What is the difference between functional and organic lesions in valvular heart diseases?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-cited answer.
Functional vs. Organic Lesions in Valvular Heart Disease
This distinction is one of the most clinically important in cardiology because it determines prognosis, guides treatment decisions, and defines whether the valve itself or the surrounding cardiac structures are the primary problem.
Core Definition
| Feature | Organic (Primary) Lesion | Functional (Secondary) Lesion |
|---|---|---|
| Valve itself | Structurally abnormal | Structurally normal |
| Problem origin | Intrinsic disease of leaflets, chordae, annulus, or subvalvular apparatus | Abnormality in non-valvular components — myocardium, ventricular geometry, atrial dilation |
| Also called | Primary valvular disease | Secondary valvular disease |
| Treating the valve | Cures or substantially helps the patient | Does not reverse the underlying disease |
"In primary mitral regurgitation, treating the mitral regurgitation cures the patient. Conversely, secondary mitral regurgitation is typically a consequence of left ventricular dysfunction… Because treating secondary mitral regurgitation cannot reverse those entities, the role of valve therapy is often unclear." — Goldman-Cecil Medicine, 26e
Organic Lesions — Key Features
The valve leaflets, chordae tendineae, papillary muscles, or annulus are intrinsically diseased. Common causes include:
- Myxomatous degeneration / mitral valve prolapse — redundant, prolapsing, or flail leaflets with chordal elongation or rupture (most common cause of primary MR in developed countries)
- Rheumatic heart disease — leaflet thickening, commissural fusion, chordal shortening
- Infective endocarditis — leaflet perforation or destruction
- Connective tissue disorders (Marfan, Ehlers-Danlos)
- Congenital anomalies — cleft mitral valve, bicuspid aortic valve
- Infiltrative/fibrotic processes — carcinoid syndrome, radiation-induced, drug-induced (fenfluramine, ergotamine)
- Degenerative calcification of the annulus
Miller's Anesthesia, 10e states: "Primary or 'organic' mitral valve disease involves abnormalities in the valve itself or in its subvalvular structural components."
Functional Lesions — Key Features
The valve leaflets are morphologically normal, but regurgitation results from geometric distortion of the surrounding cardiac apparatus. The two main mechanisms are:
- Leaflet tethering/restriction — ventricular dilatation and remodeling displaces the papillary muscles outward and apically, tethering the leaflets and preventing coaptation (restricted leaflet motion — Carpentier type IIIb)
- Annular dilatation — the annular circumference exceeds the area covered by the leaflets, causing malcoaptation without leaflet pathology (Carpentier type I); seen especially with atrial fibrillation
"In secondary mitral regurgitation, the valve itself is normal. Regurgitation occurs because of leaflet malcoaptation that results from either displacement of the papillary muscles in patients with left ventricular dysfunction or annular dilatation in patients with atrial fibrillation." — Goldman-Cecil Medicine
Common causes of functional lesions:
- Ischemic cardiomyopathy / prior MI — most common cause of functional MR (~10–20% of CAD patients)
- Dilated cardiomyopathy
- Atrial fibrillation with progressive annular dilation
- Pulmonary hypertension / right heart failure → functional tricuspid regurgitation (TR)
- Any cause of right ventricular or left ventricular remodeling
The Carpentier Classification — A Unified Framework
Carpentier's classification of leaflet motion applies to both concepts:
| Type | Leaflet Motion | Example |
|---|---|---|
| Type I | Normal motion | Functional MR from annular dilation (e.g., AF) |
| Type II | Excessive motion (prolapse/flail) | Organic MR — chordal rupture, myxomatous disease |
| Type IIIa | Restricted motion in systole AND diastole | Organic — rheumatic disease |
| Type IIIb | Restricted motion in systole only | Functional MR — ischemic/dilated cardiomyopathy (papillary muscle tethering) |
Functional MR is classically Carpentier IIIb (or a combination of I + IIIb), while organic MR spans Types II and IIIa. — Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery
Functional Tricuspid Regurgitation — A Key Example
Functional (secondary) TR is the most common form of tricuspid regurgitation. The tricuspid valve leaflets are normal; regurgitation results from:
- Tricuspid annular (TA) dilation — driven mainly by right atrial enlargement (typical in chronic atrial fibrillation)
- Papillary muscle displacement — from RV remodeling due to pulmonary hypertension
The figure below illustrates both mechanisms:
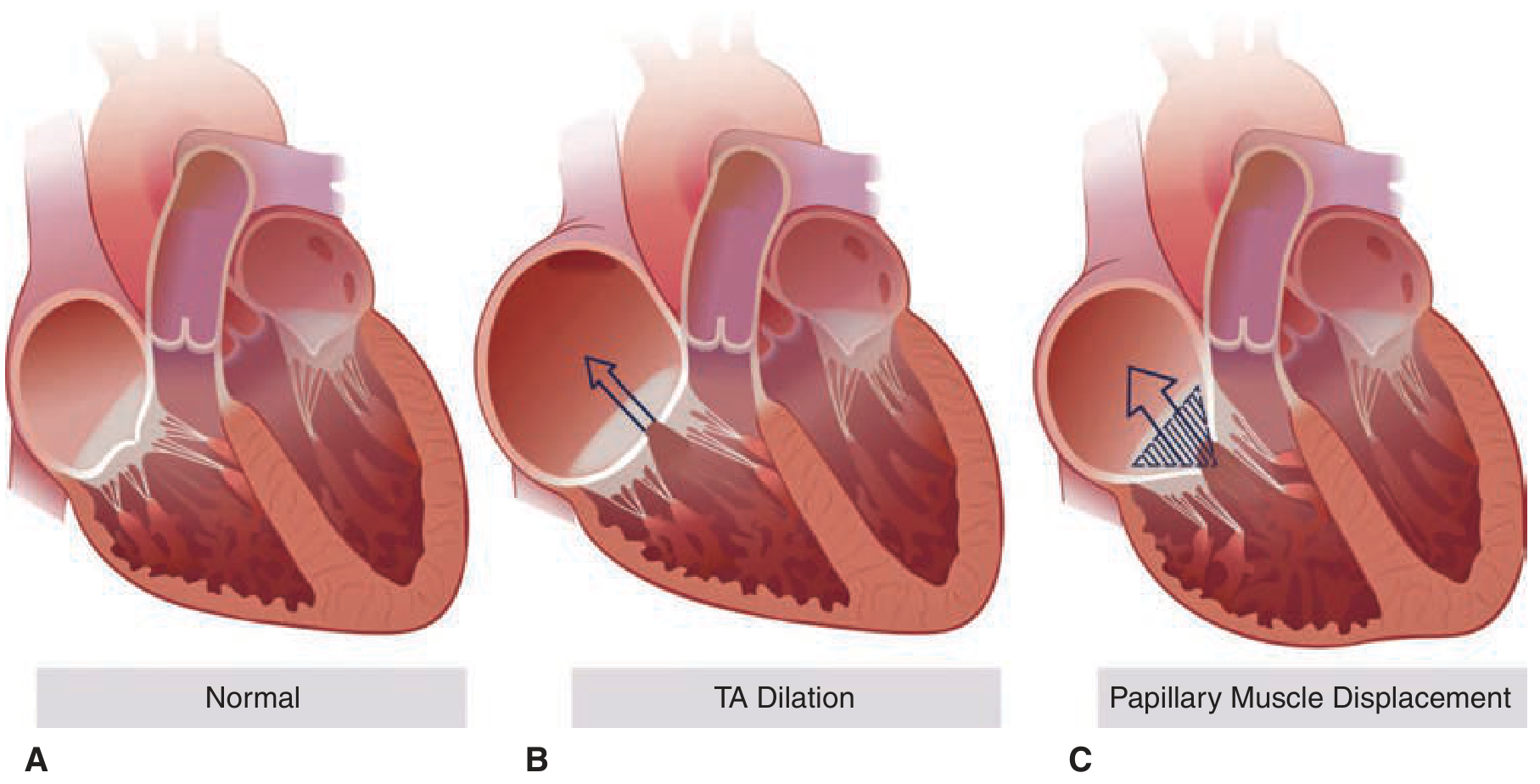
Causes include: pulmonary hypertension, RV cardiomyopathy, left-sided heart valve diseases, heart failure, and atrial fibrillation. — Fuster & Hurst's The Heart, 15e
Clinical Implications
| Clinical Aspect | Organic | Functional |
|---|---|---|
| Murmur intensity | Often loud, well-heard | May be soft or absent (weakened contraction, normal valve) |
| Echocardiography | Shows structural leaflet/apparatus abnormality | Shows normal leaflets with geometric distortion of ventricle/annulus |
| Surgical decision | Valve repair/replacement is primary therapy | Valve intervention alone is insufficient; underlying disease (heart failure, ischemia) must be treated |
| Reversibility | Valve repair can be curative | Secondary MR may improve with treatment of underlying LV dysfunction (e.g., CRT, revascularization, HF therapy) |
| Prognosis | Related to valve lesion severity | Reflects severity of underlying cardiomyopathy |
"Chronic ischemic or functional MR is present in 10% to 20% of patients with CAD and, unlike MR with primary valvular causes, it does not involve abnormalities in the morphology of the mitral valve." — Miller's Anesthesia, 10e
Mixed Lesions
In practice, organic and functional components often coexist. For example, rheumatic disease causing leaflet thickening (organic) may also produce annular and LV dilation (adding a functional component). Fuster & Hurst notes this is common in multivalvular disease in older patients. — Fuster & Hurst's The Heart, 15e
Sources: Goldman-Cecil Medicine, 26e | Miller's Anesthesia, 10e | Fuster & Hurst's The Heart, 15e | Braunwald's Heart Disease, 12e | Schwartz's Principles of Surgery, 11e
This is a shared conversation. Sign in to Orris to start your own chat.