Bainbridge reflex and Basal geris reflex.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
Basal Geris reflex physiology cardiovascular
Loading Image
Reading File
I now have comprehensive information on both reflexes. "Basal Geris reflex" is almost certainly the Bezold-Jarisch reflex - a well-known phonetic corruption used in some exam settings. Here is a thorough answer:
Bainbridge Reflex
Definition
The Bainbridge reflex is the tachycardia (increase in heart rate) caused by an increase in venous return / atrial stretch (increased blood volume). It is also called the atrial volume reflex or atrial stretch reflex.
Receptor (Afferent Limb)
- Low-pressure stretch receptors (mechanoreceptors / B-fibers) located in the right atrial wall and the cavoatrial junction (the junction of great veins with the right atrium).
- Increased blood volume → increased right-sided filling pressure → stretching of these receptors.
Afferent Pathway
- Signals travel via vagal afferent fibers (CN X) to the cardiovascular center in the medulla oblongata.
Efferent Pathway
- Efferent signals travel back through both vagal (parasympathetic) and sympathetic nerves to the SA node.
- Net effect: inhibition of parasympathetic tone (primary) + sympathetic stimulation → increased heart rate.
- There is also a direct stretch effect on the SA node itself (accounts for ~15% heart rate increase).
Response
- Increases heart rate up to 75% (particularly when baseline heart rate is slow).
- An additional 40-60% increase comes from the reflex arc (Bainbridge reflex proper).
- The reflex saturates - effect is greatest when baseline heart rate is slow; at fast baseline rates, atrial stretch may instead slow the heart via baroreceptor activation.
- Effect is limited to heart rate (chronotropy) - effects on contractility/stroke volume are insignificant.
Functional Significance
- Acts as a counterbalance to the baroreceptor reflex in heart rate control.
- During volume loading: Bainbridge reflex dominates → tachycardia.
- During volume depletion: High-pressure baroreceptor reflex dominates → also causes tachycardia (via different mechanism).
- Prevents damming of blood in the veins, atria, and pulmonary circulation.
- Works in concert with the Frank-Starling mechanism and baroreceptor reflex to regulate cardiac output.
Diagram
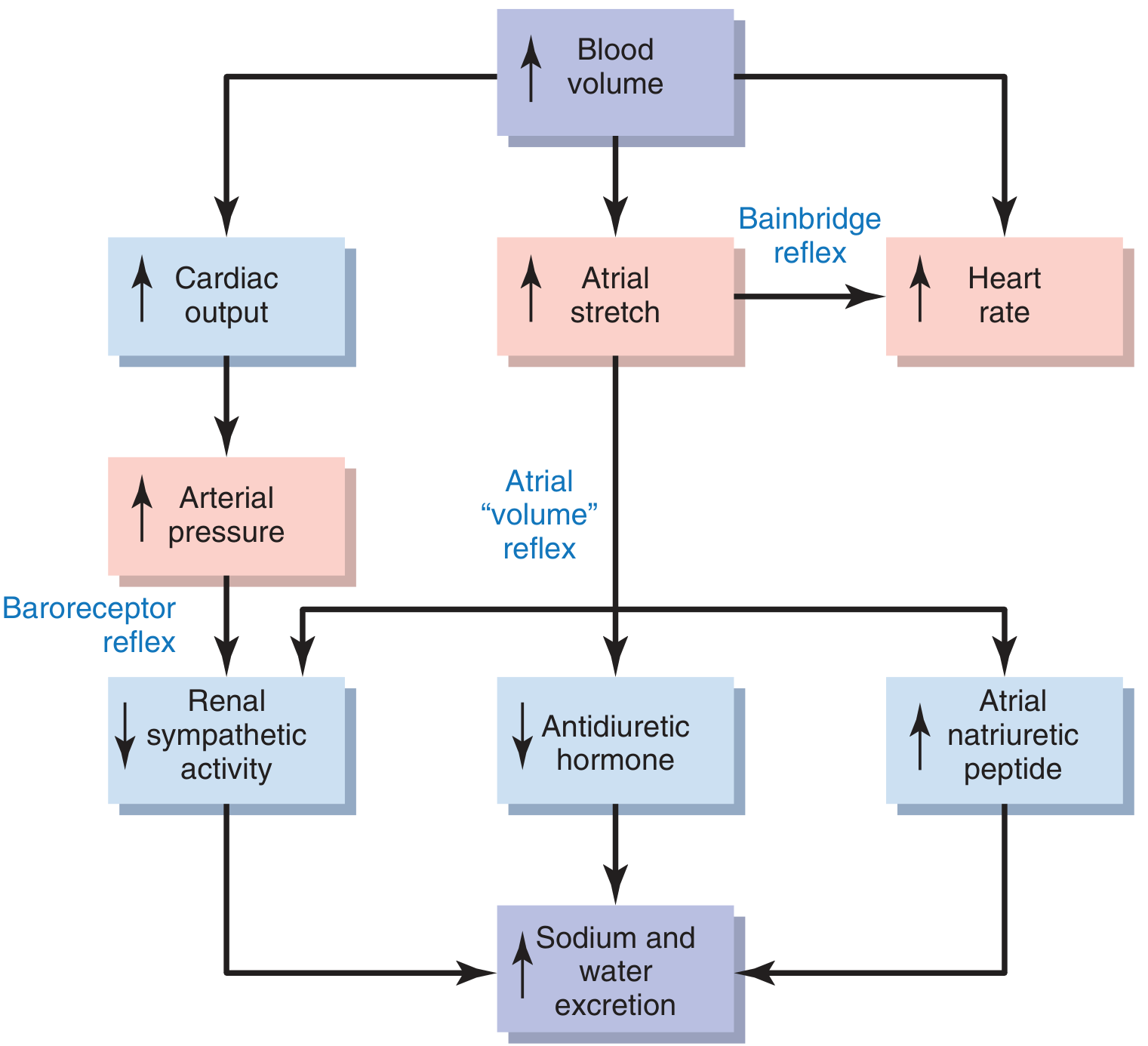
The diagram shows how increased blood volume causes atrial stretch, which via the Bainbridge reflex increases heart rate, while also triggering the volume reflex (reducing ADH, increasing ANP, reducing renal sympathetic activity) to restore volume homeostasis. - Guyton & Hall, p. 230
Bezold-Jarisch Reflex ("Basal Geris" Reflex)
Note: "Basal Geris reflex" does not appear in any standard medical textbook. This is almost certainly a phonetic misrepresentation of the Bezold-Jarisch reflex, a term commonly misspelled in regional exam notes. The correct name is Bezold-Jarisch.
Definition
The Bezold-Jarisch reflex is a cardioprotective reflex triggered by noxious stimuli in the ventricle, producing a triad of:
- Bradycardia
- Hypotension
- Coronary artery dilatation
Receptor (Afferent Limb)
- Chemoreceptors and mechanoreceptors (vagal C-fibers / juxtacapillary receptors) located in the left ventricular wall (and also in atria, great veins, pulmonary artery, alveolar capillary regions).
- These are unmyelinated type C fibers.
Stimuli That Activate the Reflex
- Noxious chemical/mechanical ventricular stimuli
- Capsaicin, serotonin, veratridine, phenylbiguanide
- Myocardial ischemia and infarction
- Thrombolysis or coronary reperfusion/revascularization
- Radiocontrast agents used in coronary angiography
- Oxygen radicals during ischemia-reperfusion
- Hypovolemia with vigorous cardiac contraction (vasovagal syncope mechanism)
Afferent Pathway
- Unmyelinated vagal afferent C-fibers → cardiovascular center in the medulla.
Efferent Pathway
- Reflexively increases parasympathetic (vagal) tone → bradycardia + hypotension.
- Simultaneously causes coronary artery dilatation.
Response
| Feature | Effect |
|---|---|
| Heart rate | Bradycardia (can drop to 20-30 bpm in humans) |
| Blood pressure | Hypotension |
| Respiration | Brief apnea followed by rapid shallow breathing |
| Coronary arteries | Dilatation |
Functional Significance
- Considered cardioprotective - the bradycardia reduces myocardial oxygen demand during ischemia.
- Implicated in the pathophysiology of vasovagal syncope: prolonged upright posture → venous pooling → reduced intracardiac volume → vigorous contraction of the near-empty ventricle → C-fiber activation → paradoxical bradycardia + hypotension → syncope.
- Modulated by ANP/BNP (natriuretic peptides); may be less pronounced in cardiac hypertrophy or atrial fibrillation.
- May also function as a defense mechanism limiting absorption of inhaled toxins.
Quick Comparison Table
| Feature | Bainbridge Reflex | Bezold-Jarisch Reflex |
|---|---|---|
| Location of receptors | Right atrium / cavoatrial junction | Left ventricular wall (C-fibers) |
| Trigger | Atrial stretch (increased venous return) | Noxious ventricular stimuli, ischemia, chemicals |
| Afferent | Vagal (myelinated B-fibers) | Vagal (unmyelinated C-fibers) |
| Heart rate effect | Tachycardia | Bradycardia |
| Blood pressure | May increase (via increased CO) | Hypotension |
| Net purpose | Prevent venous congestion; match CO to venous return | Cardioprotection; may cause vasovagal syncope |
| Clinical relevance | Exercise physiology, fluid loading | MI, vasovagal syncope, anesthesia, angiography |
Sources: Guyton & Hall Textbook of Medical Physiology, p. 230 | Miller's Anesthesia 10e | Ganong's Review of Medical Physiology 26e | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.