Nerve supply of pinna,external auditory canal,middle ear, inner ear explain in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the detailed information needed. Let me compile a comprehensive answer.
Nerve Supply of the Ear - Detailed Anatomy
The sensory supply of the ear is highly complex. Four cranial nerves (V, VII, IX, X) and two cervical spinal nerves (C2, C3) all contribute. This rich, overlapping innervation is clinically important - it explains why referred otalgia from distant sites (TMJ, pharynx, larynx, thyroid) is so common.
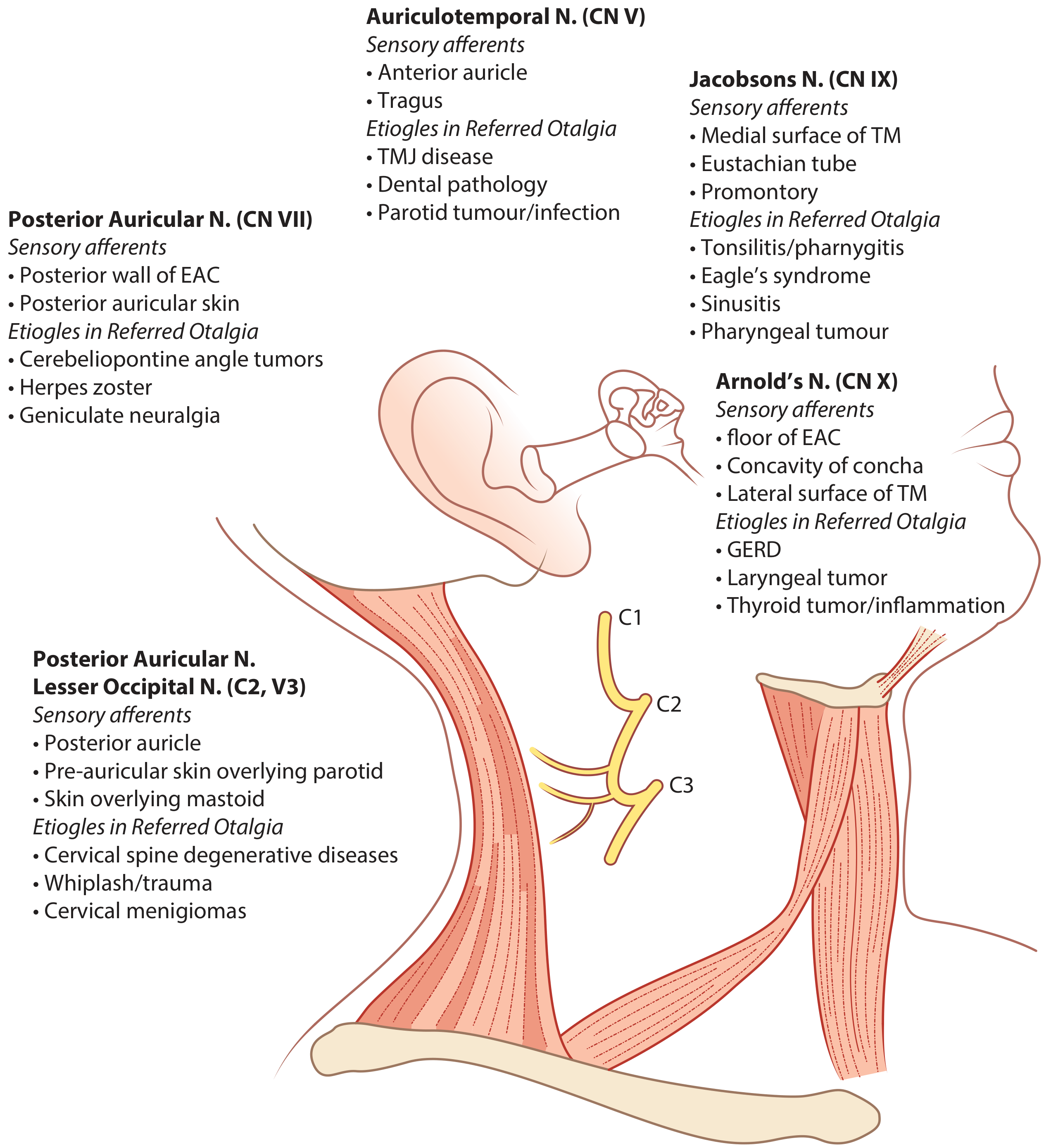
1. PINNA (Auricle)
The pinna receives innervation from both cranial branchial nerves and somatic cervical nerves. Their distribution is heterogeneous with considerable overlap.
Table: Sensory Innervation of the Auricle
| Nerve | Derivation | Region Supplied |
|---|---|---|
| Greater auricular nerve | Cervical plexus C2, C3 | Medial (cranial) surface entire; posterior portion of lateral surface - the dominant nerve of the auricle |
| Lesser occipital nerve | Cervical plexus C2, C3 | Superior portion of the medial surface |
| Auriculotemporal nerve | Mandibular division of trigeminal (V3) | Tragus, crus of helix, adjacent helix; lateral skin of pinna above the level of the external meatus |
| Auricular branch of vagus (Arnold's nerve, CN X) | Vagus nerve CN X | Concha and antihelix; small area of medial surface (eminentia conchae) |
| Facial nerve (CN VII) | CN VII | Small region at the root of the concha (sparse contribution, roughly overlapping with vagus territory) |
Key points:
- The greater auricular nerve prevails on both the lateral and medial surfaces and is the most important sensory nerve of the pinna overall
- The lesser occipital nerve contributes mainly to the superior portion of the medial (cranial) surface
- CN V3 (auriculotemporal) supplies the anterior/lateral upper pinna, especially tragus and helix crus
- The motor supply to the extrinsic auricular muscles (auricularis anterior, superior, posterior) comes from the temporal and posterior auricular branches of the facial nerve (CN VII)
2. EXTERNAL AUDITORY CANAL (EAC)
The EAC receives sensory innervation from four nerves: trigeminal (V), facial (VII), glossopharyngeal (IX), and vagus (X).
Nerve by nerve:
1. Auriculotemporal nerve (CN V3 - mandibular division of trigeminal)
- Supplies the anterior and superior walls of the EAC
- Also supplies the anterosuperior quadrant of the tympanic membrane (outer surface)
2. Auricular branch of the vagus - Arnold's nerve (CN X)
- Supplies the posterior and inferior meatal skin (floor and posterior wall of EAC)
- Also supplies the posteroinferior quadrant of the tympanic membrane (outer surface)
- Clinically important: stimulation of Arnold's nerve during microsuction or syringing of the EAC triggers the ear-cough reflex (reflex cough via vagal stimulation) and can also cause vomiting/bradycardia (Arnold's reflex)
3. Facial nerve (CN VII) - posterior auricular branch
- Supplies the posterior wall of the EAC (contribution overlaps with vagus)
- Small cutaneous area behind the ear and the posterior meatal wall
4. Tympanic branch of glossopharyngeal (Jacobson's nerve, CN IX)
- Minor contribution to the deep EAC skin
5. Greater auricular nerve (C2, C3)
- Contributes to the skin over the concha and lower part of the external meatus
3. MIDDLE EAR
The middle ear (tympanic cavity, Eustachian tube, mastoid air cells) is supplied primarily via the tympanic plexus.
Tympanic Membrane Innervation
The tympanic membrane has a dual innervation (outer surface and inner surface are supplied differently):
- Outer (lateral/epidermal) surface: Auriculotemporal nerve (V3) anterosuperiorly + Auricular branch of vagus (Arnold's nerve, X) posteroinferiorly
- Inner (medial/mucosal) surface: Tympanic branch of glossopharyngeal (Jacobson's nerve, CN IX) via the tympanic plexus
Branches from the lamina propria allow the two sources to interconnect through anastomoses. Innervation is relatively sparse in the middle part of the posterior half of the tympanic membrane.
Tympanic Plexus (Main Middle Ear Supply)
The tympanic plexus lies on the promontory (the rounded bulge on the medial wall of the tympanic cavity) and innervates the mucous membrane of the entire middle ear cleft, including the tympanic cavity walls, Eustachian tube, mastoid antrum, and mastoid air cells.
Formed by:
- Tympanic nerve (Jacobson's nerve) - branch of CN IX (glossopharyngeal)
- Leaves CN IX at the inferior (petrous) ganglion after it exits the jugular foramen
- Passes through the tympanic canaliculus (in the keel of petrous bone between the jugular and carotid foramina)
- Enters the middle ear and ramifies on the promontory
- Caroticotympanic nerves - sympathetic branches from the internal carotid plexus (superior cervical ganglion)
From the tympanic plexus arise:
- Sensory branches to the mucosa of tympanic cavity, mastoid, and Eustachian tube
- Lesser petrosal nerve - carries preganglionic parasympathetic fibers (from the inferior salivatory nucleus via CN IX) through the petrous temporal bone to the otic ganglion, where they synapse and supply the parotid gland
Middle Ear Muscles
| Muscle | Nerve Supply |
|---|---|
| Tensor tympani | Branch from the mandibular nerve (V3) via the nerve to medial pterygoid |
| Stapedius | Branch of the facial nerve (CN VII) - tympanic segment |
4. INNER EAR
The inner ear is supplied primarily by CN VIII (vestibulocochlear nerve), which divides into two functional divisions inside the internal acoustic meatus.
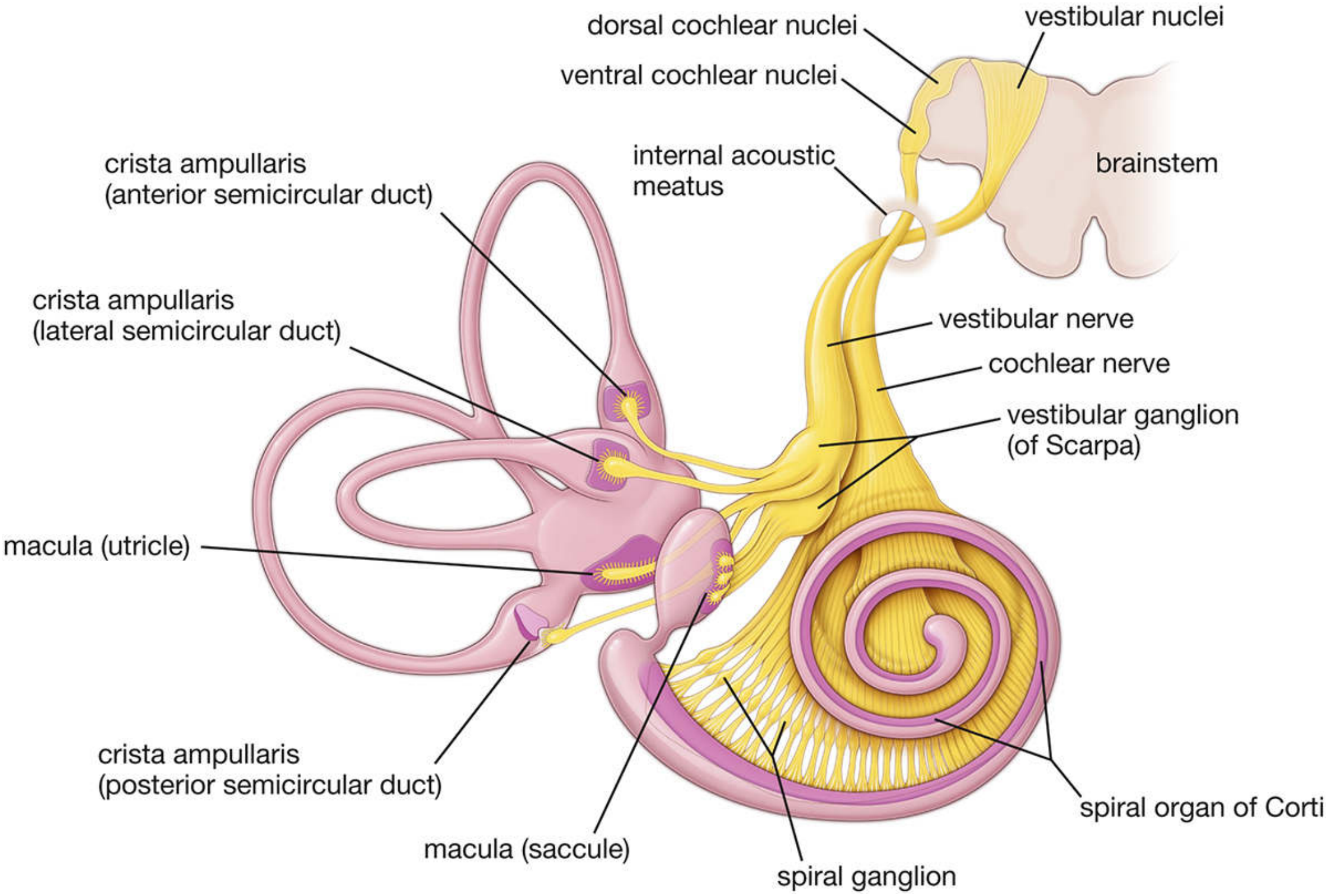
A. Cochlear Nerve (Hearing)
- Arises from bipolar neurons whose cell bodies are in the spiral ganglion of Corti (located in the modiolus, the central bony axis of the cochlea)
- Dendritic processes: exit the modiolus through tiny openings in the bony spiral lamina and synapse on hair cells in the organ of Corti
- ~90% of dendrites synapse with inner hair cells
- ~10% synapse with outer hair cells
- Axons of spiral ganglion cells form the cochlear nerve → travels through internal acoustic meatus → enters brainstem → terminates in the cochlear nuclei (dorsal and ventral) of the medulla
- From cochlear nuclei → lateral lemniscus → inferior colliculus → medial geniculate nucleus of thalamus → auditory cortex of temporal lobe (Heschl's gyri)
Efferent fibers (olivocochlear tract of Rasmussen): A small number of efferent fibers from the superior olivary complex travel parallel to the afferent fibers. They synapse on afferent nerve endings below inner hair cells or directly on outer hair cells. Their role is modulation/suppression of auditory input.
B. Vestibular Nerve (Balance)
- Arises from bipolar neurons whose cell bodies are in the vestibular ganglion (of Scarpa) in the internal acoustic meatus
- Dendritic processes originate in:
- Cristae ampullares of the three semicircular ducts (anterior, posterior, lateral) - detect angular/rotational acceleration
- Macula of the utricle - detects linear horizontal acceleration and static head position
- Macula of the saccule - detects linear vertical acceleration
- They synapse at the base of type I hair cells (as a chalice ending) or as boutons on type II hair cells
- Axons → form the vestibular nerve → internal acoustic meatus → brainstem → terminate in the four vestibular nuclei (superior, inferior, medial, lateral) of the pons/medulla
- Secondary fibers go to: the cerebellum, and the nuclei of CN III, IV, VI (for vestibulo-ocular reflex)
Blood/Nerve Supply to the Internal Ear
- The labyrinthine artery (internal auditory artery), usually a branch of the anterior inferior cerebellar artery (AICA) or basilar artery, accompanies CN VIII through the internal acoustic meatus
- The inner ear has no pain fibers - hence inner ear pathology (Meniere's disease, acoustic neuroma) does not produce local ear pain but may cause referred otalgia via CN IX/X connections
Clinical Relevance Summary
| Structure | Key Nerve | Clinical Significance |
|---|---|---|
| Pinna (cranial surface) | Greater auricular (C2,3) | Cervical spine pathology → referred auricular pain |
| Anterior pinna/tragus | Auriculotemporal (V3) | TMJ disease, dental pathology → referred otalgia |
| EAC posterior wall | Arnold's nerve (X) | Ear syringing/microsuction → reflex cough, vomiting, bradycardia |
| TM outer surface post | Arnold's nerve (X) | GERD, laryngeal/thyroid tumors → referred otalgia |
| Middle ear mucosa | Tympanic plexus (IX) | Tonsilitis, pharyngeal tumor → referred otalgia |
| Stapedius | Facial nerve (VII) | Facial nerve palsy → hyperacusis (loss of stapedius reflex) |
| Inner ear | CN VIII | Acoustic neuroma at CPA angle - hearing loss + vertigo |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 (Chapters 46, 92); Gray's Anatomy for Students (Chapter 8); K.J. Lee's Essential Otolaryngology (Chapter 4); Histology: A Text and Atlas (Chapter 25)
This is a shared conversation. Sign in to Orris to start your own chat.