosis of Specific Breast Lesions
The CNB result determines management across the full spectrum of breast pathology:
Benign/Non-Proliferative Lesions (No increased cancer risk)
- Usual ductal hyperplasia (UDH), simple cysts, fibroadenoma
- CNB establishes the benign diagnosis; if concordant with imaging, no surgical excision needed
- Return to routine surveillance
Proliferative Disease Without Atypia (~2x relative risk)
- Moderate/florid ductal hyperplasia, sclerosing adenosis, radial scar, solitary papilloma, papillomatosis
- CNB establishes the diagnosis; management depends on radiologic-pathologic concordance
- Radial scar on CNB: surgical excision recommended due to upgrade risk
High-Risk (Atypical) Lesions (>2x relative risk - Upgrade Risk on Excision)
These are the most important CNB findings guiding surgical decision-making:
| Lesion | CNB Finding | Action |
|---|---|---|
| Atypical ductal hyperplasia (ADH) | Upgrade rate 5-25% to carcinoma | Surgical excision indicated |
| Atypical lobular hyperplasia (ALH) | Upgrade to malignancy | Excision usually recommended |
| Lobular carcinoma in situ (LCIS) | Upgrade to invasive Ca: <5% if concordant | Excision no longer mandatory if radiologic-pathologic concordance; multidisciplinary review |
| Flat epithelial atypia (FEA) | Low-moderate upgrade risk | Multidisciplinary review |
| Papillary lesions | Variable upgrade risk | Excision recommended |
| Columnar cell hyperplasia with atypia | Variable | Excision recommended |
Key point: "The upgrade of lobular neoplasia diagnosed on core biopsy at time of surgical excision to malignancy is 1% to 3% and as such surgical excisional biopsy is no longer indicated if there is radiographic-pathologic concordance." - Mulholland and Greenfield's Surgery
Malignant Lesions
CNB enables:
- Definitive diagnosis of invasive vs. in situ carcinoma (DCIS)
- Histological grade (Nottingham grading)
- Biomarker assessment: ER, PR, HER2 (IHC ± FISH), and Ki-67 proliferation index
- Molecular subtyping guiding neoadjuvant vs. adjuvant therapy decisions
Per Harrison's Principles of Internal Medicine (2025): "Final diagnosis rests on pathologic confirmation, which is generally carried out by image-guided core biopsy to confirm diagnosis, assess tumor grade and morphology, and carry out biomarker evaluation for expression of estrogen receptor (ER) and progesterone receptor (PR) and HER2 proteins and potentially HER2 gene amplification."
5. Radiologic-Pathologic Concordance
After a benign result on CNB, the radiologist issues a concordance statement - assessing whether the clinical and imaging findings are consistent with the histologic diagnosis.
- Concordant result: imaging differential matches pathology - patient can return to surveillance or proceed per risk category
- Discordant result (e.g., BI-RADS 5 lesion with benign histology): concern that the target was missed or undersampled; surgical excision is mandatory
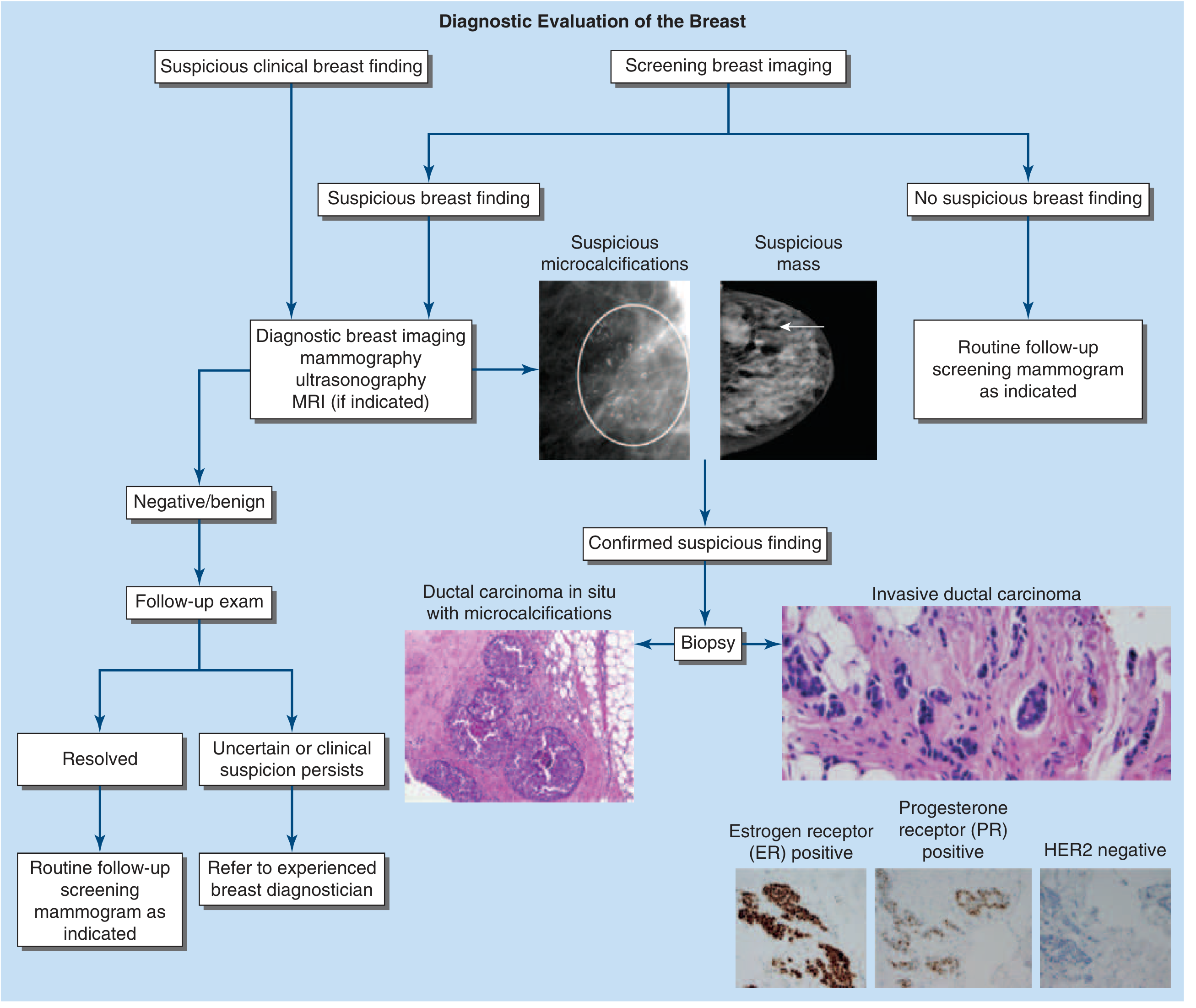
Diagnostic Evaluation of the Breast: Biopsy leads to histology (DCIS or invasive carcinoma) and receptor profiling (ER, PR, HER2) - Harrison's Principles of Internal Medicine 2025
6. Vacuum-Assisted Biopsy (VAB) - Enhanced CNB
VAB uses negative pressure to pull tissue into the collecting aperture, excising it with a rotating cutter. Advantages over standard CNB:
- Larger tissue volume per pass (9G device removes up to ~1 cm of tissue)
- Multiple harvests in 360° with single insertion
- Significantly lower false-negative rate for microcalcifications: repeat biopsy rate 11.6% vs 23.7% for standard CNB
- Superior for DCIS: only 6% upgraded to invasive carcinoma at surgery after VAB vs 21% with 14G CNB
- Near 3x more accurate than standard CNB for ADH, though underestimation still occurs in 18-25% of ADH cases
- Can remove entire small lesions percutaneously (useful for small fibroadenomas)
- Standard approach for stereotactic biopsy of microcalcifications
A 2026 systematic review and meta-analysis (Sharma et al., Eur Radiol PMID 41553473) directly compared VAB vs CNB in breast pathology, confirming VAB's advantages for accuracy.
7. Indications for Surgical Excision After CNB
CNB does not eliminate the need for surgical biopsy in certain scenarios. Indications for surgical excision after core biopsy (per Mulholland and Greenfield's Surgery):
- Atypical ductal hyperplasia (ADH) on CNB
- Radial scar
- Columnar cell hyperplasia with atypia
- Papillary lesions
- Lack of concordance between mammographic appearance and histologic diagnosis
- Nondiagnostic specimen (e.g., absent calcifications on specimen radiograph when biopsy done for calcifications)
- LCIS in certain settings
8. Limitations and Pitfalls of CNB
- Sampling error (false-negative): rare but possible; the false-negative rate is low but not zero. Vacuum-assisted devices reduce this substantially
- Underestimation ("upgrade" phenomenon): especially for ADH (upgraded to DCIS or invasive cancer in 5-25% at excision) and DCIS (upgraded to invasive cancer in ~20% at final surgical pathology)
- Non-diagnostic specimens: inadequate cores, absence of target tissue (calcifications missing from specimen)
- Technical limitations: very small breasts, deep posterior lesions, anticoagulated patients, pregnancy (for stereotactic approach), or inability to tolerate positioning
Summary
CNB occupies the central role in the breast pathology pathway - it is the bridge between imaging suspicion and definitive diagnosis, enabling treatment planning without the morbidity of surgical biopsy. Its pathological output extends beyond simple diagnosis to include histological grading, invasion assessment, biomarker profiling (ER/PR/HER2/Ki-67), and risk stratification of high-risk benign lesions. The principle of radiologic-pathologic concordance governs post-biopsy management and determines which patients require surgical follow-up.
Sources:
- Mulholland and Greenfield's Surgery, 7th ed. - Breast Surgery chapter
- Fischer's Mastery of Surgery, 8th ed. - Benign Breast Lesions and CNB Concordance
- Bailey and Love's Short Practice of Surgery, 28th ed. - Breast chapter
- Current Surgical Therapy, 14th ed. - Stereotactic Biopsy and Equipment
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Breast Cancer Diagnosis and Staging
- Sharma N et al. (2026). Vacuum-assisted breast biopsy vs core needle biopsy: a systematic review and meta-analysis. Eur Radiol [PMID: 41553473]
Borderline breast lesions saq
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Excellent - I now have comprehensive, textbook-sourced content for a thorough SAQ answer. Let me compile it.
Borderline Breast Lesions (B3 Lesions) - SAQ
Definition
Borderline breast lesions, categorized as B3 in the standard pathological reporting system, are lesions of uncertain malignant potential - they are neither clearly benign (B2) nor clearly malignant (B5). They are noninvasive neoplastic epithelial proliferations that carry a variable risk of concurrent adjacent malignancy (upgrade risk) and an increased long-term risk of future breast cancer in either breast.
Approximately 5-8% of all diagnostic core needle biopsies will show mammary dysplasia or proliferative disease with atypia.
Classification of Breast Epithelial Lesions by Cancer Risk
(Table 23.1, Robbins & Cotran Pathologic Basis of Disease)
| Pathologic Lesion | Relative Risk | Absolute Lifetime Risk |
|---|---|---|
| Nonproliferative (UDH, cysts, apocrine metaplasia, adenosis, simple fibroadenoma) | 1.0 | ~3% |
| Proliferative without atypia (florid UDH, sclerosing adenosis, radial scar, papilloma) | 1.5-2 | ~5-7% |
| Proliferative with atypia (ADH, ALH) | 4-5 | ~13-17% |
| Carcinoma in situ (LCIS, DCIS) | 8-10 | ~25-30% |
B3 Lesions: Individual Entities
1. Flat Epithelial Atypia (FEA)
- Pathology: A columnar cell lesion (CCL) with low-grade cytologic atypia but absence of architectural complexity. Cells are cuboidal-to-columnar with round, monomorphic, hyperchromatic, uniform nuclei and no prominent nucleoli. TDLUs are enlarged with dilated acini containing inspissated/calcified secretions.
- Considered the earliest morphologically recognizable precursor in the low-grade breast neoplasia pathway
- Expresses high levels of ER; low proliferation rate
- Often presents as microcalcifications on mammography (incidental finding)
- Upgrade risk to cancer on excision: ~5% (for pure FEA)
- Long-term relative risk: 2.0x
- Management: Observation (no excision) if: large-bore needle used (≤14G), adequately sampled, radiologic-pathologic concordance. National guidelines (NCCN) support nonsurgical management. Caveat: know your institutional upgrade rates.
2. Atypical Ductal Hyperplasia (ADH)
- Pathology: A monomorphic epithelial proliferation of the TDLU showing both cytologic atypia AND architectural changes resembling low-grade DCIS - but limited in extent and/or smaller in size. Cribriform or micropapillary patterns may be present.
- Distinguished from DCIS by: limited extent (less than 2 full duct spaces or <2 mm)
- Present in approximately 10% of biopsies performed to evaluate calcifications
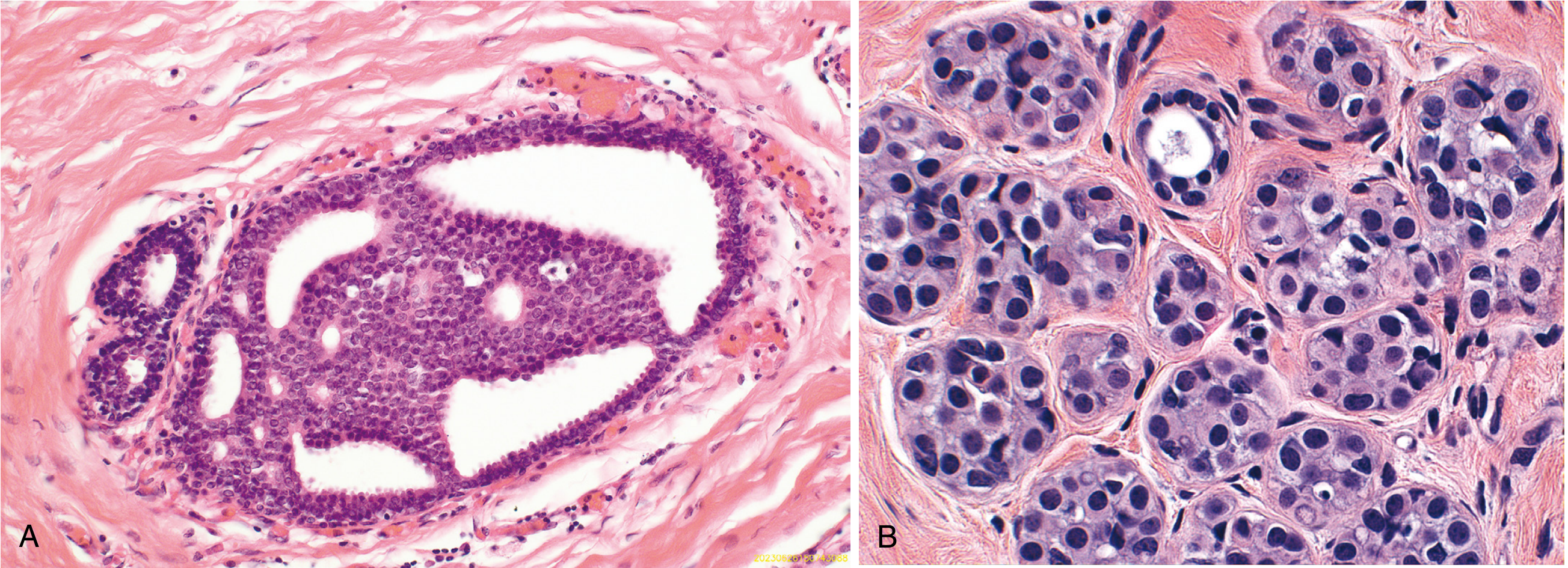
Fig: (A) ADH - partial duct involvement by monotonous cribriform proliferation. (B) ALH - monomorphic loosely cohesive cells partially filling lobule (Robbins & Cotran)
- Upgrade risk to DCIS/invasive carcinoma on excision: 10-20% (some literature 5-25%)
- Long-term relative risk: 4x general population; increases to 11-20x with family history of breast cancer
- Absolute risk: 1-2% per year (higher if >3 foci)
- Note: Standard Gail model and Tyrer-Cuzick do NOT accurately predict risk in the setting of ADH
- Management: Surgical excision is the standard recommendation UNLESS ALL of the following low-risk criteria are met:
- Large-bore needle used (<14G)
-
90% of the determinant calcifications removed (adequately sampled)
- Radiologic-pathologic concordance
- ≤2 foci of ADH
- No cell necrosis
- No mass lesion or discordance
- If observation is selected after meeting criteria: high-risk surveillance (annual mammography + annual breast MRI or whole-breast ultrasound) + chemoprevention
3. Atypical Lobular Hyperplasia (ALH)
- Pathology: Neoplastic proliferation of dyscohesive cells confined to the ductal-lobular system - histologically identical to classic LCIS but less extensive. The lobular unit must be filled with <50% of these cells, without significant distortion.
- Cells are uniform, round, loosely cohesive - pathognomonic appearance
- Shows loss of E-cadherin expression (shared feature with LCIS and invasive lobular carcinoma)
- Usually an incidental finding (not associated with specific imaging findings; calcifications may be present incidentally)
- Upgrade risk to cancer on excision: 1-4% (comparable to BI-RADS 3)
- Long-term relative risk: 3-5x general population
- Management: Observation (no excision needed) IF: incidental finding, radiologic-pathologic concordance, large-bore needle, adequately sampled, and target lesion itself does not require excision. If excised, no negative margin required.
- High-risk surveillance + chemoprevention recommended
4. Lobular Carcinoma In Situ (LCIS) - Classic Type
- Pathology: More extensive than ALH - characteristic lobular neoplasia cells distend and efface >50% of lobular acini, with significant distortion. Loss of E-cadherin is characteristic.
- A nonobligate precursor to invasive carcinoma AND a risk marker for both breasts
- Removed from the 8th edition AJCC staging system; now classified as "lobular neoplasia"
- Upgrade risk on excision: <5% when concordant and adequately sampled (no excision needed)
- Long-term relative risk: 6-10x general population; 1-2% per year
- Cumulative risk (SEER data): 11.3% at 10 years, 19.8% at 20 years
- Management: Observation if concordant (a-e criteria same as ALH above). High-risk surveillance + chemoprevention are the emphasis.
- Exception - Pleomorphic LCIS: higher-grade variant; treated more like DCIS with surgical excision
5. Radial Scar / Complex Sclerosing Lesion
- Pathology: Originates at the point of terminal duct branching. Contains a firm central fibroelastic core with elastic streaks, entrapped small tubules in fibrotic stroma, and projections containing epithelium with variable cyst formation/hyperplasia. An intact myoepithelial layer is always present. By definition, a radial scar is ≤10 mm (larger lesions = complex sclerosing lesion).
- Easily confused with malignancy on mammography - both create spiculated patterns. Distinguishing feature: the center of a radial scar is hollow ("black star/black hole"), while carcinoma has a solid central mass.
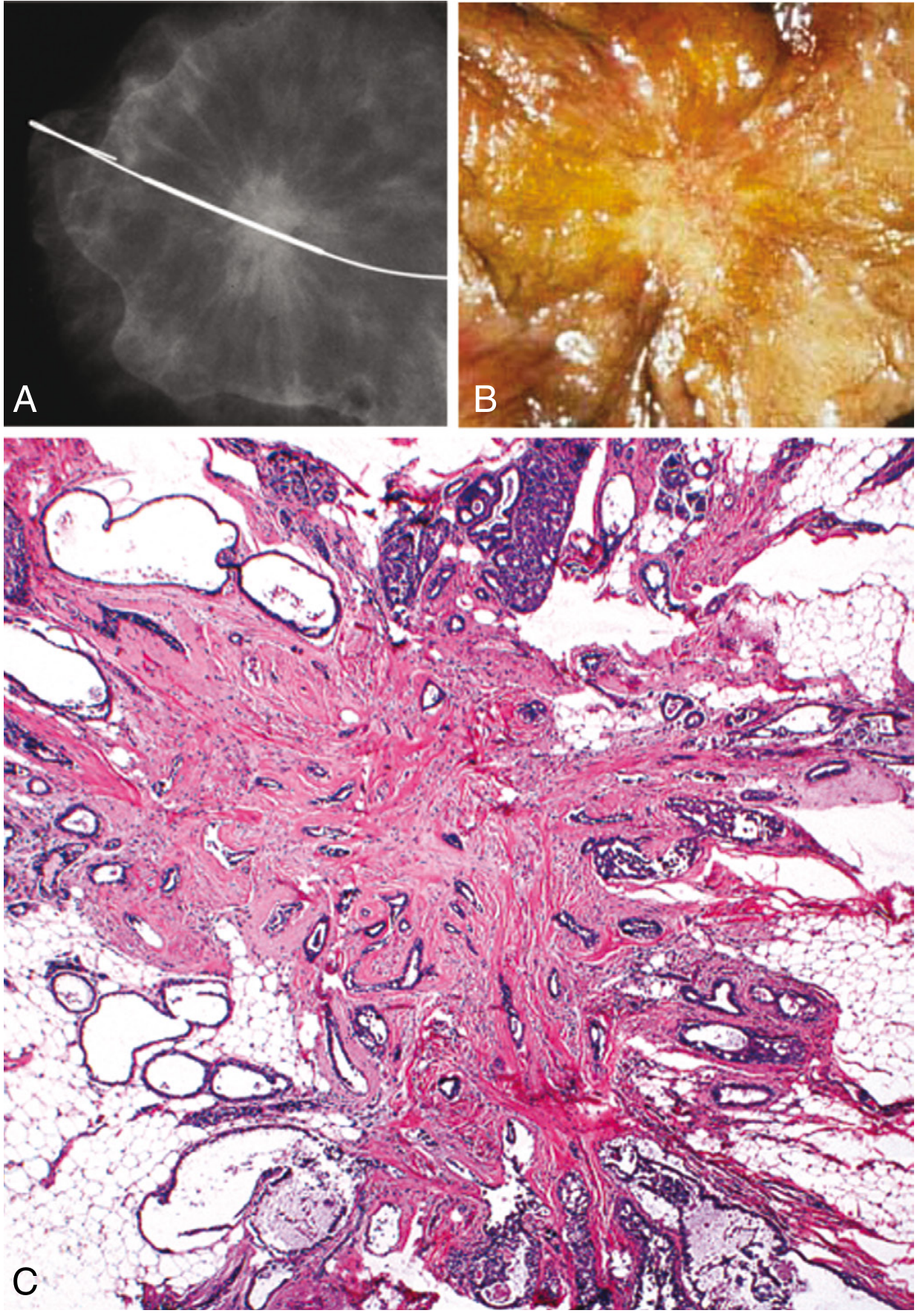
Fig: Radial scar - (A) mammographic spiculated lesion resembling cancer, (B) gross stellate fibrotic appearance, (C) histology: hollow central fibroelastic nidus with radiating epithelial projections (Robbins & Cotran)
- Upgrade risk on excision: ≤3% (low), provided: large-bore needle (≤14G), adequately sampled, size ≤10 mm, radiologic-pathologic concordance
- If discordance or associated atypia: upgrade rate rises to 26-40% - excision mandatory
- Long-term relative risk: 1.82-2.63x at 10 years; ~7% risk of breast cancer at 20 years
- Management: Observation vs. excision - multidisciplinary decision based on above criteria. Annual breast exam and mammography if observed; excise if growth/suspicious change develops.
- Incidentally found on 2-28% of benign breast biopsies
6. Papillary Lesions
-
Solitary (central) intraductal papilloma: Arises in major sub-areolar ducts. Fibrovascular core lined by both myoepithelial and luminal cells. Presents with bloody/serous nipple discharge.
- Upgrade risk averages 5-10% in modern datasets
- If adequately sampled and concordant - observation may be selected for small lesions
- Surgical excision if discordant, if >10 mm, associated with atypia, or if growth on follow-up
-
Peripheral papillomatosis (multiple papillomas): Located in terminal ductal lobular units; higher upgrade risk than solitary papilloma
- Surgical excision recommended for peripheral papillomatosis with discordance
-
Atypical papilloma (papilloma involved by ADH, ALH, or LCIS):
- Upgrade rate to carcinoma: 10-38% (wide range)
- Surgical excision is mandatory
- If excision shows no cancer, long-term relative risk is 5.1-13.1x - high-risk surveillance + chemoprevention required
Summary Table: Management of B3 Lesions
| Lesion | Upgrade Risk | Standard Management | Can Observe If... |
|---|---|---|---|
| FEA (pure) | ~5% | Observation | Concordant, large-bore, adequate |
| ADH | 10-20% | Surgical excision | Low-risk criteria met (≤2 foci, concordant, adequate, >90% removed) |
| ALH | 1-4% | Observation | Incidental, concordant, adequate |
| Classic LCIS | <5% | Observation | Concordant, adequate |
| Radial scar (no atypia, ≤10 mm) | ≤3% | Observation | Concordant, large-bore, adequate |
| Solitary papilloma (no atypia) | 5-10% | Observation or excision | Concordant, small, adequate |
| Atypical papilloma | 10-38% | Surgical excision | Never |
| Discordant any B3 | High | Surgical excision | Never |
The Upgrade Concept - Key SAQ Point
Two distinct risks must be assessed for every B3 lesion:
- Concurrent cancer risk (upgrade risk): Risk that cancer is present in adjacent breast tissue at the biopsy site RIGHT NOW - determined by surgical excision
- Future cancer development risk: Risk of developing breast cancer in either breast over the next 20 years - managed by high-risk surveillance and chemoprevention
Role of Multidisciplinary Team (MDT)
Every B3 lesion diagnosed on CNB requires multidisciplinary review (radiology + pathology + surgery). Key questions:
- Was a large-bore needle used (≤14G)?
- Was the lesion adequately sampled?
- Is there radiologic-pathologic concordance?
Concordance assessment determines whether observation or excision is appropriate.
Chemoprevention (Risk Reduction) for B3 Lesions
For patients with ADH, ALH, or LCIS (high-risk group):
- Endocrine therapy: Tamoxifen, raloxifene, anastrozole, or exemestane - taken daily for 5 years
- Reduces breast cancer risk by ~50% overall
- Combined with high-risk surveillance: clinical breast exam every 6 months + annual mammography + annual breast MRI (or whole-breast ultrasound)
- Lifestyle: maintain healthy weight, limit alcohol, moderate exercise ≥150 min/week
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Table 23.1 and Proliferative Breast Disease with Atypia
- Fischer's Mastery of Surgery, 8th ed. - Benign Breast Lesions: Histopathology, Management after CNB
- Current Surgical Therapy, 14th ed. - Proliferative Lesions with and without Atypia
- Mulholland and Greenfield's Surgery, 7th ed. - Breast chapter (Key Points)
- Grainger & Allison's Diagnostic Radiology - VAB and B3 Lesions
This is a shared conversation. Sign in to Orris to start your own chat.