Myself harish doing my clerkship rotation starting from today and my positing is in ob GYN and in that it's Labor room so what are all the things I should know and master before entering and give a brief details about topography ctg monitoring
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Searching Images
CTG cardiotocography topography fetal heart rate monitoring strip
Loading Image
Loading Image
Welcome to the labor room, Harish! Here is your comprehensive clerkship preparation guide, built from authoritative OB/GYN and maternal-fetal medicine textbooks.
🏥 Labor Room Clerkship — Complete Preparation Guide for Harish
PART 1 — THINGS TO KNOW BEFORE ENTERING THE LABOR ROOM
1. Anatomy & Physiology Essentials
| Topic | Key Points |
|---|---|
| Pelvis types | Gynecoid (ideal), Android, Anthropoid, Platypelloid — determines mode of delivery |
| Fetal skull landmarks | Occiput, bregma, anterior/posterior fontanelle, biparietal diameter (~9.5 cm at term) |
| Cervix | Effacement (softening/thinning) → Dilation (0–10 cm) → Descent of presenting part |
| Uterine blood supply | Uterine + ovarian arteries; placental blood flow ~600 mL/min at term |
2. Stages of Labour — The Backbone of the Labor Room
| Stage | Definition | Normal Duration |
|---|---|---|
| Stage 1 — Latent phase | Onset of labor → 6 cm dilation | Up to 20 hrs (nullipara) / 14 hrs (multipara) |
| Stage 1 — Active phase | 6 cm → 10 cm (full dilation) | ≥0.5–1 cm/hr; arrest >4 hrs without progress |
| Stage 2 | Full dilation → Delivery of baby | ≤3 hrs nullipara, ≤2 hrs multipara (with epidural add 1 hr each) |
| Stage 3 | Delivery of baby → Delivery of placenta | ≤30 minutes |
| Stage 4 | First 1–2 hrs post-delivery (close monitoring) | Hemorrhage risk peak period |
3. Admission Assessment Checklist
When a patient arrives in labor room, systematically assess:
History:
- Gestational age (LMP + USS dating)
- GBS (Group B Streptococcus) status — affects antibiotic prophylaxis decisions
- Prior cesarean section? (VBAC risk assessment)
- Complications: pre-eclampsia, GDM, placenta previa
- Membrane status — intact vs. ruptured (SROM/PROM)
- Contraction frequency, duration, interval
- Fetal movement felt today?
Examination:
- Vital signs (BP, pulse, temperature, SpO₂)
- Abdominal exam: Leopold's maneuvers (fetal lie, presentation, position, engagement)
- Symphysis-fundal height
- Vaginal examination (VE): cervical dilation, effacement, station (−5 to +5), position, consistency — Bishop Score
- Fetal heart rate (CTG or Pinard)
Investigations:
- Urine dipstick (protein, glucose)
- CBC, blood group & cross-match if needed
- Confirm presentation on USS if uncertain
4. Key Clinical Skills to Master
| Skill | Why it Matters |
|---|---|
| Leopold's Maneuvers (4 maneuvers) | Determine lie, presentation, position, engagement |
| Vaginal Examination | Assess labor progress using Bishop Score |
| Partograph use | Monitor labor graphically; detect arrest disorders early |
| CTG interpretation | Most important monitoring tool — see Part 2 below |
| Auscultating FHR with Pinard/Doppler | Intermittent auscultation protocol |
| Recognition of fetal distress | Category III CTG → escalate urgently |
| Active Management of 3rd Stage (AMTSL) | Oxytocin 10 IU IM + cord traction + uterine massage → prevents PPH |
| Estimating blood loss | Key in PPH identification |
| Episiotomy basics | Indications: fetal distress, shoulder dystocia, instrumental delivery |
5. Cardinal Movements of Labor (Mechanism of Labour)
These happen during vaginal delivery of a vertex-presenting fetus — memorize these:
- Engagement — Head enters pelvic inlet
- Descent — Throughout labor
- Flexion — Chin on chest; presents smallest diameter
- Internal rotation — Occiput rotates to anterior (OP → OA)
- Extension — Head delivers under pubic symphysis
- Restitution / External rotation — Head aligns with shoulders
- Expulsion — Anterior shoulder → posterior shoulder → body
6. Common Drugs Used in the Labor Room
| Drug | Use | Dose |
|---|---|---|
| Oxytocin | Labor augmentation / AMTSL | 2–5 mU/min IV infusion; 10 IU IM at delivery |
| Misoprostol | Cervical ripening / PPH | 25–50 mcg PO/SL/vaginal |
| Magnesium sulfate | Eclampsia seizure prophylaxis / neuroprotection <32 wks | Loading 4g IV → 1g/hr maintenance |
| Nifedipine / Atosiban | Tocolysis (stop preterm labor) | Nifedipine 20 mg oral |
| Betamethasone | Fetal lung maturity <34 wks | 12 mg IM × 2 doses, 24 hrs apart |
| Benzathine penicillin / Ampicillin | GBS prophylaxis | Ampicillin 2g IV loading → 1g 4-hrly |
| Fentanyl / Epidural | Labor analgesia | Per anesthesia protocol |
| Terbutaline | Intrauterine resuscitation (Cat III CTG) | 0.25 mg SC |
7. Obstetric Emergencies to Recognize Immediately
| Emergency | Key Sign | Immediate Action |
|---|---|---|
| Cord prolapse | Cord felt/seen on VE; sudden severe decels | Call for help, elevate presenting part, emergency C/S |
| Shoulder dystocia | Turtle sign after head delivery | McRoberts, suprapubic pressure, HELPERR |
| Uterine rupture | Sudden loss of FHR + maternal shock | Emergency laparotomy |
| Placental abruption | Painful bleeding + uterine rigidity | Urgent delivery + resus |
| Eclampsia | Seizure in context of hypertension/proteinuria | Airway, MgSO₄, BP control, delivery |
| PPH | Blood loss >500 mL vaginal / >1000 mL CS | Bimanual compression, uterotonics, escalate |
PART 2 — CTG MONITORING (CARDIOTOCOGRAPHY) IN DETAIL
What is CTG / Topography?
CTG (Cardiotocography) is the simultaneous, continuous electronic recording of:
- Upper channel → Fetal Heart Rate (FHR) in beats per minute
- Lower channel → Uterine Contractions (tocometry) via tocodynamometer or intrauterine pressure catheter
The term "topography" in CTG context refers to the morphological shape and pattern of the FHR tracing over time — how peaks, troughs, and the baseline are distributed topographically on the strip.
How the CTG Machine Works
"The electronic FHR monitor is a device with two components. One establishes the FHR, and the other measures uterine contractions." — Creasy & Resnik's Maternal-Fetal Medicine, p. 718
Two modes:
| Mode | Device | How it works |
|---|---|---|
| External (most common) | Doppler ultrasound transducer (cardiotachometer) | Emits ~2.5 MHz ultrasound; detects reflected signal from moving cardiac structures; interval between beats → rate (bpm) transcribed at 3 cm/min paper speed |
| Internal (more accurate) | Fetal scalp electrode (FSE) | Small spiral stainless steel wire on fetal scalp; detects R wave of fetal ECG; gives true beat-to-beat variability; requires ruptured membranes + ≥1 cm dilation |
| Uterine contractions — external | Tocodynamometer | Placed on fundus; detects frequency & duration but NOT intensity |
| Uterine contractions — internal | Intrauterine pressure catheter (IUPC) | Measures pressure in mmHg; detects frequency, duration AND intensity |
The 5 Features of CTG to Assess (DR C BRAVaDO / BRADD)
Use the BRADD or structured approach:
1. Baseline FHR
- Normal: 110–160 bpm
- Tachycardia: >160 bpm (causes: infection, fetal anemia, prematurity, maternal fever/drugs)
- Bradycardia: <110 bpm (causes: cord prolapse, maternal hypotension, abruption)
"The average FHR is 155 beats/min at 20 weeks' gestation, 144 beats/min at 30 weeks, and 140 beats/min at term. This progression reflects maturation of vagal tone." — Creasy & Resnik's Maternal-Fetal Medicine
2. Baseline Variability
Fluctuations in baseline FHR — reflects intact fetal neurological function (vagal-sympathetic balance)
| Grade | Range | Meaning |
|---|---|---|
| Absent | Undetectable | Alarming — fetal acidosis possible |
| Minimal | ≤5 bpm | Concerning |
| Moderate (Normal) | 6–25 bpm | Reassuring |
| Marked | >25 bpm | Investigate |
"FHR variability is important clinically, and its specific amplitude as part of the FHR pattern has prognostic value. The vagus nerve is responsible for transmission of impulses causing beat-to-beat variability." — Creasy & Resnik's Maternal-Fetal Medicine
3. Accelerations
- Transient rise in FHR ≥15 bpm above baseline, lasting ≥15 seconds (term)
- At <32 weeks: ≥10 bpm for ≥10 seconds
- Presence = reassuring (reactive NST)
- Absence of accelerations after fetal stimulation → Category II
4. Decelerations
This is the most critical part of CTG interpretation:
| Type | Pattern | Cause | Clinical Significance |
|---|---|---|---|
| Early | Mirror image of contraction; gradual onset + nadir at contraction peak | Fetal head compression → vagal reflex | Benign |
| Late | Begin after peak of contraction; nadir after peak; gradual onset | Uteroplacental insufficiency → fetal brain hypoxia → sympathetic activation → BP rise → baroreceptor-mediated bradycardia | Worrisome |
| Variable | Abrupt drop ≥15 bpm, ≥15 sec; variable timing/depth; V-shaped or U-shaped | Umbilical cord compression | Context-dependent; recurrent = concerning |
| Prolonged | Drop >15 bpm lasting 2–10 min | Cord prolapse, abruption, epidural hypotension | Urgent |
"Late decelerations are a result of uteroplacental insufficiency causing relative fetal brain hypoxia during a contraction... A second type is from myocardial depression in the presence of increasing hypoxia." — Miller's Anesthesia, 10e
"Variable decelerations are associated with umbilical cord compression. A sinusoidal FHR pattern is associated with fetal anemia and is considered ominous." — Miller's Anesthesia, 10e
5. Sinusoidal Pattern
- Smooth, regular, sine-wave-like oscillations 3–5 cycles/min
- Associated with severe fetal anemia (Rh disease, vasa previa)
- Ominous sign
CTG Classification — Three-Tier System (NICHD 2008)
This is the internationally used classification:
| Category | Features | Interpretation | Action |
|---|---|---|---|
| Category I (Normal) | Baseline 110–160 bpm + moderate variability + no late/variable decels + accelerations may or may not be present | Normal fetal acid-base status | Continue routine monitoring |
| Category II (Indeterminate) | Anything not Cat I or Cat III — e.g., tachycardia, minimal variability, absence of accelerations after stimulation, recurrent variables with moderate variability, prolonged decel 2–10 min | Not predictive of abnormal acid-base status | Continue monitoring; re-evaluate; consider intrauterine resuscitation |
| Category III (Abnormal) | Absent variability + recurrent late decels OR recurrent variable decels OR bradycardia OR sinusoidal pattern | Abnormal fetal acid-base status | Immediate action required |
"Category III FHR tracings require prompt patient evaluation and interventions... intrauterine resuscitation with change in maternal position, discontinuation of labor augmentation, treatment of maternal hypotension, supplemental O₂, tocolytic agent such as terbutaline. If FHR tracing does not improve, expeditious delivery." — Miller's Anesthesia, 10e
CTG Strip — What it Looks Like
Category I — Normal CTG:
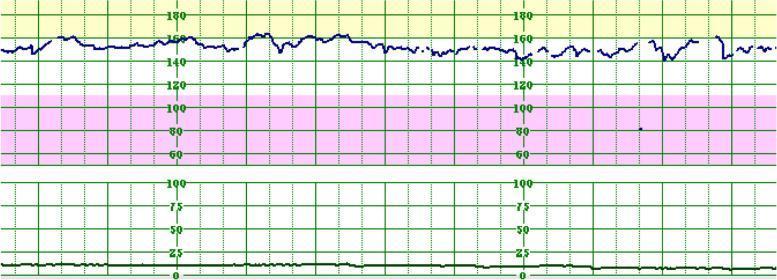
Upper trace = FHR (~150 bpm, moderate variability, no decelerations). Lower trace = uterine activity (flat = no significant contractions). This is a reassuring, Category I tracing.
Non-Reassuring CTG with Deceleration:

Upper trace = FHR showing abrupt deceleration (drop below 110 bpm) with contraction. Lower trace = uterine activity showing corresponding contraction. This pattern requires urgent assessment.
Intrauterine Resuscitation Steps (for Cat II/III)
When you see a non-reassuring CTG, act in this order:
- Reposition the mother — Left lateral decubitus (relieves aortocaval compression)
- Stop oxytocin infusion immediately
- IV fluid bolus — treat maternal hypotension (e.g., post-epidural)
- Supplemental O₂ by face mask (though evidence is evolving)
- Terbutaline 0.25 mg SC — tocolysis to stop excessive contractions
- Vaginal examination — rule out cord prolapse, assess progress
- Call your senior / prepare for delivery if no improvement
Physiological Basis of CTG (Why Decelerations Happen)
Understanding the neuroscience behind CTG makes interpretation intuitive:
- Vagus nerve (CN X) → tonic parasympathetic slowing of FHR + beat-to-beat variability
- Sympathetic nerves → tonic acceleration; released during stress/hypoxia
- Peripheral chemoreceptors (aortic/carotid bodies) → respond to ↓PO₂ / ↑PCO₂
- Baroreceptors → respond to ↑BP → reflex bradycardia (late decelerations mechanism)
- During hypoxia: vagal activity increases up to 4× → bradycardia; absent variability = CNS suppression
Quick CTG Memory Aids
Deceleration types — "EVL"
- Early = vagus (head compression) = benign
- Variable = cord compression = variable significance
- Late = uteroplacental insufficiency = ominous
Variability mnemonic — "0-5-6-25-MARK"
- 0 = Absent | ≤5 = Minimal | 6–25 = Moderate (Normal) | >25 = Marked
PART 3 — PARTOGRAPH
The partograph is a graphical tool for monitoring labor progress. Know these zones:
- Alert line — labor progress falls to this → heightened vigilance
- Action line — 4 hrs to the right of alert line → intervention required (augmentation or C/S)
- Plots: cervical dilation, fetal descent, contractions/10 min, FHR, maternal vitals, urine output, drugs
PART 4 — BEHAVIOR & SAFETY IN THE LABOR ROOM
- Always confirm identity of the patient before any procedure
- Sterile technique for VE, catheterization, any invasive procedure
- Wash hands between every patient (universal precaution)
- Never perform a VE if placenta previa is suspected without prior USS
- Document everything with time stamps — medicolegal importance
- Escalate early — "if in doubt, shout"
- Respect patient dignity at all times; ask consent before every examination
Summary Checklist for Day 1
- Know the 3 stages of labor and their duration
- Be able to do Leopold's 4 maneuvers
- Understand Bishop Score components (DECCP: Dilation, Effacement, Consistency, Cervical Position, Station)
- Read a CTG strip using the 5-feature approach
- Know Category I / II / III criteria
- Recognize the 3 types of decelerations
- Know the steps of AMTSL
- Know the first steps for Cat III CTG and cord prolapse
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice | Miller's Anesthesia, 10e | Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
Good luck in the labor room, Harish! Stay observant, ask questions, and always escalate when uncertain. 🩺
Anatomy of the labor
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
obstetric pelvis types gynecoid android anthropoid platypelloid anatomy
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.