Reversed takotsubos cardiomyopathy
Reading File
Finding Sources
Finding Sources
Searching PubMed
reverse takotsubo cardiomyopathy
Reading File
Finding Sources
Searching PubMed
"reverse takotsubo" OR "inverted takotsubo"
Reading File
Reading File
Reading File
Reading File
Searching Images
reverse takotsubo cardiomyopathy basal ballooning apical hyperkinesis
Searching the Web
reverse takotsubo cardiomyopathy basal ballooning definition pathophysiology clinical features
Loading Image
Loading Image
I now have comprehensive information to provide a thorough answer on reverse Takotsubo cardiomyopathy.
Reverse Takotsubo Cardiomyopathy (rTTC)
Definition & Classification
Reverse (or "inverted") Takotsubo cardiomyopathy is a morphological variant of Takotsubo syndrome (TTS) in which the basal segments of the left ventricle are hypokinetic/akinetic while the apex contracts normally or is hyperkinetic — the exact mirror image of classic TTS.
Shimizu et al. classified TTS into four wall-motion subtypes:
| Type | Pattern |
|---|---|
| Classic (apical) | Apical akinesia + basal hyperkinesia (~80% of cases) |
| Reverse (basal) | Basal akinesia/hypokinesis + apical hyperkinesia (~2–5%) |
| Mid-ventricular | Mid-wall hypokinesis + basal and apical hyperkinesia |
| Focal | Any other segmental ballooning pattern |
The InterTAK diagnostic criteria formally recognise all four subtypes, stating: "regional wall motion abnormality usually extends beyond a single epicardial vascular distribution" and that "transitions between all types can exist." — Fuster & Hurst's The Heart, 15th Ed.
Pathophysiology
The prevailing mechanism is catecholamine-mediated myocardial stunning, but the regional distribution in rTTC differs from classic TTS due to heterogeneous adrenergic receptor density:
- Classic TTS — The apex is rich in β₂-adrenoceptors (higher density than the base). During catecholamine surges, the apical β₂ receptors switch their signalling from Gs (stimulatory) to Gi (inhibitory), causing apical stunning while the base continues contracting.
- Reverse TTS — The basal segments are predominantly affected, suggesting either:
- A different sympathetic innervation pattern (higher basal adrenergic sensitivity in some individuals)
- A physical/pharmacological trigger (rather than emotional) — adrenergic agonists such as dobutamine, epinephrine, or exogenous catecholamines (as in pheochromocytoma or inotrope infusion) tend to preferentially stun the base
- Notably, rTTC is more commonly associated with physical triggers and pharmacological stress (e.g., dobutamine stress testing, liver transplantation, pheochromocytoma crisis) rather than emotional stress
Clinical Profile
Demographics: rTTC affects a younger population on average compared to classic TTS, and has a less pronounced female preponderance. Men and younger women are relatively more represented.
Common triggers:
- Pheochromocytoma / catecholamine-secreting tumours
- Exogenous catecholamines (dobutamine, epinephrine infusion)
- Dobutamine stress echocardiography
- Liver transplantation (reperfusion catecholamine surge)
- Subarachnoid haemorrhage / neurological events
- Emotional stress (less common than in classic TTS)
Symptoms: Indistinguishable from classic TTS and ACS:
- Chest pain, dyspnea, palpitations
- Pulmonary oedema, hypotension
- Syncope
ECG Findings
The ECG pattern mirrors the wall-motion distribution:
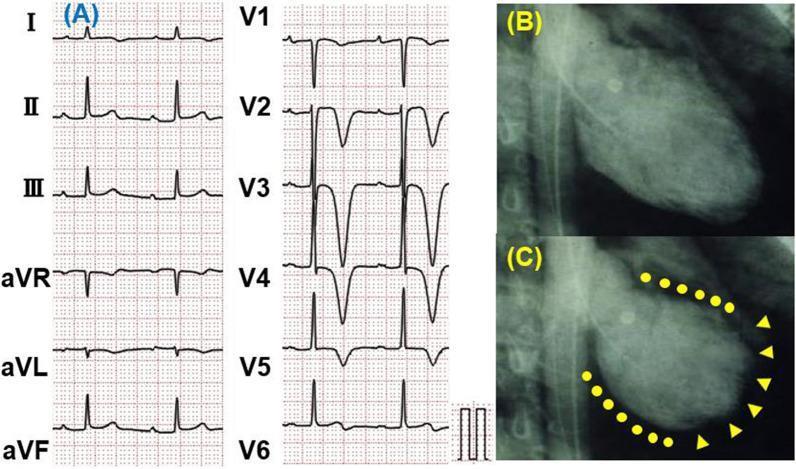
Panel A: Widespread T-wave inversions in lateral (I, aVL), inferior (II), and precordial leads (V1–V6). Panels B–C: Left ventriculography showing basal hypokinesis (dotted lines) with apical hyperkinesis (arrowheads) — the "reverse" pattern.
- ST elevation or T-wave inversions (may be less prominent in leads V4–V6 compared to classic TTS)
- QT prolongation (risk of torsades de pointes)
- ST elevation in inferior or lateral leads may be more prominent (reflecting basal ischaemia)
Echocardiography
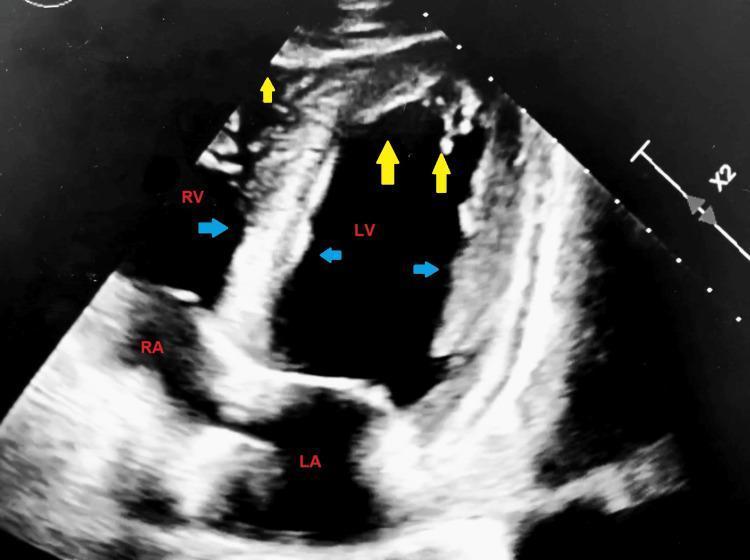
Apical 4-chamber view: yellow arrows = hyperkinetic apex; blue arrows = hypokinetic mid-to-basal LV segments. LVEF severely reduced at ~25%.
- Basal and mid-ventricular hypokinesis/akinesis
- Preserved or hyperdynamic apical contraction
- LV outflow tract obstruction is not a feature (it occurs in classic TTS due to basal hyperkinesis + septal bulge causing SAM of the mitral valve)
- Right ventricular involvement can co-occur
Diagnosis
Requires exclusion of:
- Obstructive CAD — coronary angiography (no culprit stenosis)
- Pheochromocytoma — especially in rTTC, given the strong association; 24-hr urine/plasma metanephrines should be obtained
Cardiac MRI confirms:
- Diffuse myocardial oedema without late gadolinium enhancement (distinguishes from MI and myocarditis)
- Basal distribution of wall motion abnormality
Acute Complications
Generally similar to classic TTS but note:
- No LVOT obstruction (a key difference from classic)
- Cardiogenic shock (from severe basal dysfunction)
- Arrhythmias: QTc prolongation → torsades de pointes
- LV thrombus (rare, but possible in akinetic basal segments)
Management
No randomised trials exist specific to rTTC; management follows general TTS principles:
| Situation | Approach |
|---|---|
| Pulmonary oedema | IV nitrates, diuretics |
| Haemodynamic instability | Cautious inotropes (avoid if pheochromocytoma suspected); IABP if no LVOT obstruction |
| Catecholamine surge (e.g. phaeo) | Alpha-blockade first, then beta-blockade |
| Arrhythmia / QT prolongation | Magnesium sulphate; avoid QT-prolonging drugs |
| Pharmacological trigger (dobutamine) | Cease the offending agent |
| Long-term | ACEi/ARB, beta-blocker during recovery (expert consensus); reassess for pheochromocytoma |
⚠️ If pheochromocytoma is the underlying trigger (which should always be excluded in rTTC), selective beta-blockade alone is contraindicated — it can precipitate hypertensive crisis by leaving alpha-receptors unopposed. Alpha-blockade must come first.
Prognosis
- The condition is transient and reversible in the vast majority — LV function normalises within days to weeks
- Primary rTTC (emotional trigger) has a benign prognosis
- Secondary rTTC (associated with severe physical illness or pharmacological triggers) carries a higher event rate, similar to secondary classic TTS — Fuster & Hurst's The Heart, 15th Ed.
- Recurrence risk: ~10% at follow-up (similar to classic TTS), estimated at ~2%/year — Harrison's Principles of Internal Medicine, 22nd Ed.
Key distinction summary:
| Feature | Classic TTS | Reverse TTS |
|---|---|---|
| Wall motion | Apical ballooning, basal hyperkinesis | Basal ballooning, apical hyperkinesis |
| Trigger | Emotional > physical | Physical/pharmacological > emotional |
| Demographics | Older postmenopausal women | Younger; less female-predominant |
| LVOT obstruction | Common | Absent |
| Pheochromocytoma | Occasional | Strongly associated |
| Prognosis | Benign; transient | Transient; secondary forms higher risk |
This is a shared conversation. Sign in to Orris to start your own chat.