Simulation of upper esophagus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Here is a comprehensive overview of the simulation of the upper esophagus - meaning its anatomy, physiology, and functional behavior as a segment of the GI tract.
Simulation of the Upper Esophagus
Overview
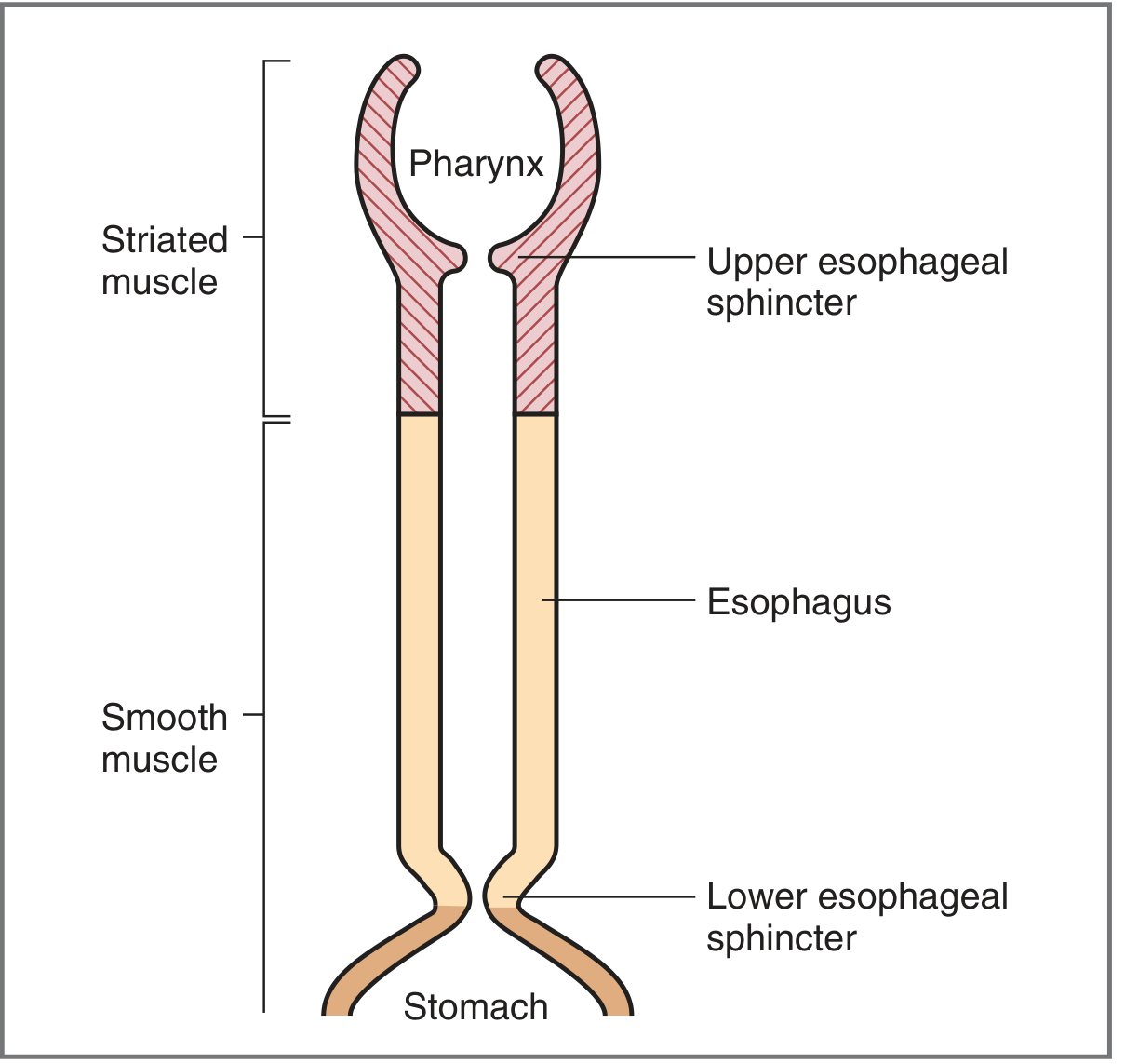
The esophagus extends from the cricoid cartilage to the cardia of the stomach (~16 cm from incisors to the cricopharyngeal sphincter; 38-40 cm to the stomach in adults). It is divided into three functional segments: the upper esophageal sphincter (UES), the esophageal body (cervical + thoracic + intra-abdominal), and the lower esophageal sphincter (LES). The lumen is approximately 20 mm in diameter.
Structural Anatomy
Wall Layers (proximal to deep)
- Mucosa - stratified squamous epithelium, lamina propria, muscularis mucosae
- Submucosa - connective tissue, blood/lymphatics, Meissner (submucosal) plexus
- Muscularis propria - inner circular + Auerbach (myenteric) plexus + outer longitudinal muscle
- No serosa - unlike most of the GI tract (clinically important: perforations spread freely)
Musculature Transition
| Segment | Muscle Type |
|---|---|
| Upper third (cervical esophagus) | Striated (skeletal) muscle |
| Middle esophagus | Mixed (transitional zone) |
| Lower two-thirds (thoracic) | Smooth muscle |
Specifically, the upper 5-33% is exclusively skeletal, and the distal 50% is exclusively smooth, with a mixed transition zone in between. - Sleisenger & Fordtran's GI and Liver Disease
Upper Esophageal Sphincter (UES)
- Formed by the lowermost fibers of the inferior constrictor muscle (cricopharyngeus)
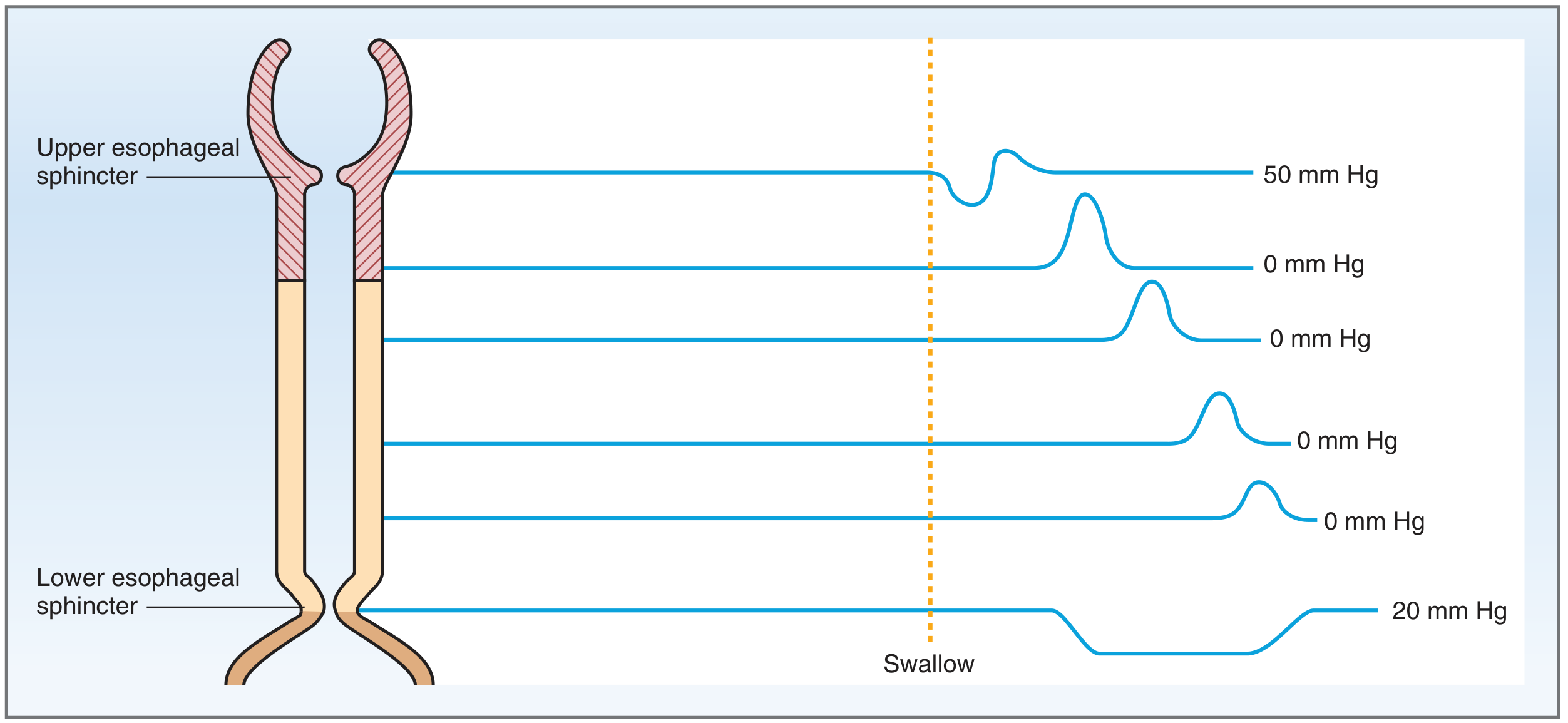
- Tonically contracted at rest - creates a high-pressure zone (~50 mmHg) that prevents inspired air from entering the esophagus and prevents esophageal reflux into the pharynx
- Relaxes during swallowing, actively dilated by laryngeal elevation during deglutition
- Composed of striated muscle (4th, 5th, and 6th branchial arches)
- Innervated by the vagus nerve and recurrent laryngeal nerve
Innervation of the Upper Esophagus
This is what makes the upper esophagus uniquely different from the rest of the GI tract:
- Parasympathetics (vagus nerve) regulate peristalsis in the esophagus
- Cell bodies in the medulla split into two functional populations:
- Nucleus ambiguus → controls striated muscle (upper esophagus)
- Dorsal motor nucleus of vagus → controls smooth muscle (lower esophagus)
- Medullary vagal postganglionic efferent fibers terminate directly at motor endplates of skeletal muscle in the upper esophagus (no intermediate ganglion)
- In contrast, fibers to smooth muscle are preganglionic and synapse on Auerbach plexus neurons
Key concept: Motor programs for the upper (striated muscle) esophagus are located in the medulla oblongata, relayed via the nucleus ambiguus. If vagal innervation is severed, propulsion in the striated segment fails permanently and does not recover - unlike the lower smooth muscle segment which retains some ENS function. - Yamada's Textbook of Gastroenterology, 7th ed.
Blood Supply
| Segment | Artery |
|---|---|
| Upper third | Inferior thyroid artery |
| Middle third | Thoracic aorta |
| Lower third | Left gastric + inferior phrenic arteries |
Venous drainage: upper esophagus → inferior thyroid veins (systemic). The lower esophagus drains to portal circulation via left gastric vein - this creates the portosystemic anastomosis responsible for varices in portal hypertension.
Physiology: Swallowing and Peristalsis
Swallowing is divided into 3 phases:
1. Oral Phase (voluntary)
- Tongue pushes bolus posteriorly into pharynx
- Activates somatosensory receptors in pharynx
- Triggers involuntary swallowing reflex in medullary swallowing center
2. Pharyngeal Phase (reflex)
- Soft palate elevates - seals nasopharynx
- Epiglottis covers laryngeal inlet; larynx elevates
- UES relaxes - opens passage from pharynx to esophagus
- Peristaltic wave initiated in pharynx propels bolus through open UES
- Respiration is briefly inhibited
3. Esophageal Phase
- The upper third (striated muscle) has the most rapid peristalsis - transit time less than 1 second
- The lower two-thirds (smooth muscle) transit takes approximately 3 seconds
- Gravity plays only a minor role; swallowing works normally regardless of body position
Primary peristalsis = physiologic sequential constriction and shortening
Secondary peristalsis = non-physiologic retrograde peristalsis
Tertiary peristalsis = non-physiologic segmental contraction without forward propulsion
Secondary peristalsis = non-physiologic retrograde peristalsis
Tertiary peristalsis = non-physiologic segmental contraction without forward propulsion
Pressure Profile During Swallowing
Clinical Correlates of the Upper Esophagus
| Condition | Mechanism |
|---|---|
| Transit dysphagia | Motility disorder of the striated-muscle segment (pharynx/upper esophagus) |
| Zenker's diverticulum | Pulsion diverticulum at the Killian's triangle (above cricopharyngeus); underlying striated-muscle motility disorder |
| Killian-Jamieson diverticula | Below the UES; associated with cervical esophageal striated muscle motility disorder |
| Cricopharyngeal bar | Failure of UES relaxation / incomplete opening |
| Foreign body lodgment | Upper esophagus is the most common site; smooth objects (coins) can be removed with Foley catheter or bougienage |
| Brainstem stroke | Disrupts nucleus ambiguus → pharyngeal/upper esophageal dysphagia |
Sources:
- Costanzo Physiology, 7th Edition - Swallowing section, p. 355
- K.J. Lee's Essential Otolaryngology - Anatomy and Physiology of the Esophagus, p. 671
- Sleisenger & Fordtran's GI and Liver Disease - Esophageal anatomy and innervation
- Yamada's Textbook of Gastroenterology, 7th ed. - The Esophagus, p. 283
- Goldman-Cecil Medicine - Normal Anatomy and Physiology
Ct Simulation of Upper esophagus in cancer
Finding Sources
Finding Sources
Searching the Web
CT simulation upper esophageal cancer radiation therapy planning positioning protocol
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12283517
Searching PubMed
CT simulation esophageal cancer radiotherapy planning target volume
Finding Sources
Searching PubMed
esophageal cancer radiotherapy target volume contouring guidelines
Searching the Web
upper esophageal cancer CT sim patient positioning arms down 5-point mask OAR organs at risk contour
Reading Web Page
https://www.astro.org/ASTRO/media/ASTRO/AffiliatePages/arro/…
Finding Sources
I now have comprehensive data from multiple authoritative sources. Here is a detailed, structured answer:
CT Simulation for Upper Esophageal Cancer - Radiation Therapy Planning
CT simulation is the foundational step in radiation therapy planning for upper esophageal cancer. It establishes the patient's treatment position, generates the 3D dataset used for target volume delineation and dose calculation, and sets the geometric reference for all subsequent treatment fractions.
1. Anatomic Segmentation of the Esophagus (Relevant Context)
Before simulation, the treating oncologist must confirm the tumor's location:
| Segment | Distance from Incisors |
|---|---|
| Cervical esophagus | 15-18 cm (cricopharyngeus to thoracic inlet) |
| Upper thoracic esophagus | 18-24 cm (thoracic inlet to carina) |
| Middle thoracic esophagus | 24-32 cm (carina to inferior pulmonary veins) |
| Lower thoracic esophagus | 32-40 cm (to GEJ) |
Upper esophageal tumors include both cervical and upper thoracic lesions, each with different simulation setups and nodal drainage patterns.
2. Pre-Simulation Workup
Before CT sim, the following imaging is needed to define the GTV:
- Endoscopy - defines proximal/distal mucosal extent; endoscopic clips can be placed at tumor margins (especially for superficial tumors not visible on CT) - clip placement should be followed immediately by CT sim
- Endoscopic ultrasound (EUS) - depth of invasion (T stage)
- Contrast-enhanced CT chest/abdomen/pelvis - defines nodal involvement, invasion of adjacent structures
- FDG-PET/CT - strongly recommended; improves positive predictive value for lymph node metastasis vs. CT alone. PET improves detection of nodal disease and occult metastases. If FDG-PET/CT is obtained in the treatment position, the CT from this scan can serve as the planning CT
- Chromoendoscopy - essential for SCC; look for synchronous lesions
3. Patient Preparation for CT Simulation
| Factor | Upper Esophagus Protocol |
|---|---|
| Fasting | NPO 2 hours before sim; 200 mL liquid 30 min before scan (to standardize stomach filling) |
| Note for upper tumors | Stomach preparation may have minimal impact on cervical/upper 1/3 tumors, but the same protocol should be repeated consistently at every treatment fraction |
4. Patient Positioning and Immobilization
This is the most critical and location-dependent step. Positioning for upper esophageal cancer differs significantly from lower esophageal cancer:
For Cervical and Upper 1/3 Esophageal Tumors:
- Position: Supine
- Arms: Arms DOWN by the side (not raised above head)
- Rationale: Proximity to the neck/thoracic inlet; arms-down allows thermoplastic shell/mask immobilization of the head and neck region
- Knee support: Yes
- Immobilization device: 5-point thermoplastic shell (head, neck, shoulders) or equivalent - this provides rigid immobilization of the cervical region and prevents rotational errors
- A vacuum cushion/alpha cradle can supplement
For Middle/Lower 1/3 and GOJ Tumors (contrast):
- Arms above head (to maximize beam entry angles and spare lung)
- Vacuum cushion or thermoplastic device
Key clinical point: The arms-down + 5-point shell combination is specific to cervical/upper esophageal lesions because these tumors are treated with head-and-neck style field arrangements, and the thermoplastic mask provides the reproducibility needed for precise daily setup. - West Midlands Cancer Alliance Radiotherapy Protocol
5. CT Simulation Imaging Parameters
| Parameter | Specification |
|---|---|
| Scan extent | Skull base (includes both lungs) to below the liver; from cricoid cartilage inferiorly through entire liver volume |
| Slice thickness | ≤3 mm (contiguous slices, no gaps) |
| Breathing technique | Free-breathing 3DCT for cervical/upper/middle esophagus |
| 4DCT | NOT recommended for proximal (cervical, upper, and middle 1/3) tumors - motion is minimal at this level. Reserve 4DCT for distal (lower 1/3 and GOJ) tumors |
| IV contrast | Optional if a diagnostic contrast CT was recently done; use contrast to delineate major vessels and tumor extent |
| Oral contrast | Generally NOT recommended; may be considered in selected patients at clinician's discretion |
| HU calibration | Scanner must be calibrated - HU to mass/electron density (photon) or HU to stopping power (proton) |
| PET/CT at sim | Strongly encouraged in treatment position if available; can replace the planning CT |
| FOV | Must include all anatomy in the beam paths - no patient anatomy excluded |
6. Motion Assessment
Motion assessment during simulation is mandatory for all patients to account for tumor and nodal excursion with respiration:
- For upper esophageal tumors: respiratory motion is small; 3DCT free-breathing is adequate
- Established ITV margins from 4DCT data (primarily from lower esophagus studies): ~0.8 cm A-P and lateral, ~1.8 cm cranio-caudal for 95% coverage - apply conservatively to upper lesions
7. Target Volume Delineation
GTV (Gross Tumor Volume)
GTV-primary (GTVp):
- Delineated on the planning CT using multimodality correlation (endoscopy, CT, PET, EUS, fluoroscopy)
- Reference landmarks used: tracheal carina and aortic arch
- Superficial tumors invisible on CT: use endoscopically placed metallic clips at proximal and distal tumor margins
- GTV encompasses all disease visible on any single imaging modality (CT, PET, or EUS)
GTV-lymph node (GTVn):
- Any pathologically involved regional lymph node by imaging criteria
CTV (Clinical Target Volume)
CTV-primary:
- Pathological studies show a 30 mm margin covers 94% of microscopic invasion
- Standard: GTV-primary + 2-4 cm cranio-caudal margin along the esophageal axis
- Radial expansion: 1.0-1.5 cm circumferential
- The entire circumference of the esophageal wall is included throughout the CTV length
For upper esophageal/cervical tumors specifically (from JASTRO 2024 guidelines):
| Primary Site | High-risk nodal stations (Group 1) | Intermediate-risk (Group 2) |
|---|---|---|
| Cervical esophagus | 101 (cervical paraesophageal), 106rec (recurrent laryngeal nerve nodes) | 102, 104, 105 |
| Upper thoracic esophagus | 101, 105, 106rec | 104, 106tbL, 107, 108, 109 |
CTV-lymph node: Metastatic nodes = GTV-lymph node with 0 mm margin. If extracapsular invasion suspected: +5 mm.
CTV editing rules (apply regardless of segment):
- Crop off: vertebral bone, trachea/bronchi, aorta, lung (structures where direct invasion is unlikely)
- For posterior margin: sculpt to the anterior border of the vertebral body (5 mm posterior growth)
- For upper tumors: include peri-esophageal nodal regions in the superior mediastinum
ITV (Internal Target Volume)
- CTV-primary + CTV-lymph node ± elective nodal CTV is adjusted for respiratory motion
- For upper esophagus: motion is small; ITV-CTV margin is minimal on standard free-breathing CT
PTV (Planning Target Volume)
Typical margins added to ITV/CTV to create PTV:
| Direction | Setup Margin |
|---|---|
| Lateral | ~0.5-1.0 cm |
| Anteroposterior | ~0.5-1.0 cm |
| Cranio-caudal | ~1.0 cm |
(These assume daily CBCT-based image guidance for position verification)
Dose prescription (standard concurrent chemoradiation, definitive intent):
- PTV initial phase: 45-50.4 Gy in 1.8 Gy/fraction (25-28 fx)
- Boost PTV: GTVp + GTVn with 0.5-1.0 cm expansion → 50.4-66 Gy
- West Midlands protocol (SCOPE): 66 Gy in 33 fractions (simultaneous integrated boost to PTV66 primary and PTV66 node)
8. Organs at Risk (OAR) - Upper Esophagus Specific
| OAR | Relevance for Upper Esophageal Tumors |
|---|---|
| Spinal cord | Primary dose-limiting structure; PRV = spinal cord + 5 mm |
| Lungs (bilateral) | Mean lung dose constraint critical |
| Heart | Less prominent for upper lesions vs. mid/lower |
| Trachea/Larynx | Proximity to cervical esophagus; laryngeal function preservation |
| Thyroid gland | In field for cervical esophagus tumors |
| Brachial plexus | Relevant for upper thoracic/cervical tumors |
| Carotid arteries | Bilateral; contour for late toxicity reporting |
9. Treatment Technique
- IMRT/VMAT: Preferred for upper esophageal tumors - superior OAR sparing vs. 3DCRT given proximity to spinal cord, lungs, larynx
- Coplanar or non-coplanar beams: Non-coplanar encouraged for complex geometries to improve conformity
- Beam angles: Avoid tangential approach to moving organs (chest wall, heart)
- Image guidance: Daily CBCT for position verification is standard
- Concurrent chemotherapy: Carboplatin/paclitaxel (CROSS regimen) or cisplatin/5-FU; given concurrently during radiation
10. Summary Workflow
Pre-sim workup (endoscopy + EUS + CT + PET)
↓
Patient NPO 2 hrs → 200 mL liquid 30 min before
↓
Supine, arms DOWN, knee support, 5-point thermoplastic shell
↓
3DCT free-breathing, ≤3 mm slices, skull base to liver
± IV contrast; PET/CT in treatment position if available
↓
GTV-p delineation (CT + PET + endoscopy clips)
↓
CTV: GTV + 2-4 cm sup/inf + 1-1.5 cm radial + elective nodes
↓
PTV: CTV + 0.5-1.0 cm margins (CBCT-verified daily)
↓
IMRT/VMAT planning with OAR constraints
↓
Concurrent chemotherapy + radiation
Sources:
- JASTRO 2024 Radiotherapy Planning Guidelines for Esophageal Cancer (PMC12283517)
- West Midlands Cancer Alliance Radiotherapy Upper GI Protocol
- NRG Oncology Esophageal Cancer Protocol Template
- ASTRO ARRO Case: Esophageal Cancer (RTOG 1010 target volume definitions)
- Sleisenger & Fordtran's GI and Liver Disease - Esophageal anatomy and innervation
This is a shared conversation. Sign in to Orris to start your own chat.