Trigger finger and pulleys
Reading File
Finding Sources
Finding Sources
Searching PubMed
"trigger finger" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all the information needed for a thorough response. Here is the complete summary:
Trigger Finger and the Pulley System
The Flexor Tendon Pulley System
The flexor tendons of each finger run through a series of fibrous tunnels (the tendon sheath) held in place by annular (A) and cruciate (C) pulleys. These pulleys keep the tendon closely apposed to the bone and prevent "bowstringing."
Finger Pulleys (A1-A5 + C1-C3)
| Pulley | Location |
|---|---|
| A1 | Over the MCP joint (metacarpal head) |
| A2 | Over the proximal part of the proximal phalanx |
| A3 | Over the PIP joint |
| A4 | Over the middle part of the middle phalanx |
| A5 | Over the DIP joint |
| C1, C2, C3 | Between A2-A3, A3-A4, A4-A5 (thinner, collapse with flexion) |
A2 and A4 are the most biomechanically critical - they must be preserved or repaired to prevent bowstringing.
Thumb Pulleys
The thumb has three pulleys:
- A1 - just proximal to the MP joint
- Oblique pulley - on the proximal part of the proximal phalanx (connects to adductor pollicis; functionally equivalent to A2 in the fingers)
- A2 - over the distal portion of the proximal phalanx
A variable fourth "annular" pulley is found in ~75% of patients and may contribute to thumb trigger stenosis.
Trigger Finger (Stenosing Tenosynovitis)
Pathophysiology
The mechanism is stenosis at the A1 pulley (the proximal portion of the tendon sheath, at the volar MCP crease). Repetitive forceful flexion or chronic inflammation causes thickening and narrowing of the A1 pulley. The flexor tendon (FDS/FDP) develops a fusiform nodule just proximal to or at the A1 pulley that catches when traversing the narrowed sheath.
- As the finger extends, the nodule gets stuck at the proximal edge of the A1 pulley - producing the characteristic painful "snap" when it finally clears
- In advanced cases, the finger can lock in flexion (unable to extend passively or actively)
- Histology: fibrocartilaginous metaplasia of the pulley and/or FDS tendon
- In rheumatoid patients, a nodule distal to the A1 pulley can also cause triggering
Epidemiology & Risk Factors
- Most common in women >50 years old
- Ring and middle fingers most commonly affected in adults
- Strong associations with diabetes mellitus (most significant), hypothyroidism, and inflammatory arthropathy (RA, gout)
- Concomitant carpal tunnel syndrome in 40-60% of patients
- Only 30% resolve spontaneously
Clinical Presentation
Symptoms progress along a spectrum (Green Classification):
| Grade | Description |
|---|---|
| I | Pain and tenderness at the A1 pulley |
| II | Catching of the finger |
| III | Locking of the finger - passively correctable |
| IV | Fixed, locked finger (cannot be passively extended) |
- Patients often mislocate pain to the PIP joint (finger) or IP joint (thumb) rather than the true site at the MCP level
- Palpable nodule at the base of the finger in the palm; the nodule moves with tendon movement
- Differential: intraarticular loose bodies, degenerative joint disease, extensor tendon subluxation, Dupuytren contracture
Treatment
Nonoperative
- Splinting - MCP blocking splint at 10-15° flexion for 6-10 weeks; may be combined with heat/ice
- NSAIDs - reduce inflammation
- Corticosteroid injection into the flexor tendon sheath:
- Approximately 60% achieve success after a single injection
- Up to 3 injections given ~3 weeks apart are acceptable
- Dose: 10-15 mg methylprednisolone acetate + 1-2 mL lidocaine (25-27 gauge needle)
- Approach: needle at 45° distal inclination into the tendon sheath at the A1 pulley level
- Intrasheath placement is NOT required for success; intratendinous injection should be avoided
- Complication: focal palmar fat atrophy; may transiently elevate blood glucose for >5 days
- ~50% recurrence rate at 1 year
- Diabetic patients are less responsive - may be better served by early surgery; preoperative hypoglycemia increases infection risk after both injection and release
Operative (A1 Pulley Release)
Indicated when nonoperative measures fail. ~97% complete resolution rate.
Open release (Technique 81.2 - Campbell's):
- Local anesthetic + pneumatic tourniquet (or WALANT - wide-awake local anesthesia no tourniquet with epinephrine)
- Transverse incision ~2 cm:
- Several mm distal to the distal palmar crease for middle, ring, and small fingers
- Several mm distal to the proximal palmar crease for the index finger
- Carefully protect digital nerves (especially the radial digital nerve of the thumb, which is particularly superficial and vulnerable)
- Spread subcutaneous tissue to expose the annular pulley system
- Divide the A1 pulley (and A0/proximal palmar pulley for trigger digits); for the thumb, release only A1 - avoid cutting the oblique pulley distally
- Have the patient actively flex/extend the digit to confirm triggering is resolved
- Persistent triggering after A1 release → consider resection of the ulnar slip of FDS
- In RA patients: prefer FDS slip excision over A1 pulley release (A1 release can worsen ulnar drift at the MCP)
Percutaneous release:
- Needle or push-knife technique under ultrasound guidance
- Risks: incomplete release, flexor tendon or digital nerve injury (especially index finger and thumb)
- A 2024 meta-analysis (PMID 38953949) found ultrasound guidance improves outcomes vs. non-guided percutaneous release
Pediatric Trigger Finger
- Trigger thumb in children: pathologic nodular thickening called "Notta's node" (not seen in adults); presents as mechanical catching or fixed IP joint flexion in early childhood; considered developmental rather than truly congenital
- Treatment: observation initially; annular pulley release at age 2-4 to prevent permanent IP joint contracture
- Pediatric trigger finger: usually caused by an anatomic anomaly (in contrast to adults where it is acquired)
Key Clinical Pearls
- The A1 pulley is the site of pathology in virtually all trigger finger cases
- A2 and A4 pulleys are the critical biomechanical ones to preserve during any flexor tendon surgery
- Thumb trigger release must spare the oblique pulley; RA trigger finger should be treated with FDS slip resection not pulley release
- Diabetes is the most clinically significant comorbidity - less response to injection, higher surgical infection risk, cost-analysis favors upfront surgery
- Post-release triggering can occur from catching on the palmar aponeurosis transverse fibers and usually resolves with time
Sources:
- Campbell's Operative Orthopaedics, 15th Ed. 2026, pp. 4497-4499
- Miller's Review of Orthopaedics, 9th Ed., p. 8957-8997
- Imaging Anatomy Text and Atlas, Vol. 3, p. 1307-1318
- Rosen's Emergency Medicine, pp. 3063-3092
- Tintinalli's Emergency Medicine, p. 3457
- Rheumatology, 2-Volume Set (Elsevier 2022), pp. 5436-5451
- Recent evidence: Ultrasound-guided vs. non-guided A1 pulley release [PMID 38953949, Int Orthop 2024]
Tendons and pulleys of finger
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the material needed for a comprehensive answer. Let me compile it.
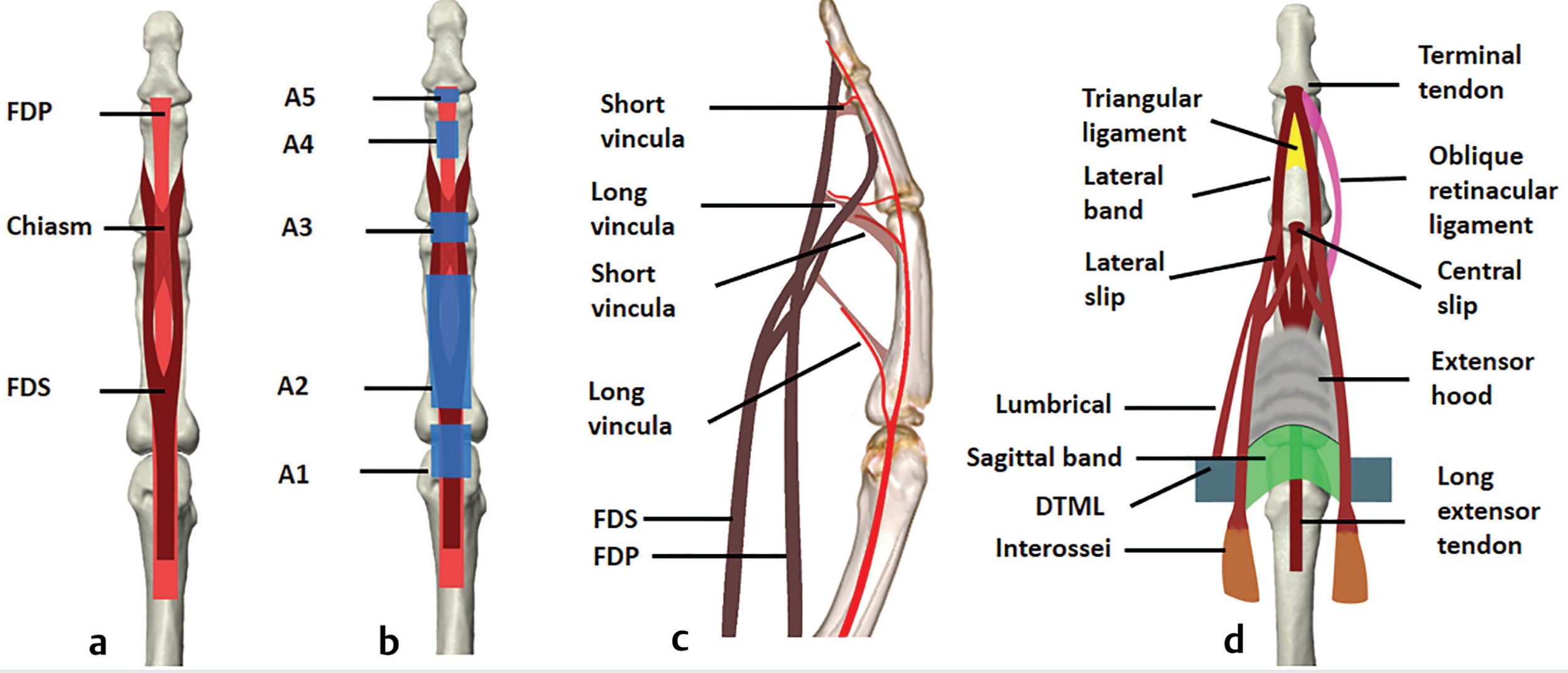
Tendons and Pulleys of the Finger
1. The Flexor Tendons
Each finger (digits 2-5) has two flexor tendons running along its palmar (volar) surface:
Flexor Digitorum Superficialis (FDS)
- Originates from the medial epicondyle and the proximal radius/ulna
- Enters the digital flexor sheath and splits into two slips at the level of the proximal phalanx
- The two slips decussate (cross each other) near the PIP joint - this crossing point is called Camper's chiasm
- After decussating, the slips reunite and insert on the sides of the middle phalanx
- Action: flexes the PIP joint (and, secondarily, the MCP joint)
Flexor Digitorum Profundus (FDP)
- Passes through the split in the FDS at Camper's chiasm (hence "profundus" going deeper to become more superficial distally)
- Inserts on the base of the distal phalanx
- Action: flexes the DIP joint (and all proximal joints)
Thumb Flexor
- The thumb has only one flexor tendon - the Flexor Pollicis Longus (FPL)
- Inserts on the base of the distal phalanx of the thumb
- Flexes the IP joint of the thumb
Blood Supply - Vincula
Tendons receive nutrition both from synovial fluid within the sheath and from vincula - small vascular folds connecting the tendons to the phalanges:
- Vincula brevia (short): to the distal FDS and distal FDP insertions
- Vincula longa (long): to the FDP (may be considered an extension of the FDS vincula brevis)
2. The Pulley System
The flexor tendons run through a fibrous digital sheath held close to the bone by a series of pulleys. These prevent bowstringing of the tendons during flexion.
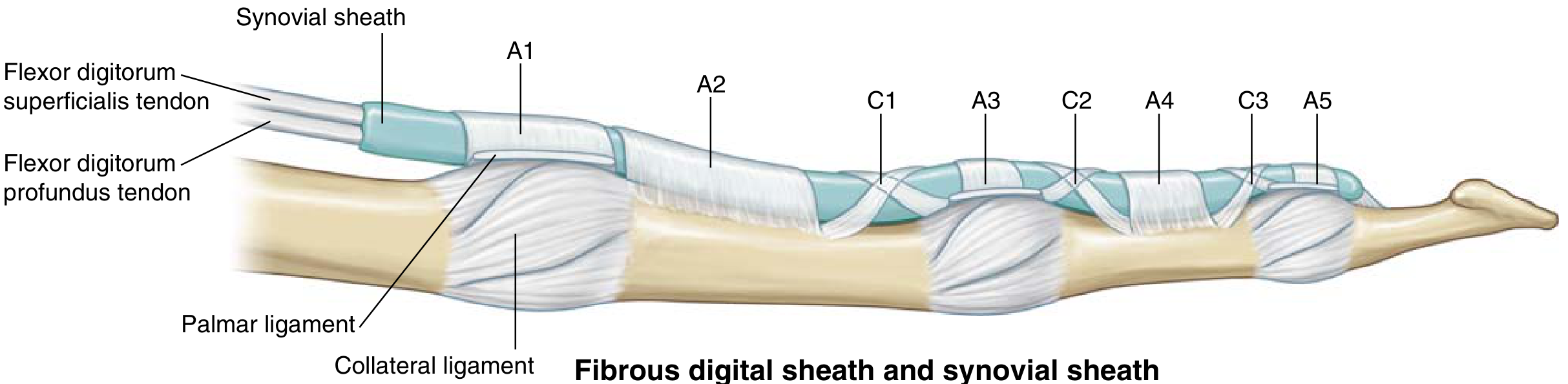
Annular Pulleys (A1-A5) - thick, rigid
| Pulley | Location | Clinical note |
|---|---|---|
| A0 | Proximal palmar (palmar aponeurosis) | Released with A1 in trigger finger surgery |
| A1 | Over the MCP joint (metacarpal head) | Site of stenosing tenosynovitis (trigger finger) |
| A2 | Over the proximal part of proximal phalanx | Most important - must be preserved |
| A3 | Over the PIP joint | |
| A4 | Over the middle part of middle phalanx | Second most important - must be preserved |
| A5 | Over the DIP joint |
Cruciate Pulleys (C1-C3) - thin, flexible
| Pulley | Location |
|---|---|
| C1 | Between A2 and A3 |
| C2 | Between A3 and A4 |
| C3 | Between A4 and A5 |
The cruciate pulleys are much thinner than the annular pulleys and collapse with finger flexion, allowing the rigid annular pulleys to approximate. They are expendable surgically.
Why A2 and A4 Are Critical
These are the longest and mechanically most important pulleys. Loss of A2 alone causes significant bowstringing; loss of both A2 and A4 renders the finger nearly non-functional for grip. They must be preserved or reconstructed whenever possible during flexor tendon surgery.
Proximal to the Digital Sheath
Before entering the digital sheath, the flexor tendons run through the carpal tunnel (Zone IV) and the palm (Zone III). In the palm, the palmar aponeurosis pulley (A0) - formed by the transverse fibers of the palmar fascia and the septa of Legueu and Juvara - provides an additional proximal constraint.
3. Thumb Pulley System
The thumb has three pulleys, distinct from the finger system:
| Pulley | Location |
|---|---|
| A1 | Just proximal to the MP joint |
| Oblique pulley | Over the proximal part of the proximal phalanx; arises from the adductor pollicis - functionally equivalent to A2 in the fingers |
| A2 | Over the distal part of the proximal phalanx |
The oblique pulley is the most critical in the thumb; it must be preserved during trigger thumb release.
4. Flexor Tendon Zones
The flexor tendon system is divided into zones that have clinical relevance for injury management and prognosis:
| Zone | Location | Significance |
|---|---|---|
| Zone I | Distal to FDS insertion | FDP only; avulsion injuries (jersey finger) |
| Zone II | A1 pulley → FDS insertion ("No man's land") | Both FDS and FDP; historically worst prognosis for repair; within the sheath |
| Zone III | Distal edge of carpal tunnel → A1 pulley | Lumbrical origin; outside sheath |
| Zone IV | Within the carpal tunnel | All 9 flexor tendons + median nerve |
| Zone V | Proximal to carpal tunnel | Forearm |
Zone II is the most challenging for repair because:
- Both FDS and FDP must be repaired within the tight sheath
- Risk of adhesions forming between the repaired tendon and the sheath
- Early active mobilization protocols are required post-repair
Thumb zones: TI (distal to FPL insertion), TII (A1 pulley to FPL insertion), TIII (proximal to A1, distal to carpal tunnel)
5. The Extensor Mechanism
The dorsal side is far more complex than a single tendon:
Extrinsic Component
- Extensor digitorum communis (EDC) - primary extensor, runs to all four fingers
- Extensor indicis proprius (EIP) - independent extensor to the index finger
- Extensor digiti minimi (EDM) - independent extensor to the little finger
At the MCP joint, the extensor tendon is held centered over the joint by the sagittal bands, which arise from the volar plate. Sagittal band injury → extensor tendon subluxation.
The Extensor Hood (Dorsal Aponeurosis)
At the proximal phalanx, the extensor mechanism trifurcates:
- Central slip → inserts on the dorsal base of the middle phalanx (extends PIP joint)
- Two lateral bands → continue distally, converging to form the terminal tendon inserting on the dorsal base of the distal phalanx (extends DIP joint)
Intrinsic Contribution
The lumbricals and interossei join the extensor mechanism on the lateral sides of the proximal phalanx and contribute to the lateral bands. This is why intrinsic muscles both flex the MCP and extend the IP joints.
Key Ligaments of the Extensor Mechanism
| Structure | Attachments | Function |
|---|---|---|
| Sagittal bands | Covers MCP joint; arises from volar plate | Centers extensor tendon; allows MCP extension |
| Transverse retinacular ligament | PIP joint level | Maintains lateral bands in proper position |
| Oblique retinacular ligament (Landsmeer) | A4 pulley → terminal tendon | Passive DIP extension when PIP extended |
| Triangular ligament | Connects the two lateral bands distally | Prevents dorsal separation of lateral bands |
Clinical Correlates of the Extensor Mechanism
- Mallet finger - rupture or avulsion of the terminal tendon at the DIP → DIP held in flexion, cannot actively extend
- Boutonniere deformity - disruption of the central slip at the PIP → PIP flexion, DIP hyperextension (lateral bands migrate volar to the PIP axis)
- Swan neck deformity - PIP hyperextension with DIP flexion (often from volar plate laxity or intrinsic tightness)
- Extensor tendon subluxation - sagittal band rupture at the MCP → extensor tendon snaps to one side with flexion
Summary Diagram Concept
PALMAR VIEW (flexor side):
Zone V → Zone IV (carpal tunnel) → Zone III (palm) → [A1] → Zone II → [A2]──[C1]──[A3]──[C2]──[A4]──[C3]──[A5]
MCP FDS ins. Prox. Ph. PIP Mid. Ph. DIP
FDS: inserts on middle phalanx (via Camper's chiasm)
FDP: passes through FDS, inserts on distal phalanx
DORSAL VIEW (extensor side):
EDC → Sagittal bands (MCP) → Central slip (→ middle phalanx base, PIP extension)
→ Lateral bands (+ lumbrical/interossei) → Terminal tendon (→ distal phalanx, DIP extension)
Sources:
- Imaging Anatomy Text and Atlas, Vol. 3, pp. 1295-1323
- Miller's Review of Orthopaedics, 9th Ed., pp. 10040-10045
- Campbell's Operative Orthopaedics, 15th Ed. 2026, pp. 4053, 4407-4408
- Sabiston Textbook of Surgery, 21st Ed., pp. 2742-2744
- Tintinalli's Emergency Medicine, p. 1394
This is a shared conversation. Sign in to Orris to start your own chat.