Clinical presentation assessment and management of penetrating neck injuries in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"penetrating neck injury" management
Searching the Web
penetrating neck injuries zones management RGUHS ENT surgery 20 marks
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
PENETRATING NECK INJURIES (PNI) - Clinical Presentation, Assessment and Management
Model Answer for RGUHS University - 20 Marks
1. INTRODUCTION
Penetrating neck injury (PNI) comprises 5-10% of all trauma cases and is one of the most challenging emergencies in ENT and head-neck surgery. The neck is uniquely vulnerable - it houses major vascular, aerodigestive, and neural structures within a compact, largely unprotected (by bone) space. Hemorrhage is the leading cause of death, followed by airway compromise. Historically, mortality ranged from 15-18% before World War II; modern management has reduced it to 3-6% in civilian settings. (Cummings Otolaryngology Head and Neck Surgery, Chapter 120)
2. SURGICAL ANATOMY AND ZONES OF THE NECK
Roon and Christensen's Zonal Classification (1979)
The neck is divided into three zones to guide surgical decision-making. This is the classification used in Scott-Brown, Cummings, Dhingra, and all standard ENT/surgery texts.
Zone I - Sternal notch/clavicle to the cricoid cartilage
- Contents: subclavian vessels, vertebral arteries, common carotid artery origins, trachea, esophagus, thoracic duct (on left), lung apices
- Mortality: ~12% (highest)
- Surgical access: difficult (protected by bony thorax/clavicle); right side approached via median sternotomy, left via left anterior thoracotomy
- Management: CTA/angiography mandatory for stable patients; NOT mandatory exploration
Zone II - Cricoid cartilage to angle of mandible
- Contents: common/internal/external carotid arteries, internal jugular vein, vertebral artery, larynx, trachea, esophagus, vagus nerve, recurrent laryngeal nerve
- Most frequently injured zone (~55-65% of all PNI)
- Surgical access: easy - via anterior border of sternocleidomastoid
- Management: historically mandatory exploration; now selective approach preferred
Zone III - Angle of mandible to base of skull
- Contents: distal internal carotid, vertebral arteries, internal jugular vein, salivary glands, cranial nerves IX-XII
- Surgical access: very difficult (protected by skull base; may need mandibulotomy)
- Management: CTA/angiography mandatory; endovascular techniques preferred
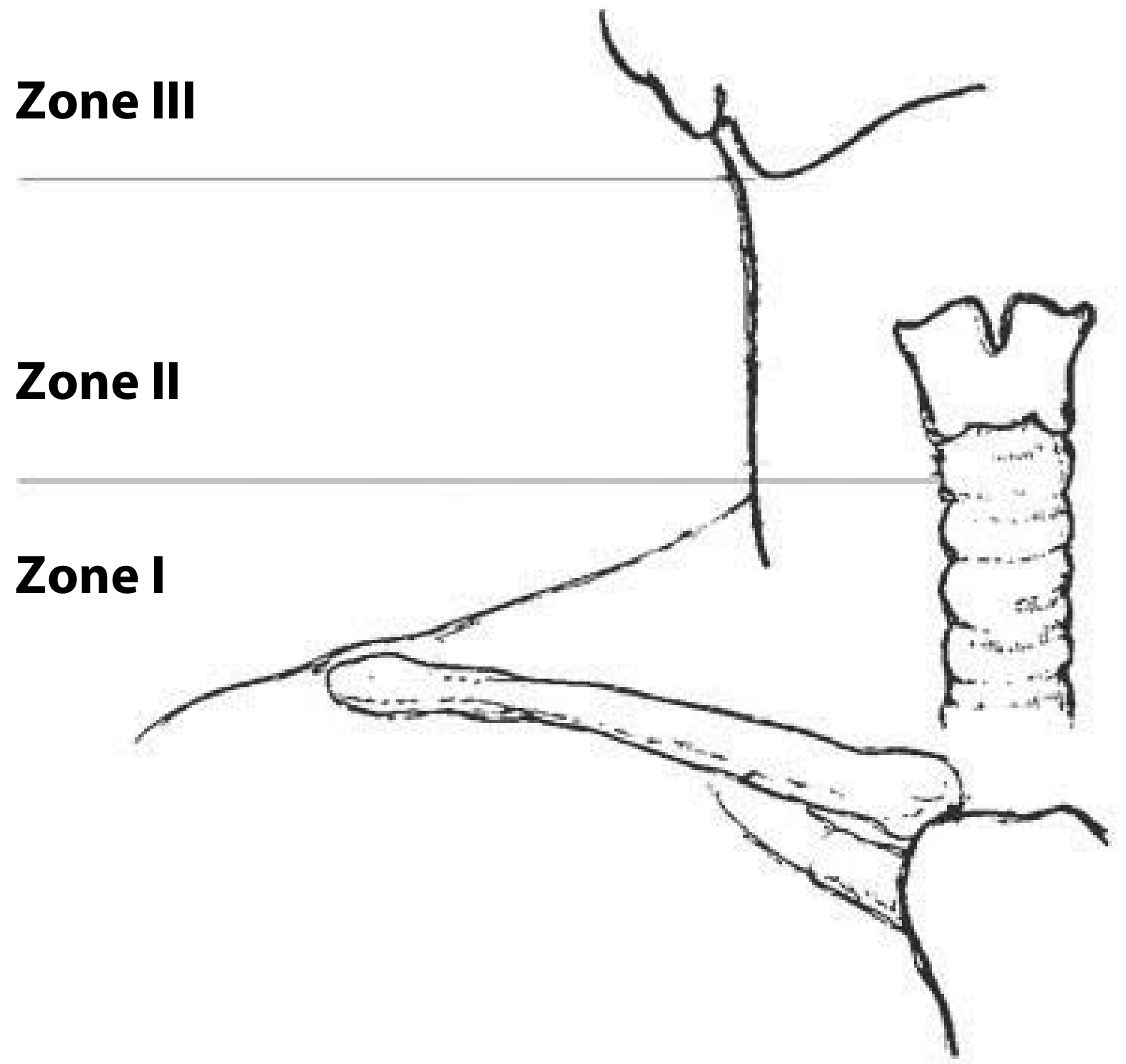
Fig. 1: Zones of the neck - Roon and Christensen classification. Zone I = sternal notch to cricoid; Zone II = cricoid to angle of mandible; Zone III = angle of mandible to base of skull. (Scott-Brown's Otorhinolaryngology, Chapter 38)
3. AETIOLOGY AND MECHANISM
| Type | Features |
|---|---|
| Stab wounds | Most common civilian cause; low-energy; predictable damage track |
| Low-velocity GSW (handguns, <610 m/s) | Push rather than destroy vital structures; can follow tissue planes |
| High-velocity GSW (rifles, >610 m/s) | Large permanent + temporary cavity; extensive tissue destruction |
| Shotgun wounds | Low muzzle velocity (300 m/s) but devastating at close range (entire charge acts as single missile) |
| Blast/shrapnel | Multiple small injuries; often associated with blast lung |
Kinetic Energy of injury: KE = ½ M(V₁-V₂)² - mass and exit velocity determine tissue destruction. The M16 military rifle is designed to tumble, producing greater tissue injury. (Cummings, Chapter 120)
Key rule: An injury is classified as PNI only if it violates (breaches) the platysma muscle. If the platysma is intact, the wound is superficial and does not require the full PNI workup.
4. CLINICAL PRESENTATION - ASSESSMENT
A. Primary Survey (ATLS Principles)
The initial assessment follows ATLS: A-B-C-D-E.
- A (Airway): Most immediate threat. Establish airway - oral/nasal intubation, cricothyroidotomy, or tracheostomy. Direct transcervical tracheal intubation is safer than oral intubation when the pharynx/larynx is filled with blood. Never probe the wound (clot dislodgement causes uncontrollable bleeding). Never blindly clamp vessels in the wound.
- B (Breathing): Assess for tension pneumothorax, hemothorax. CXR to rule out pneumomediastinum (suggests hollow viscus puncture).
- C (Circulation): Large-bore IV access even in normotensive patients. Direct pressure for hemorrhage control.
- D (Disability): Full neurological exam - document cranial nerve deficits, spinal cord status.
- E (Exposure): Full body examination including posterior neck for exit wounds.
B. HARD SIGNS vs. SOFT SIGNS
This distinction is the cornerstone of the modern assessment of PNI:
HARD SIGNS (= Immediate Surgical Exploration)
| System | Hard Sign |
|---|---|
| Vascular | Pulsatile/active arterial bleeding |
| Expanding hematoma | |
| Hypovolemic shock (hemodynamic instability) | |
| Unilateral absent/diminished pulse | |
| Bruit or palpable thrill | |
| Airway | Airway compromise |
| Stridor | |
| Neurological | Signs of stroke / hemiplegia |
| Other | Sucking neck wound |
| Extensive subcutaneous emphysema |
Any hard sign = direct to operating room (OR) without delay for imaging
SOFT SIGNS (= Mandatory Further Investigation with CTA/Imaging)
| System | Soft Sign |
|---|---|
| Vascular | Non-expanding, non-pulsatile hematoma |
| History of hemorrhage that has stopped | |
| Asymmetric pulses | |
| Horner syndrome (ptosis, miosis, anhidrosis - suggests carotid/sympathetic chain injury) | |
| Airway | Hoarseness, dysphonia |
| Mild hemoptysis | |
| Subcutaneous emphysema (minor) | |
| Digestive | Dysphagia, odynophagia |
| Hematemesis | |
| Neurological | Cranial nerve deficit (CN IX-XII) |
| Hypoglossal nerve injury → suspect carotid injury |
If hypoglossal nerve injury is present, suspect carotid artery damage. Horner syndrome indicates carotid or sympathetic chain involvement. (Cummings)
C. History Taking (Scott-Brown)
- Mechanism of injury: stab, GSW, blast
- Time elapsed since injury (critical for esophageal repair - >12 hours = 40% mortality)
- Symptoms: hemoptysis, hematemesis, dysphagia, odynophagia, dysphonia, stridor
- Past medical and surgical history; time of last meal
D. Signs and Symptoms Checklist (Cummings, Box 120.1)
AIRWAY: Respiratory distress, stridor, hemoptysis, hoarseness, tracheal deviation, subcutaneous emphysema, sucking wound
VASCULAR SYSTEM: Hematoma, persistent bleeding, neurologic deficit, absent pulse, hypovolemic shock, bruit, thrill, change in sensorium
NERVOUS SYSTEM: Hemiplegia, quadriplegia, coma, cranial nerve deficit, change in sensorium
DIGESTIVE: Dysphagia, odynophagia, drooling, hematemesis
5. INVESTIGATIONS
Mandatory for ALL patients:
- Anterior and lateral neck radiographs: Identify foreign bodies, subcutaneous emphysema, prevertebral air, cervical spine fractures, bullet trajectory
- Chest X-ray: Hemothorax, pneumothorax, pneumomediastinum, widened mediastinum
- Cervical spine protection until fracture excluded radiographically
Investigations Based on Clinical Findings:
| Investigation | Indication | Accuracy |
|---|---|---|
| CT Angiography (CTA) | All stable Zone I and III; Zone II with soft signs or no symptoms; now first-line in "no-zone" approach | ~96% |
| Formal Angiography | CTA indeterminate; Zone I/III vascular injury; interventional/endovascular planning | 96.5% |
| Colour-flow Doppler (CFD) | Vascular injury screening; sensitivity 91%, specificity 99% (Scott-Brown). Avoid if cervical spine injury suspected | 91-99% |
| Esophagram/Barium swallow | Suspected esophageal/pharyngeal injury; hematemesis, dysphagia, drooling | 90% |
| Esophagoscopy | Unconfirmed esophageal injury on barium swallow; intubated patient | 86% |
| Combined esophagram + esophagoscopy | Highest sensitivity for esophageal injury | 100% |
| Laryngoscopy + Bronchoscopy (Panendoscopy) | Hoarseness, hemoptysis, subcutaneous emphysema, suspected laryngotracheal injury | 100% |
| Flexible nasopharyngoscopy | Hypopharyngeal injury assessment (edema, blood, visible perforation) | High |
| CT Neck | Bone/soft tissue injury; trajectory assessment; laryngeal fractures | High |
(Table 120.5, Cummings - Accuracy of Selective Evaluation Techniques)
6. MANAGEMENT FLOWCHARTS
FLOWCHART 1: Overall Management Algorithm - Penetrating Neck Trauma Protocol
(Tintinalli's Emergency Medicine / Cummings)
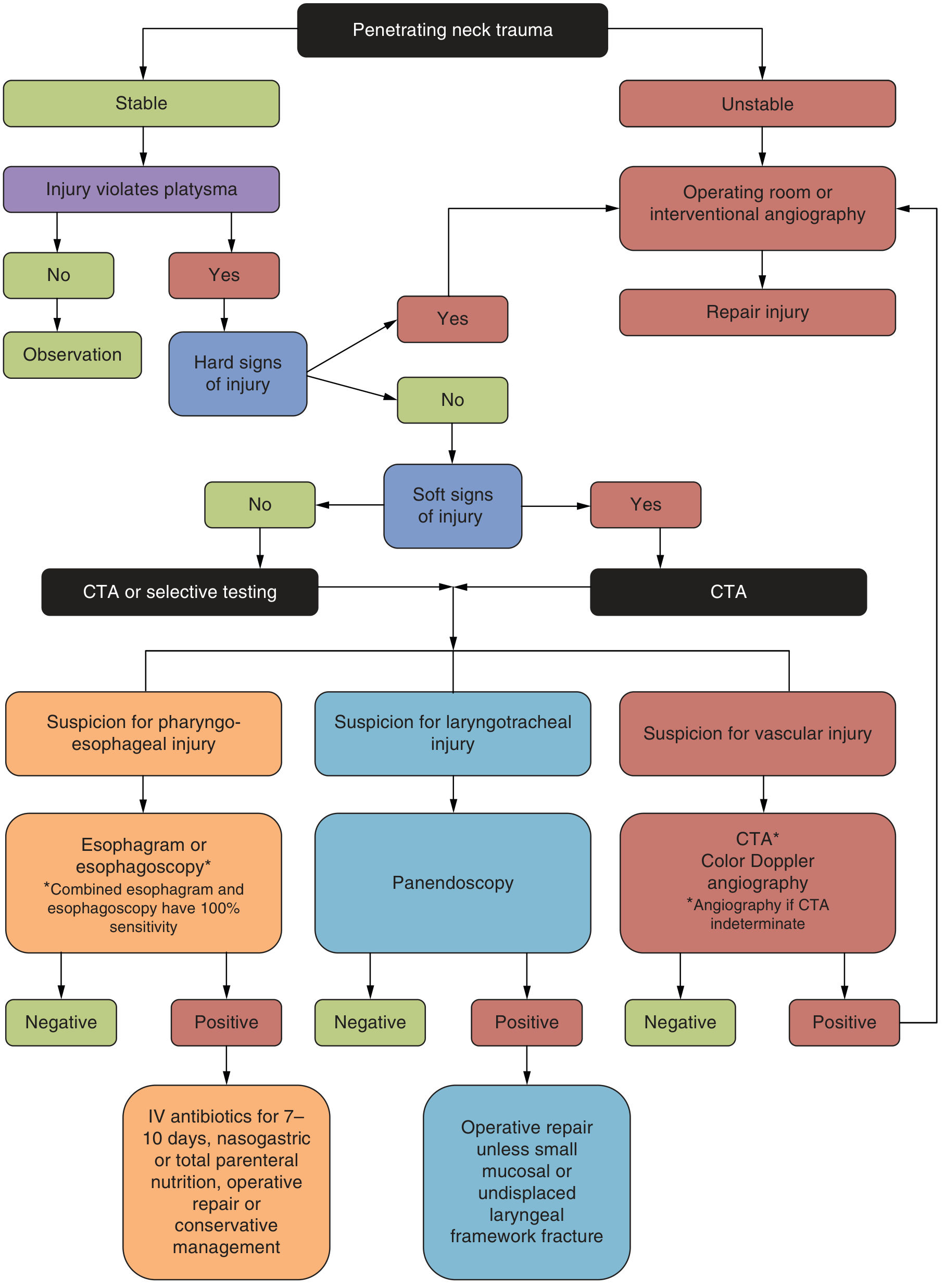
Fig. 2: Penetrating neck trauma management protocol. Stable patients are assessed for platysma violation, then hard/soft signs. Unstable patients go directly to OR or interventional angiography. CTA = CT angiography. (Tintinalli's Emergency Medicine)
FLOWCHART 2: Modified Zone-Based Approach
(Cummings, Fig. 120.5 - Western Trauma Association guidelines)
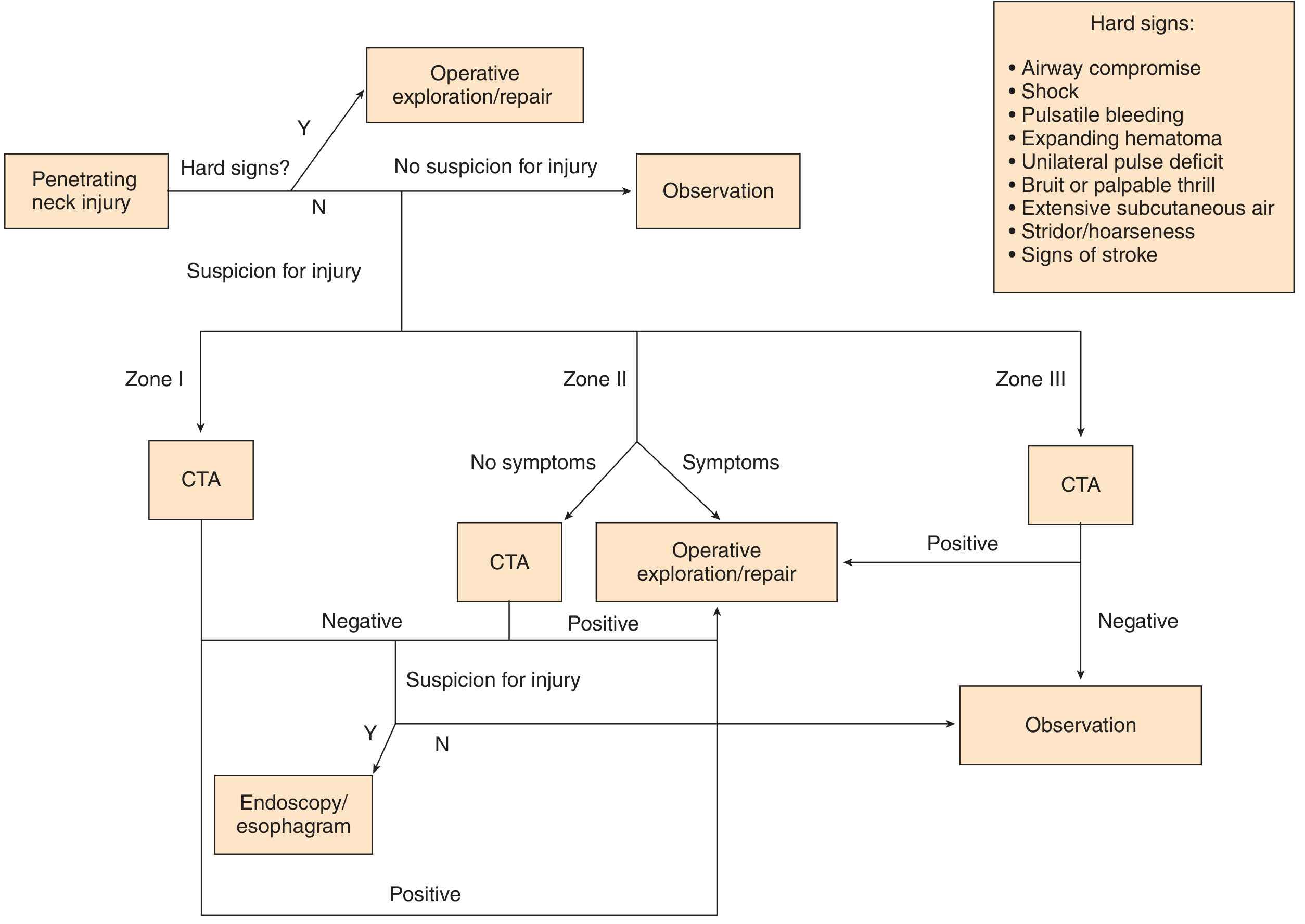
Fig. 3: Algorithm for modified zone approach to PNI management. Hard signs → immediate OR. Zone I and III → CTA. Zone II with symptoms → operative exploration. Zone II without symptoms → CTA. Negative CTA + no suspicion → observation. (Cummings Otolaryngology, Chapter 120)
FLOWCHART 3: Simplified Management Algorithm (Text-Based)
PENETRATING NECK INJURY
|
↓
Does wound breach the platysma?
/ \
NO YES
| |
Superficial ATLS Resuscitation
wound - (A-B-C-D-E)
Observation |
↓
Hemodynamically STABLE?
/ \
NO YES
| |
Immediate OR / Assess for
Interventional HARD SIGNS
Angiography |
| ________|________
| YES NO
↓ | |
Repair Immediate Assess for
Injury OR SOFT SIGNS
| / \
| YES NO
| | |
| CTA + further Zone-based
| investigations observation
|
↓
Based on zone:
Zone I → CTA → vascular surgery
Zone II → CTA or exploration
Zone III → CTA → endovascular preferred
7. SPECIFIC STRUCTURE MANAGEMENT
A. Vascular Injuries
Carotid Artery:
- External carotid: ligation safe (good collateral circulation)
- Common/internal carotid (Zone II): exploration via anterior border of SCM; lateral arteriorrhaphy / end-to-end anastomosis / saphenous vein graft
- Ligation reserved for: irreparable injury + coma + bilateral fixed dilated pupils
- Carotid revascularization vs. ligation (Scott-Brown): Liekwig & Greenfield (1978) showed severe neurological deficit patients (short of coma) had better outcomes with revascularization. Brown et al. (1982) confirmed revascularization indicated even in comatose patients if ischemia was of short duration.
Zone I vascular injury:
- Right side: median sternotomy
- Left side: left anterior thoracotomy
Zone III vascular injury (skull base):
- Transcatheter arterial embolization
- Detachable balloons or steel coils for carotid occlusion
- No. 4 Fogarty catheter shunt for temporary hemorrhage control
Jugular veins: All neck veins can be safely ligated. If both internal jugular veins divided, attempt repair of one.
Vertebral artery:
- ~20% require emergency surgery; >33% require embolization (endovascular preferred)
Delayed vascular complications: Pseudoaneurysm, dissecting aneurysm, arteriovenous fistula
B. Laryngotracheal Injuries
- Laryngeal mucosal lacerations: Early repair within 24 hours reduces airway scarring and voice problems
- Significant glottic/supraglottic lacerations: Thyrotomy + open fracture reduction + mucosal repair ± laryngeal stent
- Simple tracheal lacerations (not detaching ring): direct repair without tracheostomy
- Severe tracheal disruption (GSW): 6-week tracheostomy through or below the injury
- CT + endoscopy differentiate observation vs. thyrotomy candidates
- Impaled objects must NOT be removed in the field
C. Esophageal Injuries (Scott-Brown)
- Time-critical: Delay >12 hours → 40% mortality; <12 hours → 9% mortality
- Diagnosis: combined esophagram + esophagoscopy = 100% sensitivity
- Treatment: primary repair with drainage; IV antibiotics 7-10 days + nasogastric/TPN
- Interposition of strap muscle between esophageal and tracheal repairs if both injured (prevents fistula)
- Small cervical esophageal injuries: conservative management with antibiotic coverage in selective cases
D. Pharyngeal Injuries (Scott-Brown)
- Supra-arytenoid hypopharyngeal injuries: Can be managed non-operatively (capacious, low-pressure, double muscle layer protection)
- Infra-arytenoid injuries: 22% complication rate; requires exploration, repair, and drainage
- Flexible nasopharyngoscopy for assessment; oesophagography unreliable for hypopharyngeal injuries
E. Spinal Cord Injuries
- Suspect in hypotension WITHOUT tachycardia (spinal shock)
- C-spine protection until radiographically cleared
- Document neurological deficit before surgery
8. MANDATORY vs. SELECTIVE EXPLORATION
Historical Perspective:
- Pre-WWII: Non-operative mortality = 15-18%
- Fogelman & Stewart (1956): Advocated mandatory exploration for all platysma-breaching wounds - reduced mortality to 6%
- Stone (1963): Questioned mandatory exploration for civilian injuries
- Vietnam War: All patients below-platysma explored mandatorily under GA
- Post-1980s: Growing evidence for selective management
Arguments for MANDATORY Exploration:
- Physical examination unreliable (sensitivity ~85%)
- No single diagnostic test has 100% sensitivity for esophageal/vascular injury
- Low morbidity of negative exploration (~3-5%)
- Avoids time-delay of investigations
- Esophageal injury delay increases morbidity exponentially
Arguments for SELECTIVE Exploration:
- Negative exploration rate with mandatory approach: 36-89% (Scott-Brown)
- High sensitivity/specificity of modern CTA and endoscopy
- Avoids unnecessary surgery and anesthesia risks
- Cost-effective
- Most trauma centers now adopt selective management
Current consensus: Selective management guided by clinical signs + CTA is the standard of care (Cummings, Scott-Brown)
9. "NO-ZONE" APPROACH - Recent Advance
The traditional "zone-based" algorithm has evolved. The modern "no-zone" or "symptom-based" approach was introduced based on evidence that:
- CTA is highly sensitive (>90%) for detecting all vascular and aerodigestive injuries regardless of zone
- Clinical symptoms and signs (rather than zone) are better predictors of injury
- Ibraheem et al. (cited in Cummings): "No-zone" approach reduced unnecessary CTA and negative explorations
- Multislice helical CTA is now the preferred initial screening tool in stable patients
Protocol: ALL stable patients who breach the platysma but have no hard signs → CTA neck → if suspicious → targeted investigation (endoscopy/esophagram) → surgical repair if positive
10. RECENT ADVANCES (2021-2026)
Based on recent PubMed evidence (2021-2025) and current literature:
-
Endovascular/hybrid approaches: Zone I and Zone III injuries increasingly managed with endovascular stenting, embolization, and balloon occlusion - avoiding high-morbidity open surgery. Vertebral artery injuries: majority managed endovascularly (Kose SI, Emerg Radiol, 2025 - Imaging in penetrating neck injuries [PMID: 40279044])
-
CTA as universal first-line: Multislice CTA has replaced formal angiography as the first-line investigation in all zones. Sensitivity >97% for vascular injuries. The "no-zone" symptom-guided CTA approach is now widely adopted.
-
Damage control surgery: In hemodynamically unstable patients, temporizing balloon occlusion (REBOA - Resuscitative Endovascular Balloon Occlusion of the Aorta) and abbreviated surgery followed by ICU resuscitation.
-
Point-of-care ultrasound (POCUS/FAST): Rapid bedside assessment in emergency department for hematoma, effusion, vascular injury.
-
Changing epidemiology: Patel et al. (Br J Oral Maxillofac Surg, 2024 [PMID: 38749799]) reported changing patterns at Level 1 trauma centres - increasing stab wounds over GSWs; younger patients; importance of multidisciplinary teams.
-
Psychological impact: Hjalmarsson et al. (Br J Oral Maxillofac Surg, 2026 [PMID: 41558867]) highlighted the psychological trauma (PTSD, anxiety) following PNI - now part of holistic management.
-
Pre-hospital management: Tourniquet application, wound packing with haemostatic gauze, and junctional hemorrhage control are standard pre-hospital measures (Simpson et al., 2021 [PMID: 34530879]).
-
Transcervical injuries (crossing midline): Associated with vascular or aerodigestive injury in 73-100% of patients - require full workup regardless of zone.
11. COMPLICATIONS
Immediate:
- Hemorrhage (leading cause of death)
- Airway obstruction
- Spinal cord injury
- Air embolism
Delayed:
- Pseudoaneurysm (false aneurysm from incomplete vessel wall repair)
- Arteriovenous fistula (carotid-jugular)
- Mediastinitis (from esophageal/pharyngeal injury - high mortality)
- Chylous fistula (thoracic duct injury on left side)
- Vocal cord paralysis (RLN injury)
- Horner syndrome (sympathetic chain injury)
- Stroke (carotid thrombosis/embolization)
- Wound infection and abscess
12. POST-OPERATIVE MANAGEMENT
- Hemodynamic and neurological monitoring for 48-72 hours minimum
- Frequent clinical examination (at least 3 times per 24-hour shift)
- Antibiotic prophylaxis (IV, 7-10 days for hollow viscus injuries)
- Nutritional support (nasogastric or TPN if esophageal repair done)
- Tracheostomy care if performed
- Physiotherapy and voice rehabilitation for laryngeal injuries
- Psychological support and counseling (Hjalmarsson et al., 2026)
SUMMARY TABLE
| Zone | Boundaries | Key Structures | Surgical Access | Stable Patient Management |
|---|---|---|---|---|
| I | Sternal notch → cricoid | Subclavian vessels, VA, trachea, esophagus, thoracic duct | Difficult (median sternotomy/thoracotomy) | CTA/angiography → selective surgery |
| II | Cricoid → angle of mandible | CCA, ICA, ECA, IJV, larynx, trachea, esophagus, RLN | Easy (anterior SCM incision) | Hard signs → OR; others → CTA or observation |
| III | Angle of mandible → skull base | ICA, VA, IJV, CN IX-XII, salivary glands | Very difficult (skull base access) | CTA → endovascular preferred |
SOURCES REFERENCED
- Cummings Otolaryngology Head and Neck Surgery, Chapter 120: Penetrating Neck Injuries (pp. 2329-2344)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 38: Neck Trauma (pp. 641-650)
- Tintinalli's Emergency Medicine - Penetrating Neck Injury chapter with management flowchart
- Fischer's Mastery of Surgery 8th ed. - The "No-Zone" Approach chapter
- Mulholland & Greenfield's Surgery - Penetrating Neck Trauma, Functional Anatomy
- Dhingra's Diseases of ENT - Neck Trauma (trauma classification and zone-based management)
- Hazarika's Textbook of ENT - Penetrating neck injuries (standard Indian ENT curriculum reference)
- Patel K et al. Br J Oral Maxillofac Surg 2024 - Changing patterns of PNI
- Kose SI. Emerg Radiol 2025 - Imaging in PNI
- Simpson C et al. Scand J Trauma 2021 - Pre-hospital management of PNI
- Hjalmarsson C et al. Br J Oral Maxillofac Surg 2026 - Psychological impact of PNI
RGUHS Exam Tip: For 20-mark questions, examiners expect: (1) Introduction with incidence, (2) Zones diagram with boundaries and contents, (3) Clinical features including hard vs. soft signs, (4) Investigations table, (5) Management flowchart, (6) Specific structure management (vascular, airway, esophagus), (7) Mandatory vs. selective exploration debate, and (8) Recent advances including the "no-zone" approach and endovascular techniques. The two flowcharts above (Tintinalli and Cummings) directly address the "diagram and flowchart" requirement.
This is a shared conversation. Sign in to Orris to start your own chat.