PA 2.1 Describe the causes, mechanisms, types and effects of cell injury and their clinical significance PA 2.2 Describe the etiology of cell injury. Distinguish between reversible-irreversible injury: mechanisms; morphology of cell injury PA 2.3 Describe morphological changes in intracellular accumulation of fats, proteins, carbohydrates, pigments Mujhe ye saari competency detail me samjhao flowchart,tables,bullets ke saath Reference robbins pathology and harshmohan
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed. Let me compile the comprehensive answer.
PA 2.1 / 2.2 / 2.3 - Cell Injury: Complete Study Notes
Reference: Robbins & Cotran Pathologic Basis of Disease (10th Ed.) + Robbins Basic Pathology
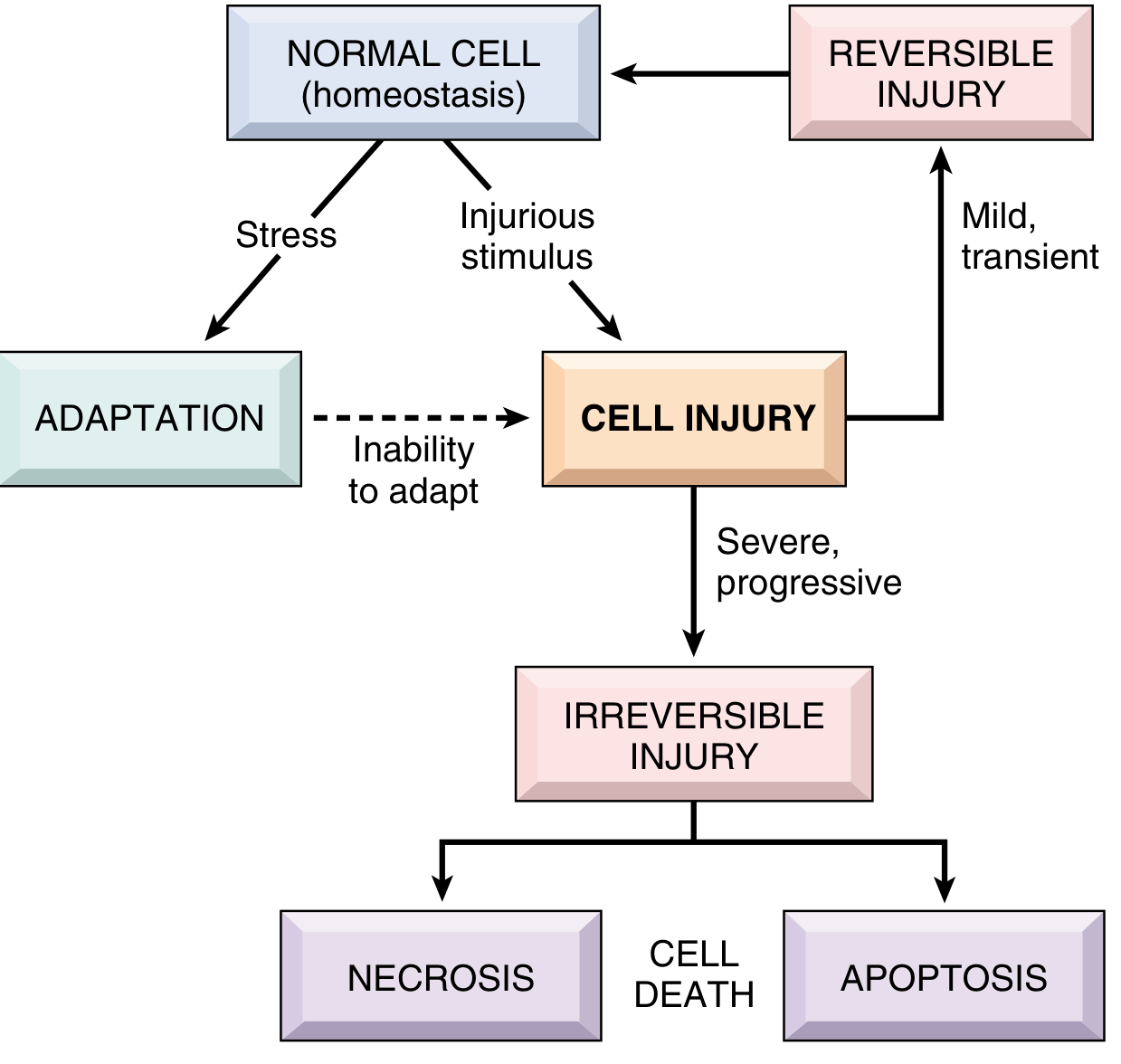
OVERVIEW FLOWCHART
PA 2.1 - CAUSES, MECHANISMS, TYPES AND EFFECTS OF CELL INJURY
A. CAUSES OF CELL INJURY
CAUSES OF CELL INJURY
│
├── 1. Hypoxia & Ischemia ─── Most common cause
│ ├── Ischemia (blocked artery)
│ ├── Cardiorespiratory failure
│ ├── Anemia / CO poisoning
│
├── 2. Physical Agents
│ ├── Mechanical trauma
│ ├── Extremes of temperature (burns, frostbite)
│ ├── Radiation
│ └── Electric shock
│
├── 3. Chemical Agents & Drugs
│ ├── Hypertonic glucose/salt
│ ├── O2 (toxic at high conc.)
│ ├── Arsenic, cyanide, mercury
│ ├── Alcohol, cocaine
│ └── Therapeutic drugs (dose-dependent)
│
├── 4. Infectious Agents
│ ├── Viruses, bacteria, fungi
│ ├── Parasites (tapeworms, etc.)
│ └── Mechanisms: toxins, immune response
│
├── 5. Immunologic Reactions
│ ├── Autoimmune disease
│ ├── Allergic reactions
│ └── Chronic immune responses → inflammation → cell injury
│
├── 6. Genetic Abnormalities
│ ├── Extra chromosome (e.g., Down syndrome)
│ ├── Single base substitution (e.g., Sickle cell)
│ ├── Enzyme defects (inborn errors of metabolism)
│ └── DNA damage / misfolded proteins → apoptosis
│
└── 7. Nutritional Imbalances
├── Protein-calorie deficiency (PEM)
├── Specific vitamin deficiencies
└── Obesity → DM2, atherosclerosis
B. MECHANISMS OF CELL INJURY
Key Biochemical Mechanisms (Table)
| Mechanism | What Happens | Example |
|---|---|---|
| ATP Depletion | Na-K ATPase pump fails → cell swelling; anaerobic glycolysis → lactic acidosis | Ischemia |
| Mitochondrial Damage | Loss of oxidative phosphorylation; cytochrome c release → apoptosis | Toxins, radiation |
| Ca²+ Influx | Activates phospholipases, proteases, endonucleases, ATPases → membrane & DNA damage | Ischemia, toxins |
| Oxidative Stress (ROS) | Free radicals damage lipid membranes (peroxidation), proteins, DNA | Reperfusion, radiation, drugs |
| Membrane Permeability Defects | Lysosomal membrane damage → enzymatic digestion of cell | Ischemia, toxins |
| DNA Damage | Direct or via ROS; triggers p53 → apoptosis if irreparable | Radiation, chemotherapy |
| Protein Misfolding (ER stress) | Unfolded protein response (UPR) activated; if overwhelmed → apoptosis | α1-antitrypsin deficiency |
Integrated Stress Response (ISR)
- Activated by hypoxia, infection, nutrient starvation, misfolded proteins
- Four kinases phosphorylate eIF2α → reduces protein synthesis → adapts cell
- If stress persists → triggers apoptosis
C. TYPES OF CELL INJURY
CELL INJURY
│
├── REVERSIBLE INJURY ───── Mild / transient stimulus
│ ├── Cell can recover if stimulus removed
│ └── → Returns to normal
│
└── IRREVERSIBLE INJURY ─── Severe / persistent stimulus
├── "Point of no return" crossed
├── Defined by:
│ ├── Inability to reverse mitochondrial dysfunction
│ └── Profound membrane damage
└── → CELL DEATH
├── NECROSIS (pathologic)
└── APOPTOSIS (physiologic or pathologic)
[+newer: necroptosis, pyroptosis, ferroptosis]
D. EFFECTS / CLINICAL SIGNIFICANCE
| Type | Effect | Clinical Example |
|---|---|---|
| Reversible injury | Cellular swelling, fatty change | Hepatic steatosis in alcoholism |
| Necrosis | Tissue death, inflammation | MI, renal infarct, TB (caseous necrosis) |
| Apoptosis | Silent cell death, no inflammation | Embryogenesis, AIDS, cancer chemotherapy |
| Cell death biomarkers | Proteins leak into blood | Troponin in MI (detectable within 2 hrs); ALT/AST in hepatitis |
| Necroptosis | Regulated necrosis | Viral infections |
| Pyroptosis | Inflammatory cell death | Bacterial infections |
PA 2.2 - REVERSIBLE vs IRREVERSIBLE INJURY
Sequential Development of Changes
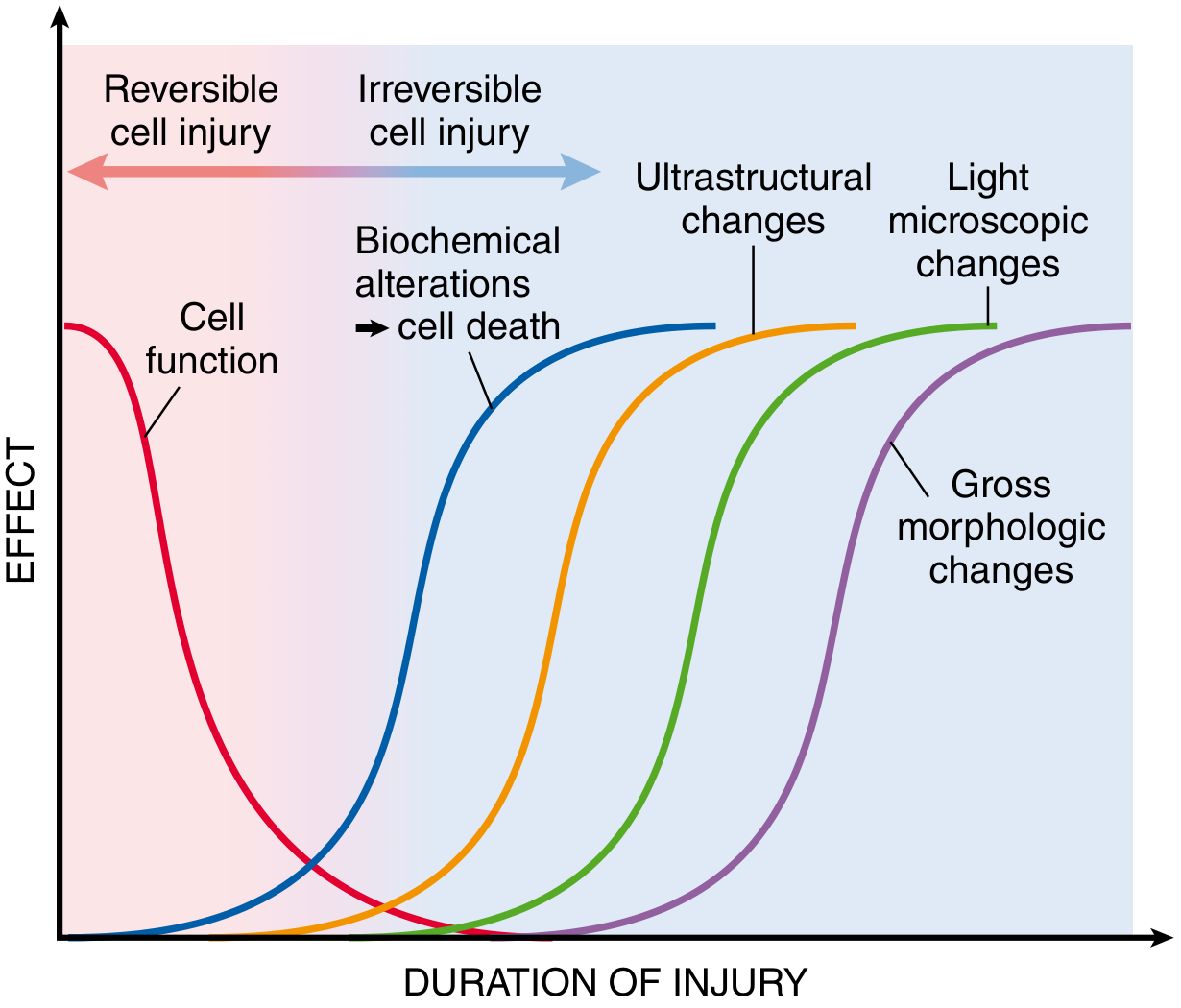
Key concept: Morphological changes LAG behind biochemical alterations. Cell function is lost FIRST.
- In myocardial ischemia: swelling = minutes; light microscope evidence = 4-12 hours
Comparison Table: Reversible vs Irreversible Injury
| Feature | Reversible Injury | Irreversible Injury (Necrosis) |
|---|---|---|
| Stimulus | Mild, transient | Severe, persistent |
| Outcome | Cell recovers | Cell death |
| ATP | Reduced (some remaining) | Severely depleted |
| Mitochondria | Swollen (reversible) | Large amorphous densities, irreversibly damaged |
| Plasma membrane | Blebbing (intact) | Disrupted, ruptured |
| Nucleus | Normal to clumped chromatin | Pyknosis → karyorrhexis → karyolysis |
| ER | Dilated | Fragmented |
| Ribosomes | Detached from ER | Disaggregated |
| Cytoplasm | Swollen, vacuolated | Eosinophilic, moth-eaten |
| Inflammation | None | YES (hallmark of necrosis) |
Morphology of Reversible Cell Injury
Two consistent features (Robbins):
- Cellular swelling - due to failure of ATP-dependent Na⁺-K⁺ pump → water influx → organelles swell
- Fatty change - toxic injury disrupts lipid metabolism → triglyceride-filled vacuoles (mainly in liver)
Other changes visible:
- Plasma membrane blebbing and loss of microvilli
- Mitochondrial swelling (no amorphous densities)
- ER dilation with detachment of ribosomes
- Clumping of nuclear chromatin
- Eosinophilia (↓ cytoplasmic RNA)
Morphology of Irreversible Injury - NECROSIS
Cellular Changes
- Eosinophilia - loss of RNA + denatured proteins bind eosin
- Vacuolated, moth-eaten cytoplasm - digested organelles
- Myelin figures - whorled phospholipid precipitates (phagocytosed or calcified)
Nuclear Changes (3 Patterns)
NUCLEAR CHANGES IN NECROSIS
│
├── 1. PYKNOSIS ─── Nuclear shrinkage + increased basophilia (chromatin condensation)
│
├── 2. KARYORRHEXIS ─── Pyknotic nucleus fragments into pieces
│
└── 3. KARYOLYSIS ─── Chromatin basophilia FADES due to DNase degradation
(Nucleus eventually disappears in 1-2 days)
Patterns of Tissue Necrosis (High-Yield Table)
| Pattern | Mechanism | Gross Appearance | Classic Example |
|---|---|---|---|
| Coagulative | Denaturation of proteins preserves cell outline; hypoxia stops enzyme activity | Firm, pale infarct | Myocardial infarction, renal infarct |
| Liquefactive | Enzymatic digestion liquefies tissue (lots of enzymes/neutrophils) | Pus/fluid-filled cavity | Brain infarct, bacterial abscess |
| Caseous | Coagulative + liquefactive; structureless granular debris | Cheese-like, white | TB (tuberculosis) |
| Fat necrosis | Lipase releases fatty acids → bind Ca²+ (saponification) | Chalky white deposits | Acute pancreatitis |
| Fibrinoid | Antigen-antibody complexes + fibrin deposited in vessel walls | Pink smudgy vessel walls | Malignant hypertension, vasculitis |
| Gangrenous | Ischemic coagulative + superimposed infection | Dry (coagulative) or Wet (liquefactive) | Diabetic foot, bowel ischemia |
Apoptosis vs Necrosis (Comparative Table)
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Cause | Pathologic | Physiologic or pathologic |
| Cell size | Swollen | Shrunken |
| Nucleus | Pyknosis/karyolysis | Fragmentation into nucleosome-sized pieces |
| Plasma membrane | Disrupted | Intact (forms apoptotic bodies) |
| Cellular contents | Leaked | Retained in apoptotic bodies |
| Inflammation | YES - intense | NO |
| ATP | Depleted | Required |
| Example | MI, infarct | Embryogenesis, lymphocyte culling |
PA 2.3 - INTRACELLULAR ACCUMULATIONS
Overview: 4 Mechanisms of Accumulation
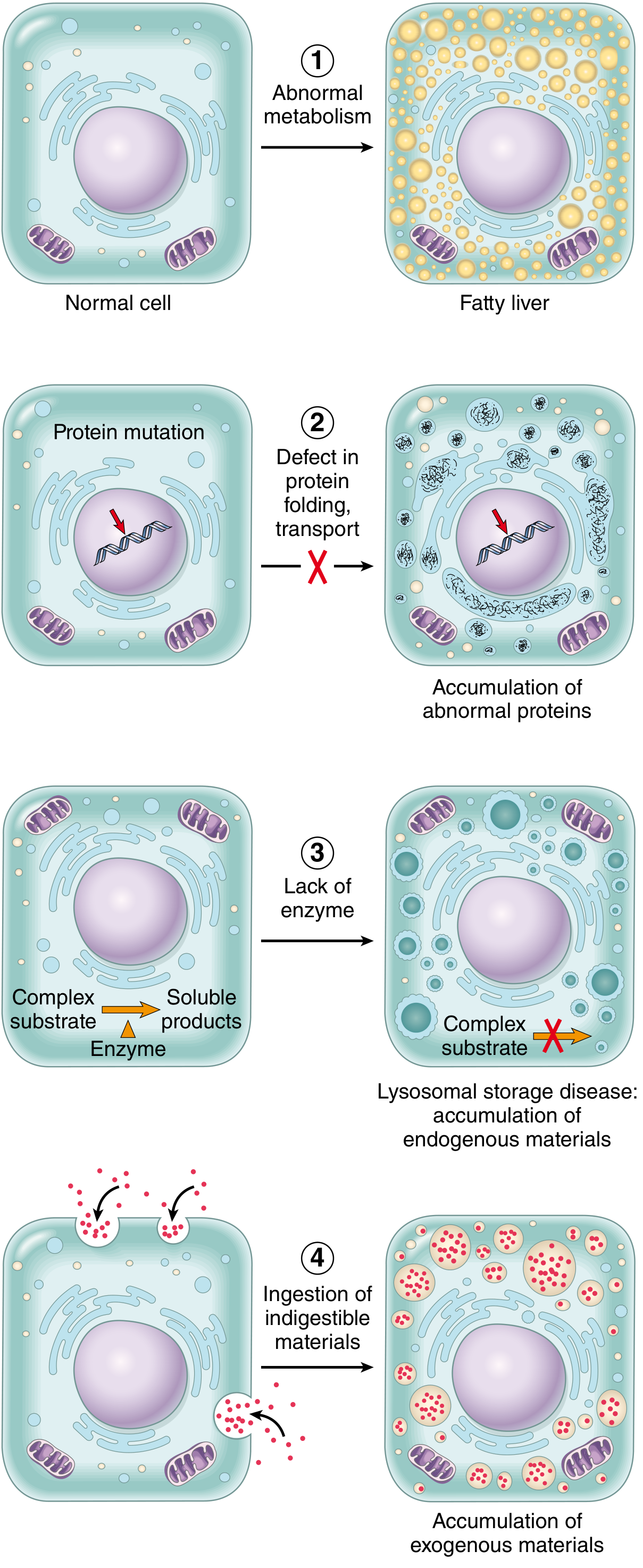
MECHANISMS OF INTRACELLULAR ACCUMULATION
│
├── 1. INADEQUATE REMOVAL of normal substance
│ (defects in production/transport)
│ Example: Fatty liver (steatosis)
│
├── 2. ACCUMULATION due to defect in folding/transport/secretion
│ Example: α1-antitrypsin deficiency (builds up in ER of hepatocytes)
│
├── 3. FAILURE TO DEGRADE - inherited enzyme deficiency
│ Example: Lysosomal storage diseases (Gaucher's, Tay-Sachs)
│
└── 4. DEPOSITION OF ABNORMAL EXOGENOUS SUBSTANCE
Cell has no enzyme to degrade it
Example: Carbon (coal dust), silica particles
A. FAT ACCUMULATION (Steatosis / Fatty Change)
Sites
- Liver (most common - major organ of fat metabolism)
- Heart, skeletal muscle, kidney (less common)
Causes (Mnemonic: DATO AN)
- D - Diabetes mellitus
- A - Alcohol (most common in high-income countries)
- T - Toxins
- O - Obesity / NAFLD
- A - Anoxia
- N - Nutritional deficiency (protein malnutrition)
Mechanism (Liver Fatty Change)
Normal liver fat metabolism:
FFA → Triglycerides → bound to Apoprotein → Lipoprotein → EXPORTED
Fatty change occurs when ANY step is disrupted:
├── ↑ FFA delivery (obesity, DM, starvation)
├── ↓ β-oxidation of FA (hypoxia, toxins like CCl4)
├── ↑ FA esterification to TG (alcohol)
├── ↓ Apoprotein synthesis (CCl4, protein malnutrition)
└── ↓ Lipoprotein secretion (alcohol, CCl4)
Morphology
- Gross: Liver is enlarged, yellow, greasy
- Light microscopy: Clear lipid vacuoles in cytoplasm (triglyceride washed out in processing)
- Small droplets initially (microvesicular) - nucleus central
- Large droplets later (macrovesicular) - nucleus pushed to periphery
- Special stain: Oil Red O stains fat red in frozen sections
Cholesterol Accumulation
| Condition | Cells Involved | Appearance |
|---|---|---|
| Atherosclerosis | Smooth muscle cells + macrophages in intima | Foam cells (lipid vacuoles), cholesterol clefts |
| Xanthomas | Macrophages in skin/tendons | Foamy macrophage clusters |
| Cholesterolosis | Macrophages in gallbladder lamina propria | Focal foam cell clusters |
| Niemann-Pick disease type C | Multiple organs | Lysosomal storage disease |
B. PROTEIN ACCUMULATION
Types and Examples
| Type | Mechanism | Example | Morphology |
|---|---|---|---|
| Reabsorption droplets | ↑ protein reabsorption via pinocytosis | Nephrotic syndrome (heavy proteinuria) | Pink hyaline cytoplasmic droplets in proximal tubule; REVERSIBLE |
| Russell bodies | ↑ Ig synthesis in plasma cells → accumulate in RER | Multiple myeloma, chronic inflammation | Large rounded eosinophilic inclusions |
| Defective transport/secretion | Misfolded protein accumulates in ER | α1-antitrypsin deficiency | PAS+ globules in hepatocyte ER → emphysema (loss of function) |
| Alcoholic hyaline (Mallory bodies) | Accumulated keratin intermediate filaments | Alcoholic liver disease | Eosinophilic cytoplasmic inclusions in hepatocytes |
| Neurofibrillary tangles | Accumulated neurofilaments + tau | Alzheimer disease | In neurons of brain |
C. CARBOHYDRATE (GLYCOGEN) ACCUMULATION
Causes
- Diabetes mellitus - abnormal glucose metabolism
- Sites: renal tubular epithelium, liver, cardiac myocytes, beta cells of islets
- Glycogen storage diseases (Glycogenoses) - inherited enzyme defects
- e.g., Pompe (acid maltase deficiency), McArdle (muscle phosphorylase)
Morphology
- Light microscopy: Clear vacuoles in cytoplasm (glycogen dissolves in aqueous fixatives)
- Best identified: Fixed in absolute alcohol (not formalin)
- Special stains:
- PAS (Periodic Acid-Schiff): Rose-to-violet color
- Best carmine: Confirms glycogen
- Diastase digestion: Serial section treated with diastase - glycogen disappears (confirms it IS glycogen, not mucin)
D. PIGMENT ACCUMULATION
Classification Flowchart
PIGMENTS
│
├── EXOGENOUS (from outside body)
│ ├── Carbon (coal dust) ─────── Most common exogenous pigment
│ │ ├── Inhaled → phagocytosed by alveolar macrophages
│ │ ├── → lymphatics → tracheobronchial lymph nodes (blackened)
│ │ └── Anthracosis (lungs); Coal worker's pneumoconiosis
│ └── Tattoo pigments ─── Indigestible, remain in dermal macrophages lifelong
│
└── ENDOGENOUS (synthesized in body)
│
├── LIPOFUSCIN ("wear-and-tear" pigment)
│ ├── Composition: polymers of lipids + phospholipids + protein
│ ├── Origin: lipid peroxidation of polyunsaturated lipids (free radical injury)
│ ├── Appearance: yellow-brown, finely granular, perinuclear
│ ├── Significance: telltale sign of free radical damage; NOT injurious itself
│ └── Seen in: aging liver, heart; cancer cachexia; malnutrition
│
├── MELANIN
│ ├── Brown-black, endogenous
│ ├── Formed by: Tyrosinase → tyrosine → DOPA → melanin (in melanocytes)
│ └── Only endogenous brown-black pigment
│
├── HEMOSIDERIN (iron-containing)
│ ├── Derived from ferritin aggregates (haemoglobin breakdown)
│ ├── Golden-yellow to brown granules
│ ├── Stain: Prussian blue (stains blue)
│ ├── Local: old hemorrhage site (e.g., bruise turning brown)
│ └── Systemic: hereditary hemochromatosis, transfusion hemosiderosis
│
└── BILIRUBIN
├── Normal bile pigment; product of Hb catabolism
├── Accumulates in jaundice
└── Stain: Van Gieson, Hall's bile stain
SUMMARY TABLE: Intracellular Accumulations (High-Yield for Exams)
| Substance | Disease/Condition | Special Stain | Key Feature |
|---|---|---|---|
| Triglycerides | Alcoholic liver, NAFLD, DM | Oil Red O (frozen section) | Clear vacuoles, macrovesicular/microvesicular |
| Cholesterol | Atherosclerosis, xanthoma | - | Foam cells, cholesterol clefts |
| Protein droplets | Nephrotic syndrome | H&E (pink hyaline) | Proximal tubule; reversible |
| Russell bodies | Myeloma, chronic inflammation | H&E (eosinophilic) | Distended RER in plasma cells |
| α1-antitrypsin | α1-antitrypsin deficiency | PAS+ | Hepatocyte ER; → emphysema |
| Glycogen | DM, glycogenoses | PAS + Best carmine; diastase labile | Clear vacuoles; abs. alcohol fixation |
| Lipofuscin | Aging, cachexia | Yellow-brown on H&E (autofluorescent) | Perinuclear; free radical marker |
| Hemosiderin | Hemochromatosis, hemorrhage | Prussian blue | Golden-brown granules |
| Melanin | Melanoma, Addison's | Masson-Fontana | Brown-black |
| Carbon | Anthracosis, pneumoconiosis | Black, H&E | Alveolar macrophages, lymph nodes |
CLINICAL SIGNIFICANCE SUMMARY
| Injury Type | Clinical Marker | Disease |
|---|---|---|
| Myocardial necrosis | Cardiac Troponin T/I (2 hrs); CK-MB | MI |
| Hepatocyte necrosis | ALT, AST | Hepatitis |
| Bile duct injury | Alkaline phosphatase (ALP) | Cholestasis |
| Pancreatic necrosis | Serum amylase/lipase | Pancreatitis |
| Fatty liver | Liver biopsy + steatosis on imaging | Alcoholic liver, NAFLD |
| Glycogen storage | ↑ glycogen on biopsy, enzyme assay | Pompe, McArdle disease |
| Carbon accumulation | CXR: bilateral reticulonodular opacities | Pneumoconiosis |
Reference:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, 10th Ed. - Chapter 2: Cell Injury, Cell Death, and Adaptations (pp. 47-80)
- Robbins & Kumar - Basic Pathology - Chapter 1: Cell Injury and Death
This is a shared conversation. Sign in to Orris to start your own chat.