BONE HEALING in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bone healing" OR "fracture healing" mechanisms
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative sources. Let me compile the full detailed answer:
Bone Healing - A Detailed Guide
Sources: Rockwood & Green's Fractures in Adults (10th ed, 2025), Campbell's Operative Orthopaedics (15th ed, 2026), Bailey & Love's Short Practice of Surgery (28th ed), Miller's Review of Orthopaedics (9th ed)
Overview
Bone is one of the few tissues in the body capable of true regeneration - restoring the original structure rather than just forming a scar. Fracture healing is a complex, interdependent cascade involving inflammation, repair, and remodeling that requires the recruitment of appropriate cells (fibroblasts, macrophages, chondroblasts, osteoblasts, osteoclasts) and expression of appropriate genes at the right time and anatomic location. The two broad types are natural (indirect/secondary) bone healing and primary (direct) bone healing, determined largely by the mechanical environment at the fracture site.
- Rockwood & Green's Fractures in Adults, 10th ed, 2025
Types of Bone Healing
1. Natural (Indirect / Secondary) Bone Healing
This is the most common form. It occurs when there is controlled interfragmentary motion (a "relatively stable" environment) - seen with cast immobilization, intramedullary nails, external fixators, or flexible plate constructs. The fracture heals by bridging with a callus envelope rather than direct remodeling across the bone ends.
2. Primary (Direct) Bone Healing
Occurs only when there is absolute stability with anatomic reduction and compression. Requires:
- Interfragmentary motion < 0.15 mm
- Fracture strain < 2-5%
- No gap between fracture ends
It occurs by osteoclast cutting cones crossing adjacent fracture surfaces, followed by osteoblasts forming new bone. Two sub-types:
- Contact healing: Cutting cones cross directly, produce strong lamellar bone
- Gap healing: Small residual gaps are filled with lamellar bone perpendicular to the bone axis, then remodeled longitudinally - this bone is not as strong as contact-healed bone
Primary bone healing does not increase speed of healing - it is actually a much slower process. Early plate removal risks refracture; removal is recommended no sooner than 2 years after surgery.
Natural Bone Healing Cascade
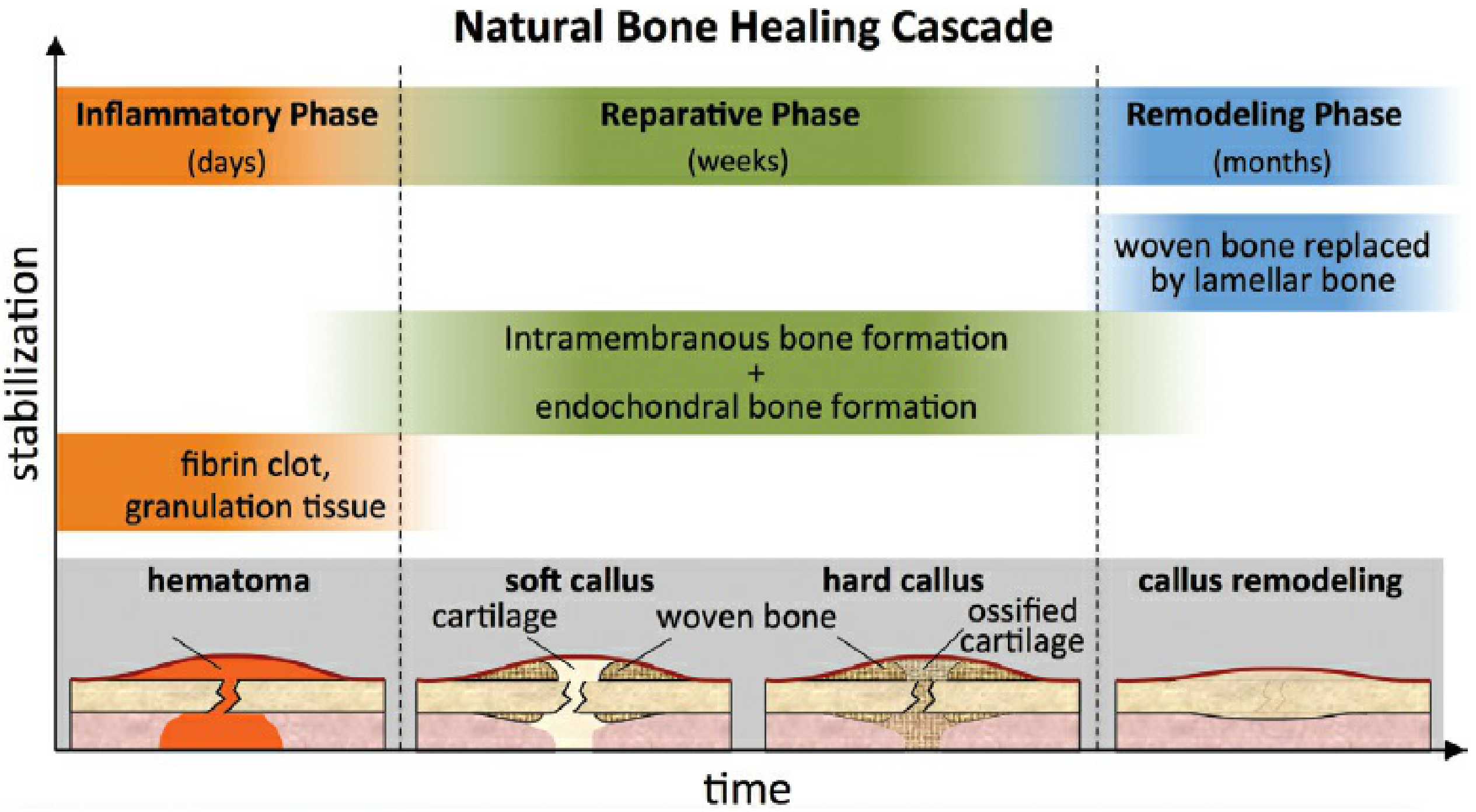
Figure: Qualitative temporal representation of tissue deposited during natural bone healing. As more mature tissue forms, resistance to refracture increases. (Rockwood & Green's, 10th ed)
Phase 1: Inflammatory Phase (Days 0-5)
Stage 1 - Hematoma Formation (Days 0-3)
- Rupture of blood vessels at the fracture site fills the gap with a hematoma
- The clot forms a fibrin scaffold with hematopoietic cells - provides the initial framework
- This tissue has the lowest mechanical stability but can tolerate up to 100% fracture strain
- Most early stability comes from surrounding soft tissues
- Cells present: Monocytes, PMNs (polymorphonuclear cells), T cells, B cells, macrophages
Stage 2 - Granulation Tissue (Days 3-5)
- Inflammatory cells invade the hematoma, initiating lysosomal degradation of necrotic tissue
- Mesenchymal stem cells are recruited from periosteum, endosteum, and bone marrow
- Angiogenesis begins within periosteal tissues and marrow space, routing appropriate cells to the fracture site
- Beginning of the anabolic phase
Phase 2: Reparative Phase (Days 5 - Weeks)
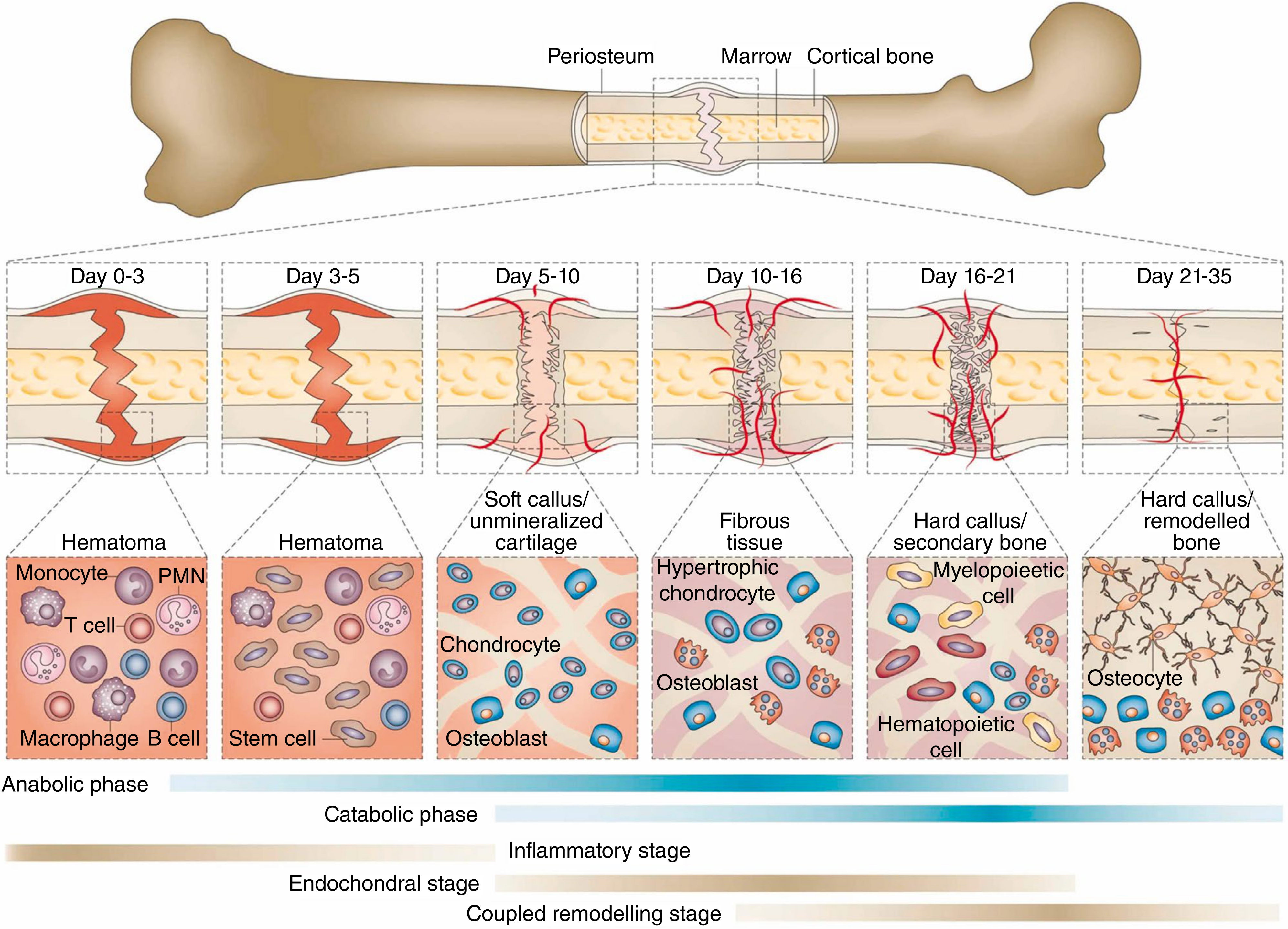
Figure: Fracture healing process showing cell types at each stage from Day 0 to Day 35, with metabolic phases (anabolic/catabolic) and biological stages (inflammatory, endochondral, coupled remodeling). (Campbell's Operative Orthopaedics, 15th ed, 2026 - Adapted from Einhorn & Gerstenfeld, Nat Rev Rheumatol 2015)
Soft Callus (Days 5-16)
- Pluripotential mesenchymal stem cells differentiate into:
- Fibroblasts
- Chondroblasts
- Osteoblasts
- Tissue strain is initially too high close to the fracture for cartilage or bone formation, so granulation tissue (highest allowable strain) forms near the fracture site first
- Intramembranous bone formation begins circumferentially around the periosteal and endosteal surfaces, proximal and distal to the fracture (away from the fracture, where strain is lower)
- Endochondral ossification begins as granulation tissue improves stability: cartilage is deposited along intra- and extramedullary cortex near the fracture
- Soft callus is flexible, cartilaginous, and allows large deformation before failure
- Cells present: Chondrocytes, osteoblasts
Hard Callus (Days 16-21)
- Endochondral ossification continues: the cartilaginous callus undergoes calcification (ossification)
- Progressive mineralization increases stiffness and stability at the fracture site
- The structural moment of inertia increases as callus is deposited away from the neutral axis (extramedullary callus contributes far more to repair strength than intramedullary callus)
- Cells present: Hypertrophic chondrocytes, osteoblasts, hematopoietic cells, myelopoietic cells
- Hard callus marks the end of the reparative phase and the beginning of remodeling
Phase 3: Remodeling Phase (Days 21-35 → Months to Years)
- Woven (immature) bone is replaced by lamellar bone via coupled remodeling
- The medullary canal is restored
- Bone returns to near-normal morphology and mechanical strength
- Cells present: Osteocytes (embedded within remodeled lamellar bone)
- Radioisotope studies have shown increased bone scan activity long after clinical and radiographic union, confirming that remodeling continues for years
Biochemical Steps (Collagen Typing)
The biochemical progression during healing is reflected by the type of collagen present at each stage:
| Step | Collagen Types |
|---|---|
| Mesenchymal | I, II, III, V |
| Chondroid | II, IX |
| Chondroid-osteoid | I, II, X |
| Osteogenic | I |
- Miller's Review of Orthopaedics, 9th ed
Growth Factors in Bone Healing
| Growth Factor | Action | Key Notes |
|---|---|---|
| Bone Morphogenetic Proteins (BMPs) | Osteoinductive; stimulate bone formation | BMPs activate intracellular SMAD signaling molecules to cause osteoblastic differentiation. BMP-2: acute open tibial fractures. BMP-7: tibial nonunions. BMP-4: mutations linked to fibrodysplasia ossificans progressiva. BMP-3: no osteogenic activity |
| TGF-β (Transforming Growth Factor-beta) | Promotes cell proliferation and matrix production | Explored clinically for long bone healing and OA |
| IGF (Insulin-like Growth Factor) | Stimulates bone growth and repair | Works with TGF-β and BMP |
| PDGF (Platelet-Derived Growth Factor) | Cell proliferation, angiogenesis | Co-delivery with BMP-2 studied for enhanced healing |
| FGF (Fibroblast Growth Factor) | Angiogenesis and cell proliferation | |
| VEGF (Vascular Endothelial Growth Factor) | Angiogenesis | Required for revascularization of fracture site |
Key molecular signaling: COX-2 (cyclooxygenase-2) activity is required for normal endochondral ossification during fracture healing.
- Miller's Review of Orthopaedics, 9th ed; Rockwood & Green's, 10th ed
Perren's Strain Theory
Perren's theory explains tissue differentiation at the fracture site based on the local mechanical strain:
| Strain at Fracture Site | Tissue Formed |
|---|---|
| < 100% | Fibrous tissue forms |
| < 10% | Soft callus (cartilage) forms |
| < 2% | Hard callus forms and progressive mineralization occurs |
| 2-5% failure strain | Bone can form (primary healing threshold) |
Clinical implication: A little movement (relative stability) is beneficial - it drives callus formation. Too much movement prevents mineralization and can result in nonunion. Too little movement (with a gap) prevents cutting cones from crossing and can also delay healing.
- Bailey & Love's Short Practice of Surgery, 28th ed
Type of Healing by Stabilization Method
| Type of Stabilization | Predominant Healing Type |
|---|---|
| Cast (closed treatment) | Periosteal bridging callus + interfragmentary endochondral ossification |
| Compression plate | Primary cortical healing (cutting-cone / Haversian remodeling) |
| Intramedullary nail | Early: periosteal bridging callus, endochondral ossification; Late: medullary callus, intramembranous ossification |
| External fixator (less rigid) | Periosteal bridging callus; endochondral ossification |
| External fixator (more rigid) | Primary cortical healing; intramembranous ossification |
| Inadequate immobilization + adequate blood supply | Hypertrophic nonunion (failed endochondral ossification; type II collagen predominates) |
| Inadequate immobilization + inadequate blood supply | Atrophic nonunion |
| Inadequate reduction with displacement | Oligotrophic nonunion |
- Miller's Review of Orthopaedics, 9th ed
Clinical and Radiographic Terminology
| Term | Definition |
|---|---|
| Clinical union | Fracture site is stable and pain-free; sufficient stiffness and strength from mineralization |
| Radiographic union | Bone trabeculae or cortical bone seen crossing the fracture site on plain X-ray |
| Malunion | Fracture heals with residual deformity |
| Delayed union | Healing takes longer than expected for that fracture location (usually > 6 months) |
| Nonunion | Complete failure of the fracture to unite |
Radiological timeline of healing features:
-
Periosteal reaction: seen as early as 4 days, present in ≥50% of cases by 2 weeks
-
Soft callus: visible on radiograph within 2-3 weeks
-
Hard callus: 3-6 weeks
-
Remodeling: peaks around 8 weeks; bone scintigraphy shows increased uptake for up to 1 year
-
Grainger & Allison's Diagnostic Radiology; Bailey & Love's, 28th ed
Factors Affecting Bone Healing
Systemic Factors
| Factor | Effect |
|---|---|
| Tobacco / Nicotine smoking | Single most notable inhibitor. Delays healing, decreases callus strength, increases nonunion risk (especially tibia), increases pseudarthrosis risk after spinal fusion by up to 500% |
| Age | Older patients have slower healing |
| Nutritional status | Protein malnutrition reduces periosteal callus, decreases callus strength, increases fibrous tissue within callus |
| Diabetes | Microvascular disease, reduced immunocompetence, and neuropathy alter bone metabolism → delayed healing |
| Corticosteroids | Decrease callus proliferation |
| NSAIDs | Inhibit COX-2, impairing endochondral ossification; adverse effects on fracture healing |
| Fluoroquinolone antibiotics | Toxic to chondrocytes; slow bone healing |
| Head injury | Can paradoxically increase osteogenic response |
| Growth hormone | Positive - increases callus volume |
| PTH / Thyroid hormone | Positive - promote bone remodeling |
Local Factors
- Vascular disruption or poor perfusion (peripheral vascular disease, soft-tissue injury)
- Severity and energy of injury
- Presence of infection (open fractures)
- Loss of bone / soft-tissue interposition
- Fracture geometry and type
Treatment Factors
- Extent of surgical trauma
- Type of fixation (rigid vs. flexible)
- Fracture displacement, overdistraction
- Load-induced bone and soft-tissue deformation
Stimulation of Fracture Healing
| Method | Mechanism |
|---|---|
| Low-intensity pulsed ultrasound (LIPUS) (30 mW/cm²) | Accelerates healing and increases mechanical strength of callus through cellular response to mechanical energy |
| Direct current electrical stimulation | Stimulates an inflammatory-like response, decreases oxygen, increases tissue pH |
| Alternating current (capacitive coupling) | Affects cAMP and collagen synthesis in the repair stage |
| Pulsed electromagnetic fields (PEMF) | Initiates calcification of fibrocartilage (but not fibrous tissue) |
| Bone grafting | Provides osteoconductivity (scaffold), osteoinductivity (BMP), and osteogenesis (living cells) |
Key Summary
- Natural bone healing progresses through Inflammatory → Reparative (soft callus → hard callus) → Remodeling phases, driven by relative stability
- Primary bone healing requires absolute stability with direct cortical contact; it is slower, not faster
- Perren's strain theory governs tissue differentiation: less strain = more organized tissue
- BMPs (especially BMP-2 and BMP-7) are the most important osteoinductive growth factors, signaling through SMAD pathways
- COX-2 is an essential enzyme for endochondral ossification; NSAIDs and quinolones inhibit it
- Smoking is the single most modifiable systemic inhibitor of bone healing
- Remodeling continues for years even after clinical and radiographic union
This is a shared conversation. Sign in to Orris to start your own chat.