Pneumocystis jiroveci pneumonia full details for md exams 10 marks answer from fishman and murray only
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from both Fishman's (Chapter 134) and Murray & Nadel's (Chapter 123) textbooks, plus two key images. Let me now compose the full 10-mark MD exam answer.
Pneumocystis jirovecii Pneumonia (PCP) — Complete 10-Mark MD Exam Answer
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapter 134); Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set (Chapter 123)
1. Introduction and Historical Background
Pneumocystis is an extracellular, obligate ascomycetous yeast-like fungus that is tropic to mammalian lung tissue. It produces a clinical spectrum ranging from asymptomatic colonization to a subacute-to-acute interstitial pneumonia (PCP) in susceptible hosts. First described by Carlos Chagas in 1909 and mistakenly classified as a developmental stage of Trypanosoma cruzi, the organism was correctly recognized as a separate entity by Delanoe and Delanoe in 1912 and named Pneumocystis carinii. It was not recognized as a human pathogen until 1942. The 1980s HIV/AIDS pandemic caused an explosion in incidence, with PCP accounting for more than one-fourth of community-acquired pneumonias in persons living with HIV/AIDS (PLWH) and nearly two-thirds of AIDS-defining diagnoses early in the epidemic.
In recognition of its host-species specificity, the organism infecting humans was renamed Pneumocystis jirovecii (honoring Otto Jirovec), while P. carinii remains the rat pathogen. Despite the name change, PCP (Pneumocystis pneumonia) remains the accepted abbreviation for the syndrome.
- Fishman's, Chapter 134 | Murray & Nadel's, Chapter 123
2. Organism Biology and Morphologic Forms
P. jirovecii has three predominant morphologic forms:
| Form | Size | Features |
|---|---|---|
| Trophozoite | 2-5 μm | Thin-walled, amoeboid, pseudopodia/filopodia; 10x more abundant than cysts in specimens |
| Precyst (immature cyst) | 3-8 μm | Developing sporozoites; cell wall thickens progressively |
| Mature cyst | 3-8 μm | Thick-walled, globular; contains up to 8 sporozoites (intracystic bodies, 1 μm) |
Key biological features (exam-critical):
-
P. jirovecii lacks ergosterol in its cell membrane (unlike most fungi) - instead contains cholesterol like mammalian cells. This explains intrinsic resistance to azoles and amphotericin B.
-
The cell wall is low in chitin but rich in (1,3)-β-D glucan, making this a target for echinocandins and a basis for serologic testing (serum β-D-glucan assay).
-
Cannot be cultured in vitro beyond a few replication cycles - no culture-based diagnosis is possible.
-
Demonstrates strict host-species specificity - P. jirovecii infects only humans.
-
Fishman's, Ch. 134
3. Life Cycle
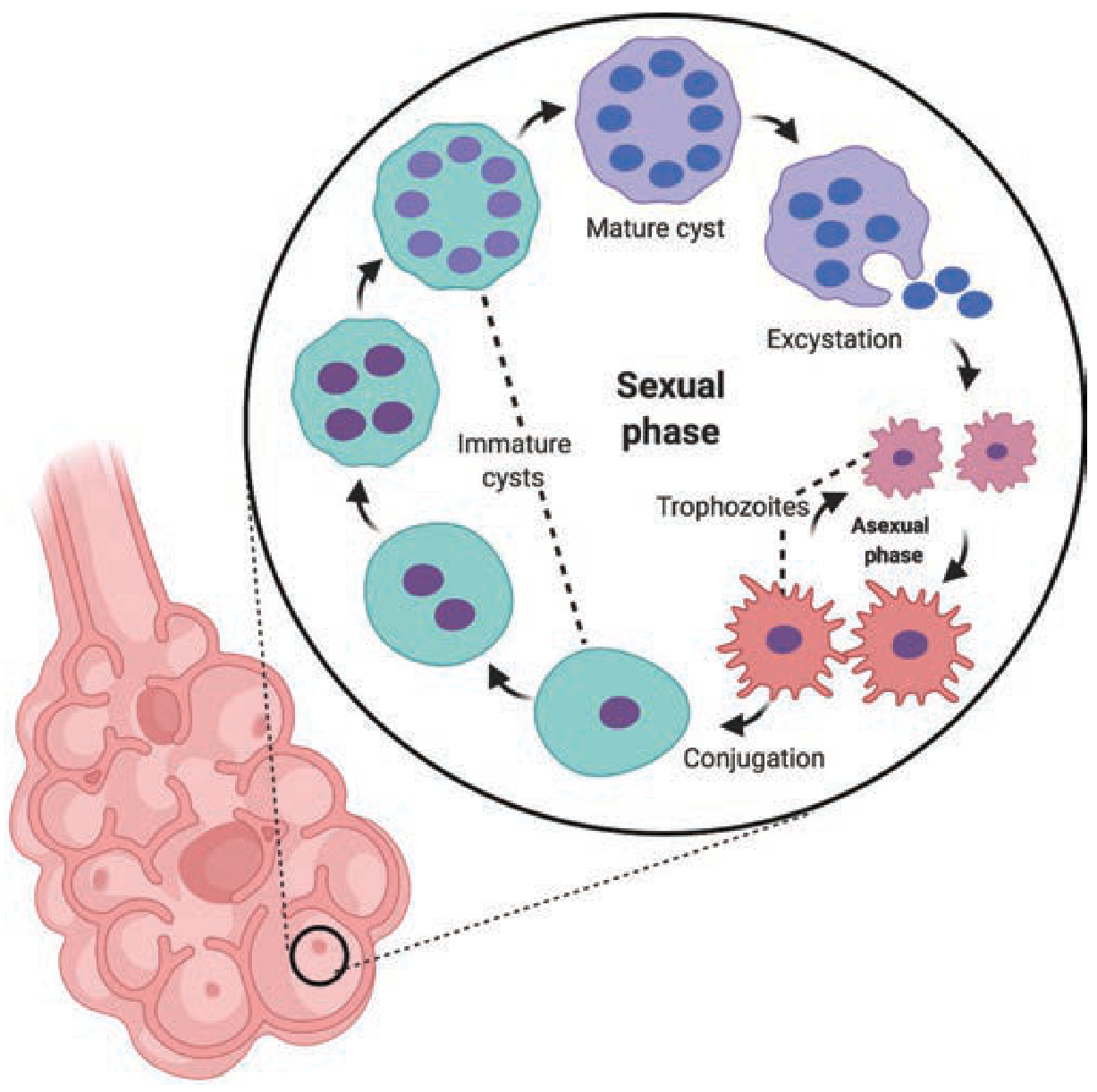
Figure: P. jirovecii life cycle (Fishman's, Fig. 134-1). Mature cysts undergo excystation to release sporozoites. Sporozoites develop into trophozoites (asexual phase - binary fission). Two haploid trophozoites conjugate into a precyst (sexual phase), which matures into a full cyst.
Proposed life cycle:
-
Aerosolized mature cysts are inhaled into terminal alveoli
-
Excystation releases sporozoites into lung tissue
-
Sporozoites → trophozoites → binary fission (asexual proliferation)
-
Two haploid trophozoites → conjugation → precyst (diploid) → mature cyst (sexual phase)
-
Mature cysts are essential for transmission; organisms do not bud (distinguishing from other yeasts)
-
Fishman's, Ch. 134
4. Epidemiology and Risk Factors
Ubiquitous worldwide. Seropositivity approaches 85-100% of the U.S. population by age 2-4 years, indicating near-universal early-life exposure (Murray & Nadel's). Primary infection is either a mild respiratory illness or asymptomatic.
Transmission: Airborne, via close contact with an infected host. Human-to-human transmission is strongly supported by molecular studies - genotypically identical aerosolized organisms have been identified in air samples from clinic rooms, bronchoscopy suites, and hospital rooms of PCP patients. Studies suggest close contact for as little as 24 hours may suffice. The debate between reactivation of latent infection vs. de novo re-infection has not been fully resolved; evidence supports both mechanisms.
Risk factors - HIV-infected patients:
- CD4+ count < 200 cells/μL (accounts for ~95% of cases in adolescents/adults) - Murray & Nadel's
- CD4+ percentage < 14%
- Prior episode of PCP
- Oropharyngeal candidiasis
Risk factors - HIV-negative patients (now majority in developed world, 60-70% of new infections):
- Prolonged high-dose corticosteroids (≥0.3 mg/kg for ≥2 weeks)
- Hematologic malignancies (particularly ALL, lymphoma)
- Solid organ transplant recipients
- Hematopoietic stem cell transplant (HSCT) recipients
- Cytotoxic chemotherapy (cyclophosphamide, methotrexate)
- Autoimmune diseases (SLE, vasculitis, inflammatory bowel disease)
- Biologic agents: TNF inhibitors, anti-CD20 (rituximab), anti-CD52 (alemtuzumab)
- Primary immunodeficiencies (SCID, hyper-IgM syndrome)
Notably, PCP in HIV-negative patients tends to present more acutely with higher mortality compared to the indolent presentation in HIV-positive patients.
- Fishman's, Ch. 134
5. Pathogenesis
-
Attachment and colonization: P. jirovecii trophozoites attach closely to type I pneumocytes via surface glycoproteins (major surface glycoprotein, MSG/gp120), which undergo antigenic variation to evade host immunity. This attachment is mediated by fibronectin, vitronectin, and surfactant proteins.
-
Immune evasion: The organism is extracellular and resides within the alveolar space. CD4+ T-lymphocytes are the primary defense; CD4 depletion (as in HIV) is the single most important predisposing factor. Alveolar macrophages, neutrophils, and CD8+ T cells also contribute to defense but cannot compensate alone.
-
Alveolar injury: The combination of organism burden + host inflammatory response causes:
- Exudative alveolitis with characteristic foamy, eosinophilic, honeycomb-like alveolar exudate (containing organisms, surfactant debris, and macrophages)
- Type I pneumocyte damage → disruption of alveolar-capillary membrane
- Impaired surfactant production and function
- Interstitial edema and thickened alveolar walls
- Severe cases progress to diffuse alveolar damage (DAD) with hyaline membrane formation
-
Paradoxically, patients with very low CD4+ counts (< 50 cells/μL) may have less inflammatory injury but higher organism burden; those with a recovering immune system (after ART initiation) can develop immune reconstitution inflammatory syndrome (IRIS) - a paradoxical worsening of clinical and radiographic features.
-
(1,3)-β-D-glucan released from the cell wall into the bloodstream during active infection serves as a diagnostic biomarker and mediates pro-inflammatory cytokine release.
- Fishman's, Ch. 134
6. Clinical Features
HIV-positive patients (subacute presentation - hallmark):
- Prodrome of several weeks - a key distinguishing feature vs. bacterial pneumonia (3-5 days)
- Classic triad: Fever + nonproductive cough + progressive dyspnea on exertion
- High fever, rigors, purulent sputum, and pleuritic chest pain are uncommon - their presence suggests bacterial pneumonia
- Physical examination: lungs may be normal; when abnormal, inspiratory crackles are the most common finding (associated with greater severity and increased mortality)
- Oxygen desaturation on exertion - sensitive but nonspecific indicator
HIV-negative patients (acute, more fulminant):
-
Shorter prodrome (days rather than weeks)
-
More severe hypoxia at presentation
-
Higher ICU admission rates and mortality
-
Murray & Nadel's, Ch. 123
7. Laboratory and Imaging
Laboratory:
- Serum LDH: Elevated in PCP (nonspecific - does not establish or exclude diagnosis)
- Serum (1,3)-β-D-glucan: Sensitive but not specific (elevated in other fungal infections); useful as screening/supportive tool
- ABG: Hypoxemia (PaO₂ < 70 mmHg in severe disease); widened alveolar-arterial (A-a) gradient > 35 mmHg defines severe disease requiring adjunctive corticosteroids
- S-LDH and β-D-glucan combined improve diagnostic accuracy
Chest Radiograph (CXR):
- Classic: Bilateral symmetrical reticular or granular opacities beginning in the perihilar region and extending peripherally
- May be normal in 0-39% of cases despite active infection - normal CXR does not exclude PCP
- Thin-walled cysts (pneumatoceles): Seen in 10-20% of cases - single or multiple; can be large; predispose to spontaneous pneumothorax (a classic complication of PCP)
- Less common: unilateral/asymmetrical opacities, lobar consolidation, nodules (±cavitation), miliary pattern, upper lobe predominance (particularly with aerosolized pentamidine prophylaxis breakthrough)
High-Resolution CT (HRCT):
- Bilateral ground-glass opacities - the hallmark CT finding; typically perihilar/central
- Useful when CXR is normal but clinical suspicion is high
- Can demonstrate pneumatoceles not visible on CXR
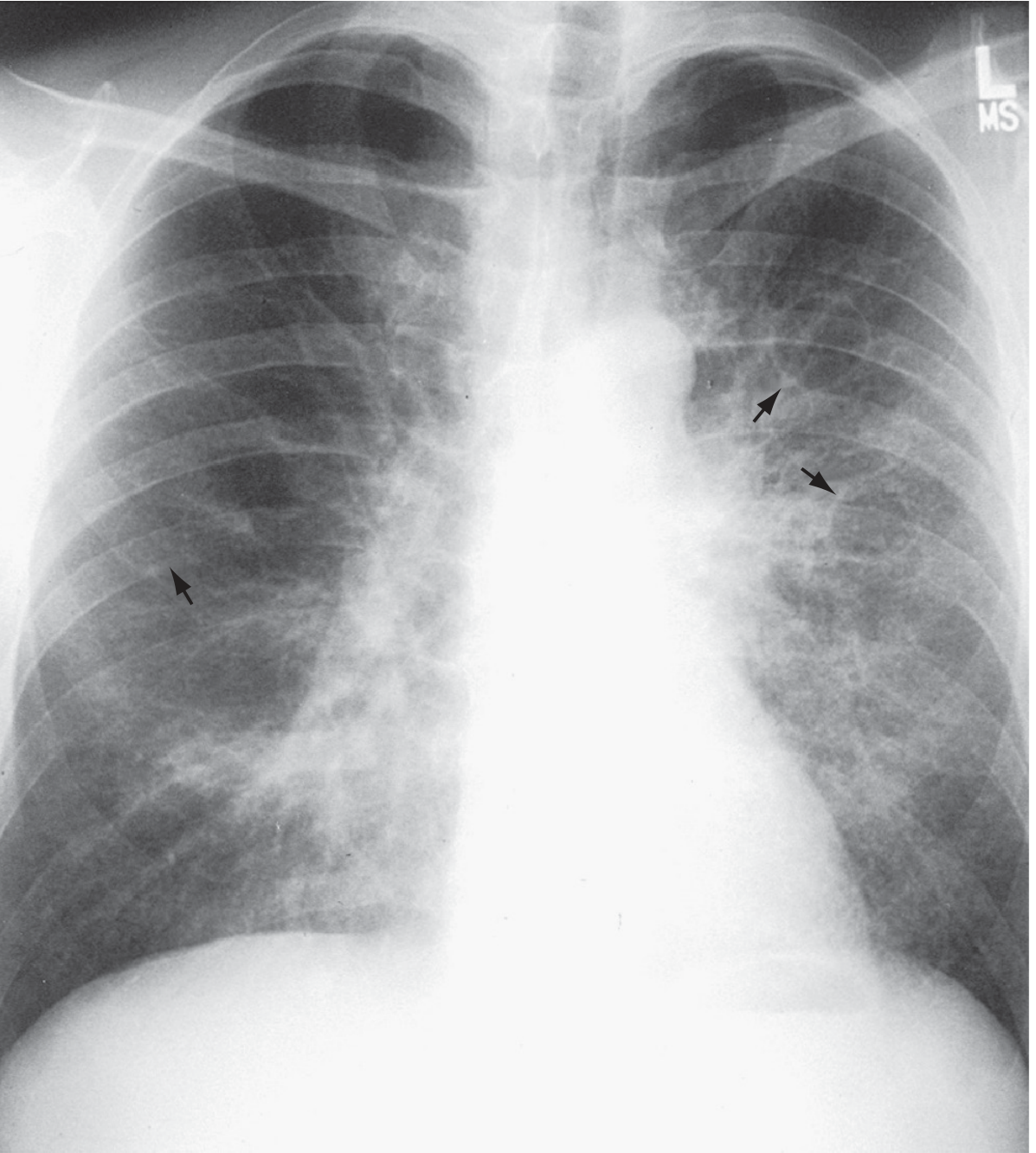
Figure: PCP in an HIV-infected patient. Bilateral perihilar granular opacities with pneumatoceles (arrows). (Murray & Nadel's, Fig. 123.4)
- Murray & Nadel's, Ch. 123 | Fishman's, Ch. 134
8. Diagnosis
Gold standard: Microscopic visualization of P. jirovecii in stained respiratory specimens.
Culture is not possible.
Staining Methods:
| Stain | Stains | Notes |
|---|---|---|
| Gomori Methenamine Silver (GMS) | Cyst wall only | High sensitivity; stains cyst walls black |
| Toluidine Blue-O | Cyst wall only | Rapid; for cysts only |
| Giemsa / Diff-Quik | Both cysts AND trophozoites | Better overall organism detection |
| Direct Immunofluorescence (DFA/monoclonal antibody) | Both forms | Most sensitive conventional stain; gold standard for BAL |
| PCR (real-time) | DNA detection | Most sensitive; lower specificity (detects colonization) |
Specimen Sources (in order of increasing invasiveness):
-
Induced Sputum (IS): First-line non-invasive approach. Sensitivity 50-90% in HIV-positive patients; lower in HIV-negative. A negative result mandates bronchoscopy.
-
Bronchoalveolar Lavage (BAL): Standard of care diagnostic procedure. Sensitivity ~97% for HIV-positive patients. Should be performed in the most affected lobe on CXR; if diffuse disease, right middle lobe; if upper-lobe predominant (pentamidine breakthrough), lavage both an upper lobe and RML. BAL + DFA staining is the diagnostic cornerstone.
-
Oral Wash + PCR: Sensitivity 54-100% in HIV-positive patients; 44-100% in HIV-negative. Less invasive than bronchoscopy; used when bronchoscopy is unavailable or high-risk.
-
Transbronchial Biopsy: Added diagnostic value when BAL is equivocal; rarely necessary alone. Sensitivity 43-96%.
-
Open/Surgical Lung Biopsy: Rarely performed today; reserved for cases with multiple potential pathogens.
Consensus Diagnostic Criteria (EORTC/MSGERC):
- Proven PCP: Detection of organism by staining in BAL, sputum, or lung tissue
- Probable PCP: ≥1 host criterion + clinical features (fever, cough, dyspnea) + suggestive imaging + positive non-stain test (β-D-glucan or PCR) - Fishman's, Ch. 134
9. Treatment
Duration: 21 days for all forms of PCP.
First-Line Treatment:
Trimethoprim-Sulfamethoxazole (TMP-SMX) - drug of choice for mild, moderate, and severe PCP:
- TMP: 15-20 mg/kg/day
- SMX: 75-100 mg/kg/day
- Divided into 3-4 daily doses
- IV route: recommended for moderate-severe PCP (can transition to oral after clinical improvement)
- Mechanism: inhibits folate synthesis (TMP inhibits dihydrofolate reductase; SMX inhibits dihydropteroate synthase)
Adverse effects (more frequent in HIV-infected patients):
- Rash (common; can be severe: Stevens-Johnson syndrome, toxic epidermal necrolysis)
- Fever, GI complaints (nausea, vomiting)
- Elevated aminotransferases
- Hyperkalemia (TMP blocks ENaC)
- Bone marrow suppression (anemia, neutropenia) - typically in week 2
Alternative Regimens (for TMP-SMX intolerance/allergy):
| Regimen | Indication |
|---|---|
| IV Pentamidine (4 mg/kg/day) | Moderate-severe; most effective alternative; toxicities: nephrotoxicity, hypoglycemia/hyperglycemia, hypotension, arrhythmias |
| Clindamycin + Primaquine | Mild-moderate; oral; check G6PD before primaquine |
| TMP + Dapsone | Mild-moderate; oral; check G6PD |
| Atovaquone | Mild PCP only; oral suspension; better tolerated; less effective |
| Echinocandins | Emerging evidence (targets β-D-glucan synthase); not yet first-line |
Adjunctive Corticosteroids (exam-critical):
Indications (HIV-positive adults/adolescents):
- PaO₂ < 70 mmHg on room air, OR
- A-a gradient > 35 mmHg
Regimen (oral prednisone or IV methylprednisolone):
- Days 1-5: Prednisone 40 mg twice daily
- Days 6-10: Prednisone 40 mg once daily
- Days 11-21: Prednisone 20 mg once daily
Must be started at the same time as anti-Pneumocystis therapy (or before), regardless of whether diagnosis is confirmed. Mechanism: attenuates the inflammatory response that drives hypoxemia and lung injury (particularly relevant as organisms die and release antigenic material).
Mortality: Early in the AIDS epidemic, acute respiratory failure from PCP requiring mechanical ventilation had mortality >86%. With modern management (corticosteroids, lung-protective ventilation, ART), mortality is ~30-50% for ventilated patients.
- Murray & Nadel's, Ch. 123 | Fishman's, Ch. 134
10. Prophylaxis
Primary Prophylaxis Indications (HIV):
- CD4+ count < 200 cells/μL OR CD4+ percentage < 14%
- History of oropharyngeal candidiasis
- Irrespective of ART status
Discontinuation of Prophylaxis:
- When CD4+ count rises to > 200 cells/μL for at least 3 months as a result of ART
- Can consider discontinuation at CD4+ 100-200 cells/μL if HIV RNA is undetectable for ≥3-6 months
Secondary Prophylaxis:
- Any patient with prior PCP episode - continue indefinitely until CD4+ > 200 cells/μL for ≥3 months
Drug Options:
| Drug | Dose | Notes |
|---|---|---|
| TMP-SMX (DS) | 1 DS tablet daily (or 3x/week) | First-line; also covers Toxoplasma gondii |
| Dapsone | 100 mg/day OR 50 mg BD | Check G6PD; add pyrimethamine + leucovorin for Toxoplasma coverage if CD4 < 100 |
| Atovaquone suspension | 1500 mg/day with food | Oral; well tolerated |
| Aerosolized pentamidine | 300 mg monthly (Respirgard II nebulizer) | Effective and well-tolerated; risk of breakthrough at CD4 < 100; upper lobe breakthrough with prophylaxis failure |
TMP-SMX is also protective against bacterial infections and toxoplasmosis.
Prophylaxis in HIV-Negative Immunocompromised Patients:
-
TMP-SMX (one SS or DS tablet daily/3x weekly) is recommended for solid organ transplant recipients, HSCT recipients, patients on high-dose steroids + T-cell depleting agents, and those on anti-CD20/CD52 biologics.
-
Murray & Nadel's, Ch. 123 | Fishman's, Ch. 134
11. IRIS and Special Considerations
Immune Reconstitution Inflammatory Syndrome (IRIS):
HIV-infected patients who initiate ART during or shortly after PCP treatment may develop a paradoxical worsening of clinical and radiographic features (IRIS). Mechanism: recovering CD4+ T cells mount an exuberant inflammatory response to residual Pneumocystis antigens. IRIS rarely requires discontinuation of ART; symptomatic management is standard. Occasionally causes respiratory failure. Diagnosis is one of exclusion.
Extrapulmonary PCP: Rare; seen in highly immunosuppressed patients with heavy organism burden and structural lung disease. Most commonly reported sites: lymph nodes, spleen, liver, retina (choroidal lesions), bone marrow.
Pneumothorax: A classic and feared complication, particularly in the setting of pneumatoceles. Bilateral pneumothorax in an AIDS patient should always raise suspicion of PCP.
Summary Box (High-Yield for Exams)
| Feature | Key Point |
|---|---|
| Organism | Ascomycetous fungus; no ergosterol → resistant to azoles/amphotericin |
| Hallmark host factor | CD4 < 200 cells/μL (HIV); prolonged steroids (non-HIV) |
| Classic presentation (HIV) | Weeks of fever, nonproductive cough, exertional dyspnea |
| CXR | Bilateral perihilar reticular/granular opacities; pneumatoceles |
| CT | Bilateral ground-glass opacities |
| Diagnostic gold standard | BAL + DFA staining |
| Most sensitive test | PCR (lacks specificity) |
| Serum marker | (1,3)-β-D-glucan, serum LDH (elevated) |
| First-line treatment | TMP-SMX × 21 days (IV for moderate-severe) |
| Steroids indication | PaO₂ < 70 mmHg or A-a gradient > 35 mmHg |
| First-line prophylaxis | TMP-SMX DS 1 tablet/day |
| Stop prophylaxis when | CD4 > 200 for ≥3 months on ART |
| Key complication | Spontaneous pneumothorax (from pneumatoceles) |
| IRIS | Paradoxical worsening after ART initiation |
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set, Chapter 134 (Nussbaum & Azar); Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set, Chapter 123.
This is a shared conversation. Sign in to Orris to start your own chat.