Tell me obs and gynac history taking and examination in detail with proper understanding with images
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
obstetric gynecology history taking examination GTPAL Leopold maneuvers detailed
Reading Web Page
Leopold maneuvers obstetric history GTPAL examination
Searching the Web
Leopold maneuvers diagram image obstetric abdominal examination fetal presentation
Loading Image
Searching the Web
gynecological pelvic examination diagram speculum bimanual uterus diagram
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
Leopold maneuvers four steps diagram infographic obstetric
Loading Image
I now have comprehensive material from Berek & Novak's Gynecology, Schwartz's Surgery, Williams Obstetrics (via web), and visual images. Let me compose the full, detailed answer.
Obstetrics & Gynaecology: History Taking and Examination
Sources: Berek & Novak's Gynecology (16th Ed.), Schwartz's Principles of Surgery (11th Ed.), Williams Obstetrics (24th Ed.), StatPearls
PART 1 - THE APPROACH TO THE PATIENT
Before taking any history, establish rapport. The intimate and highly personal nature of gynaecological conditions demands particular sensitivity to evoke an honest response. Key principles:
- Empathy and attentive listening - the patient must feel her concerns are heard
- Confidentiality - privileged information belongs to the patient
- Non-judgmental attitude - especially regarding sexual practices, gender identity, and reproductive choices
- Whole-patient view - medical, psychological, social, cultural, and family dimensions all matter
A complete gynaecological assessment covers chief complaint, history of present illness, menstrual history, obstetric history, sexual history, contraceptive history, past medical and surgical history, family history, and social history.
PART 2 - HISTORY TAKING
2.1 Chief Complaint and History of Present Illness
Use the SOCRATES framework to characterize any symptom:
| Component | What to ask |
|---|---|
| Site | Where exactly is the problem? |
| Onset | When did it start? Sudden or gradual? |
| Character | Nature of pain/discharge/bleeding |
| Radiation | Does it spread anywhere? |
| Associated symptoms | Nausea, fever, dysuria, back pain? |
| Timing | Constant, intermittent, cyclical? |
| Exacerbating/relieving factors | What makes it worse or better? |
| Severity | On a scale of 1-10 |
The table below from Schwartz's Principles of Surgery summarizes the key elements systematically:
| Issue | Elements to Explore | Significance |
|---|---|---|
| Menstrual history | Age at menarche, cycle pattern, LMP, PMB, intermenstrual spotting, medication use | Identifies endocrine, structural, infectious, oncologic causes |
| Obstetrical history | Number of pregnancies, dates, type of deliveries, losses, complications | Predisposing factors for GTD, surgical complications |
| Sexual history | Partners, practices, protection, pregnancy intention | Risk assessment, STI testing sites, anatomical collection |
| Infectious diseases | STDs, treatment, HIV status | Also assess GI diseases mimicking STDs |
| Contraceptive history | Current and prior methods, duration | Concurrent pregnancy risk, contraceptive complications |
| Cytologic screening | Frequency, prior abnormal Pap, prior surgery | Cervical cancer screening adequacy |
(Schwartz's Principles of Surgery, 11th Ed.)
2.2 Menstrual History (PALM-COEIN Framework)
Ask about:
- Age at menarche (normal: 10-16 years)
- Cycle regularity - is it regular (every 21-35 days)?
- Duration of bleeding - normally 2-7 days
- Amount of flow - number of pads/tampons per day, clots, flooding
- Dysmenorrhoea - primary (no cause) or secondary (endometriosis, fibroids)
- Intermenstrual bleeding (IMB) - bleeding between periods
- Post-coital bleeding (PCB) - suggests cervical pathology
- Post-menopausal bleeding (PMB) - always requires investigation (endometrial cancer until proven otherwise)
- LMP (Last Menstrual Period) - exact date, character (was it normal?)
- Premenstrual symptoms - breast tenderness, mood changes, bloating
"The menstrual history should include age at menarche, frequency and duration of periods, dysmenorrhoea or associated symptoms, last menstrual period, longest gap between menses, and any birth control." - Swanson's Family Medicine Review
Key terms:
- Amenorrhoea: absence of periods (primary >16 yrs, secondary >3 cycles)
- Oligomenorrhoea: cycles >35 days apart
- Menorrhagia: heavy periods (>80 mL or >7 days)
- Metrorrhagia: irregular, frequent bleeding
- Menometrorrhagia: both heavy and irregular
2.3 Obstetric History - GTPAL System
Every obstetric history must be recorded using GTPAL:
| Letter | Stands for | Definition |
|---|---|---|
| G | Gravida | Total number of times pregnant (including current pregnancy, ectopics, miscarriages, molar pregnancies) |
| T | Term | Number of deliveries at ≥37 weeks gestation |
| P | Preterm | Number of deliveries between 20-36+6 weeks |
| A | Abortus | Number of pregnancies ending before 20 weeks (spontaneous or induced) |
| L | Living | Number of currently living children |
Example: A woman with 3 pregnancies - one full-term delivery, one premature birth, one miscarriage, with 2 living children = G3T1P1A1L2
"Gravidity = number of times the woman has become pregnant (includes preterm births, ectopic pregnancies, molar pregnancies, and abortions). Parity = number of pregnancies reaching viable gestational age (>20 weeks), INCLUDING stillbirths." - Williams Obstetrics, 24th Ed.
For each previous pregnancy, document:
- Year of pregnancy and outcome
- Gestational age at delivery
- Mode of delivery (SVD, instrumental, LSCS - and reason)
- Birth weight of baby
- Any complications (PPH, pre-eclampsia, GDM, prolonged labour)
- Neonatal outcome
2.4 Sexual History (5 P's)
Take sensitively, explain confidentiality first:
- Partners - How many partners in the last 3 months/12 months? Male, female, both?
- Practices - Type of sexual activity (vaginal, oral, anal)?
- Protection - Do you use condoms? Consistently?
- Past STIs - Any previous infections? Treated?
- Pregnancy plans - Are you currently trying to conceive or avoid pregnancy?
2.5 Contraceptive History
- Current contraceptive method and duration of use
- Past methods used and why stopped
- Any complications (e.g., VTE on OCP, PID with IUD)
- Future contraceptive plans
2.6 Smear/Screening History
- Last cervical smear - date and result
- Any previous abnormal smear (CIN grade, treatment - LLETZ, cryotherapy)
- HPV status if known
- Up-to-date with screening program?
2.7 Past Medical and Surgical History
Particularly important in obs & gynae:
- Previous pelvic or abdominal surgery (affects adhesions, future fertility)
- Thyroid disease, diabetes, hypertension, epilepsy (all affect pregnancy)
- Autoimmune conditions (SLE, APS - recurrent miscarriage)
- Bleeding disorders (affects menorrhagia management)
2.8 Drug History and Allergies
- Current medications (including OTC and herbal)
- Folic acid use (pre-conception/first trimester)
- Teratogenic drugs (warfarin, valproate, ACE inhibitors, retinoids)
- Drug allergies with reaction type
2.9 Family History
Important FH in obs & gynae:
- Breast cancer (BRCA1/2 risk)
- Ovarian cancer
- Endometrial cancer
- Cervical cancer
- Pre-eclampsia, gestational diabetes, thrombophilia
- Congenital anomalies
2.10 Social History
- Smoking (pack years - affects fertility, pregnancy, cervical cancer)
- Alcohol use (units per week)
- Recreational drugs
- Occupation
- Relationship status, domestic violence screening ("Do you feel safe at home?")
- Ethnicity (certain conditions more prevalent, e.g., fibroids in Afro-Caribbean women)
PART 3 - PHYSICAL EXAMINATION
3.1 General Examination
Before the pelvic exam, perform a full general examination:
- General appearance: well/unwell, pallor (anaemia from menorrhagia), jaundice
- Vital signs: BP, pulse, temperature, respiratory rate, weight/BMI
- Thyroid: goitre, signs of thyroid dysfunction
- Breasts: detailed examination (see below)
- Cardiovascular and respiratory: baseline assessment
- Lymph nodes: inguinal nodes (vulval malignancy, STIs), supraclavicular nodes (metastatic disease)
- Abdomen: before pelvic exam
3.2 Abdominal Examination
Inspection:
- Distension (ascites, mass, pregnancy)
- Visible scars (previous laparotomy, Pfannenstiel, laparoscopy ports)
- Striae gravidarum (pregnancy history)
- Linea nigra (pregnancy)
- Visible masses
Palpation:
- Start away from the area of tenderness
- Liver, spleen size
- All four quadrants systematically
- Any mass: site, size, shape, surface, consistency, tenderness, mobility, whether you can get below it
- Rebound tenderness (peritonism - PID, ruptured ectopic)
Percussion:
- Shifting dullness and fluid thrill (ascites - ovarian cancer)
- Organomegaly
Auscultation:
- Bowel sounds
- Fetal heart sounds (in pregnancy, from ~12 weeks with Doppler, ~24 weeks with Pinard)
"Evidence of fullness or mass effect should be noted. This is particularly important in evaluating patients who may have a pelvic mass and in determining the extent of omental involvement, for example, with metastatic ovarian cancer." - Berek & Novak's Gynecology
3.3 Obstetric-Specific Abdominal Examination
In pregnant women, the abdominal examination includes:
Fundal Height Measurement:
- Measured in cm from the symphysis pubis to the top of the uterine fundus
- From 20 weeks, fundal height in cm approximates gestational age in weeks
- SFH <10th centile = growth restriction; >90th centile = macrosomia, polyhydramnios, multiple pregnancy
Leopold's Maneuvers - systematic palpation to determine fetal lie, presentation, position, and engagement:

| Maneuver | Also called | Technique | What it determines |
|---|---|---|---|
| 1st | Fundal Grip | Face patient, palpate the fundus with both hands | Which fetal part is in the fundus (head = hard, round, ballottable; breech = soft, irregular, non-ballottable) |
| 2nd | Lateral/Umbilical Grip | Hands on lateral sides of uterus, one side steady while other palpates | Location of fetal back (hard, smooth, resistant) vs. small parts (irregular, nodular) |
| 3rd | Pawlik's Grip | Single hand above symphysis pubis, thumb and fingers grasp presenting part | Nature and engagement of the presenting part; if movable = not engaged |
| 4th | Pelvic Grip | Face patient's feet, fingertips directed toward pelvic inlet, deep pressure bilaterally | Degree of descent/engagement; hands converge = head not engaged; diverge = engaged |
(Williams Obstetrics, 24th Ed.)
Auscultation of Fetal Heart:
- Normal FHR: 110-160 bpm
- Pinard stethoscope (from ~24 weeks) or Doppler (from ~12 weeks)
- Best heard over the fetal back
3.4 Pelvic Examination
Position: Patient lies in the dorsal lithotomy position, bladder emptied, adequately draped and privacy maintained.
A chaperone should always be offered and documented.
The pelvic examination follows a structured sequence (from Berek & Novak's Gynecology, Table 1-6):
A. External Genitalia - Inspection
Inspect systematically:
- Mons pubis - hair distribution (decreased in hypoestrogenism, virilization causes male-pattern)
- Labia majora - skin characteristics, symmetry, swelling, ulcers, warts
- Labia minora - mucosal changes, lesions
- Clitoris - size (clitoromegaly in androgen excess), adhesions
- Urethral orifice - caruncle, prolapse, discharge
- Vaginal introitus - patency, hymenal remnants
- Perineum - old lacerations, episiotomy scars
- Anus - haemorrhoids, skin tags, fissures, warts
Special palpations:
- Bartholin's glands (posterior labia majora): palpate for cyst/abscess - tender, fluctuant swelling at 5 or 7 o'clock position
- Skene's glands (paraurethral): milk the urethra for discharge if urethritis suspected
- Prolapse screen: Ask patient to bear down (Valsalva) - observe for anterior wall bulge (cystocele), posterior wall bulge (rectocele/enterocele), or cervical descent (uterine prolapse)
B. Speculum Examination
The Cusco (bivalve) speculum is most commonly used in the UK/India; Graves speculum for larger vaginas.
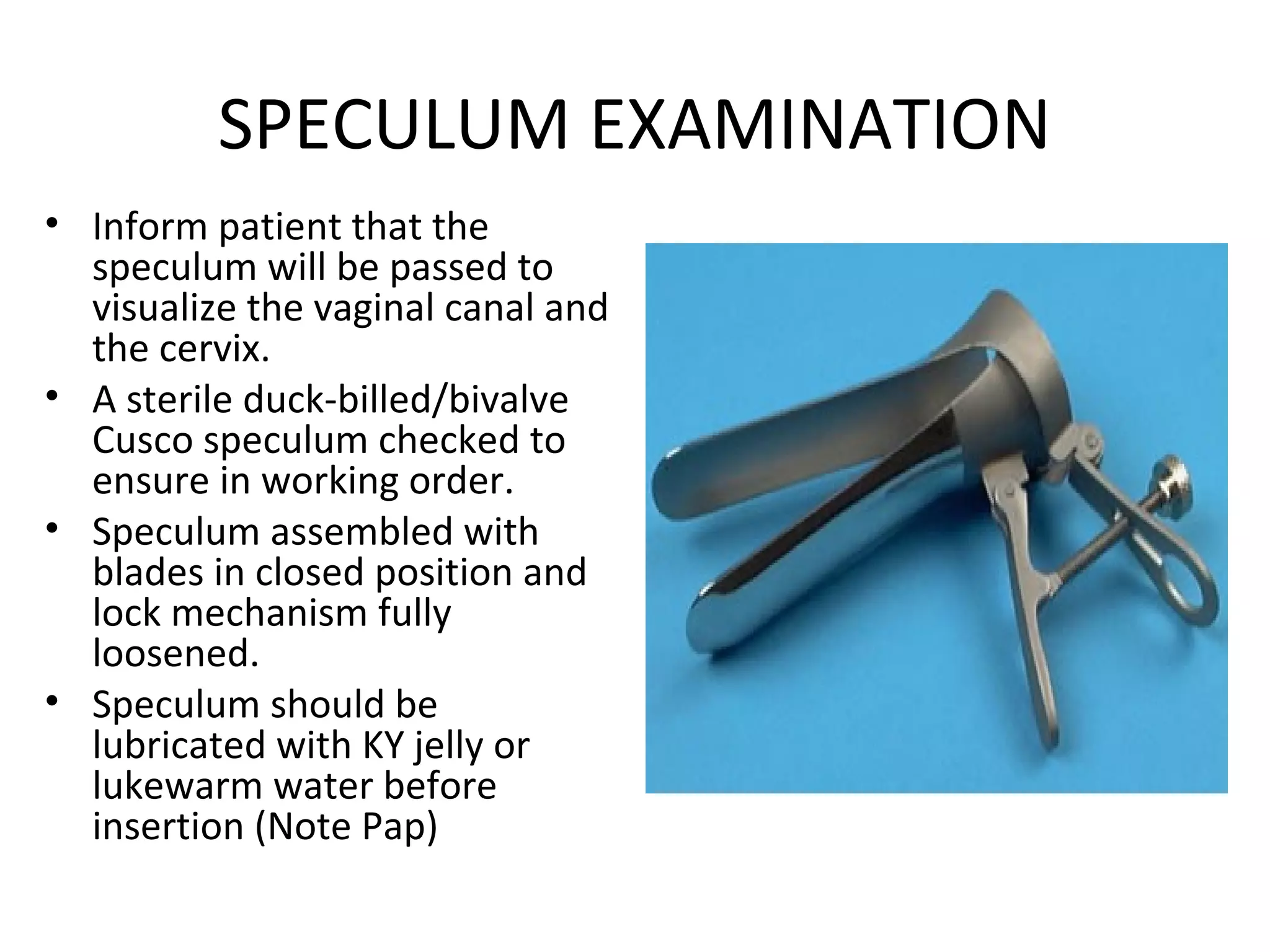
Technique:
- Warm and lubricate the speculum (use warm water if Pap smear planned - lubricant can interfere)
- Separate the labia with the non-dominant hand
- Insert blades obliquely (45°), directed posteriorly along the vaginal axis
- Once fully inserted, rotate to horizontal and open blades to visualize the cervix
- Lock the blades open when the cervix is visualized
What to inspect:
Vaginal walls:
- Colour (bluish = Chadwick's sign of pregnancy)
- Rugae (atrophic if flat and pale = oestrogen deficiency)
- Discharge: colour, consistency, smell (white curdy = candidiasis; grey frothy malodorous = BV; green/yellow frothy = trichomoniasis; mucopurulent = gonorrhoea/chlamydia)
- Lesions: warts (HPV), ulcers (herpes, syphilis), cysts, prolapse
Cervix:
- Colour and appearance - smooth, ectropion (columnar epithelium on ectocervix - common, especially on OCP)
- OS: nulliparous (small round) vs multiparous (transverse slit)
- Discharge from os
- Nabothian follicles (benign retention cysts)
- Polyps
- Contact bleeding or friable tissue (malignancy until proven otherwise)
- Erosions/ulcers
Samples to collect during speculum exam:
- High vaginal swab (HVS) for candida, BV, trichomoniasis
- Endocervical swab for gonorrhoea and chlamydia (or NAAT)
- Cervical smear (Pap smear / liquid-based cytology) - as per screening schedule
- Colposcopy-directed biopsy if cervical lesion visible
C. Bimanual Pelvic Examination
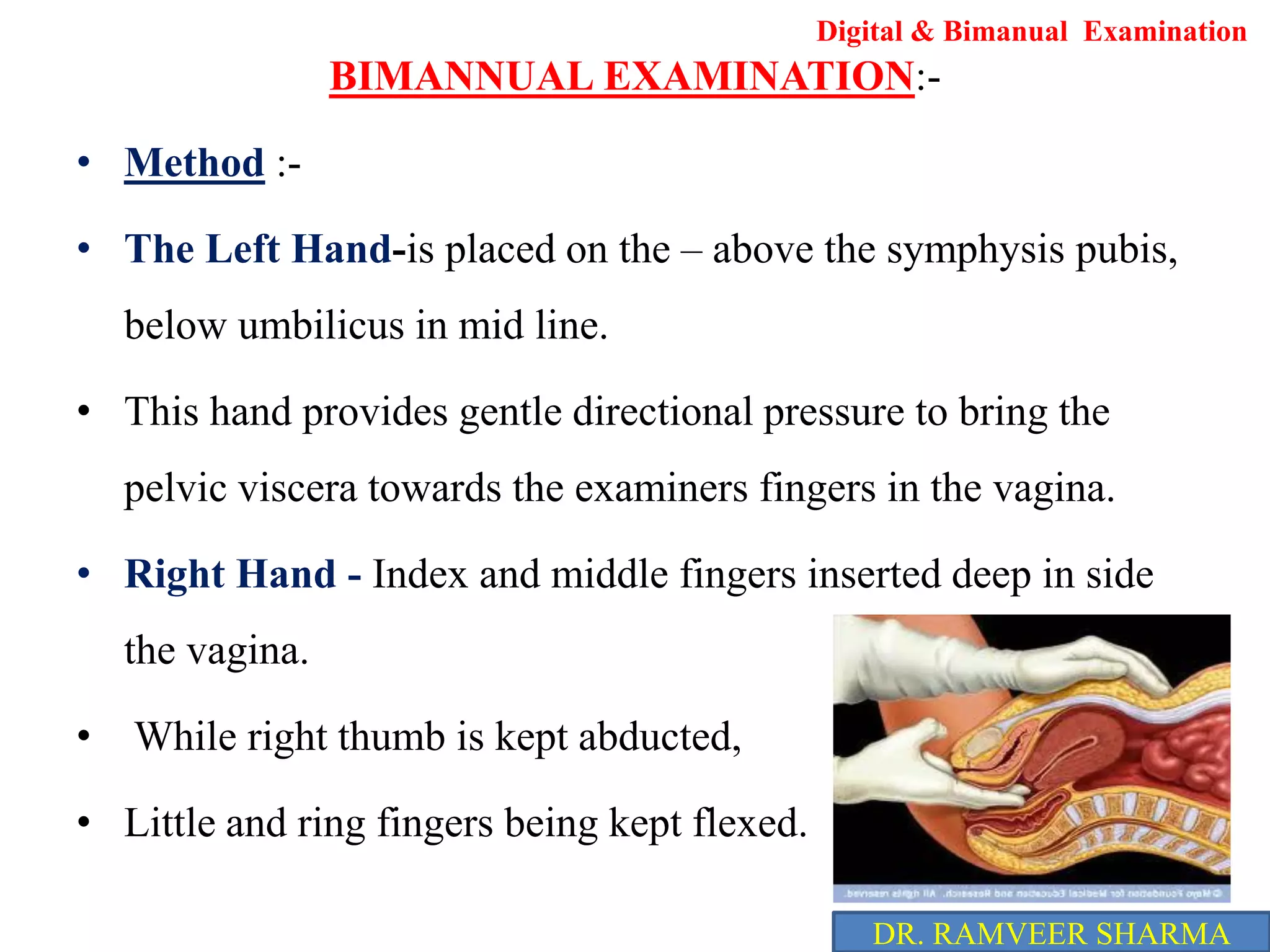
Technique:
- Dominant hand: index and middle fingers lubricated and inserted into the vagina (posteriorly)
- Non-dominant (abdominal) hand: placed suprapubically to bring pelvic organs towards the vaginal fingers
- Right hand in vagina for right-handed examiners; left for left-handed
Systematic palpation:
1. Vagina and Fornices:
- Tenderness of the posterior fornix (pouch of Douglas tenderness = PID, ruptured ectopic, endometriosis)
- Masses in fornices
2. Cervix:
- Consistency: soft (pregnant = Hegar's sign), firm (normal), hard (malignancy)
- Mobility: fixed cervix = endometriosis, malignancy, PID
- Cervical excitation/motion tenderness (CMT): moving the cervix side-to-side causes pain = PID (Chandelier sign)
- Cervical Os: assess dilatation (in miscarriage/labour)
3. Uterus:
- Size: normal uterus is ~8x5x3 cm, pear-shaped; in pregnancy measured in weeks
- Shape: regular (normal) or irregular (fibroids)
- Position:
- Anteverted/anteflexed (most common, ~80%)
- Retroverted/retroflexed (~20% - normal variant; also endometriosis, adhesions)
- Consistency: firm (normal), soft (pregnancy), hard (calcified fibroids, malignancy)
- Mobility: mobile (normal) vs. fixed (malignancy, endometriosis, PID)
- Tenderness: extreme uterine tenderness = PID or ectopic
4. Adnexae (Ovaries and Tubes):
- Each adnexa palpated by moving vaginal fingers to each lateral fornix while abdominal hand pushes downward
- Note: size, shape, mobility, tenderness
- Normal ovaries are approximately 3x2x2 cm - often not palpable, especially in obese patients
- Adnexal mass: cyst (smooth, fluctuant), solid mass (malignancy), tender (ectopic, torsion, TOA)
"The size, shape, mobility, contour, consistency, and position of the uterus are determined. The patient is asked to provide feedback about any areas of tenderness, and her facial expressions are observed during the examination." - Berek & Novak's Gynecology
D. Rectovaginal Examination
Performed when indicated:
- Index finger in vagina, middle finger in rectum simultaneously
- Evaluates:
- Rectovaginal septum - endometriosis deposits, rectovaginal fistula
- Posterior uterine surface - fibroids, adhesions
- Uterosacral ligaments - nodularity = endometriosis
- Posterior cul-de-sac - deposits (ovarian cancer, endometriosis)
- Rectal mucosa - polyps, cancer
- Anal sphincter tone
3.5 Obstetric-Specific Pelvic Examination (Clinical Pelvimetry)
In obstetrics, internal examination also assesses pelvic adequacy:
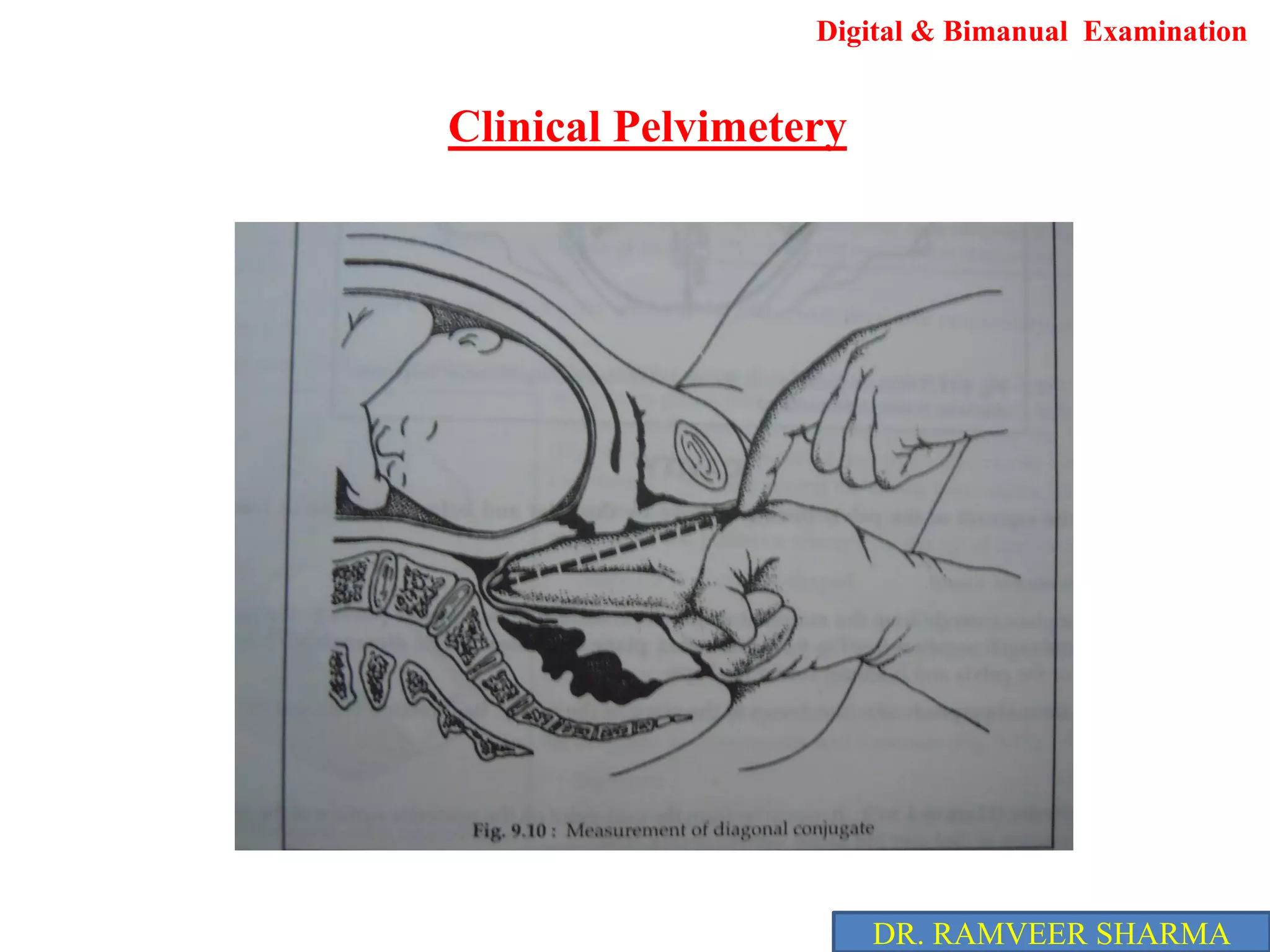
- Diagonal conjugate = distance from the lower border of the symphysis pubis to the sacral promontory (normal ≥12.5 cm); subtract 1.5 cm to get the obstetric conjugate
- Ischial spines - assess their prominence (prominent spines = reduced transverse diameter)
- Sacrum - assess curvature (flat sacrum = reduced AP diameter)
- Subpubic angle - should be ≥90° (narrow angle = android pelvis, unfavourable for vaginal delivery)
- Cervical assessment in labour: dilation (0-10 cm), effacement, consistency, position, station of presenting part (Bishop's score)
3.6 Breast Examination
In obstetrics (antenatal) and routine gynaecology:
Inspection (patient sitting, arms at sides, then raised above head):
- Symmetry and size
- Skin changes: peau d'orange (lymphoedema - malignancy), erythema (mastitis), dimpling
- Nipple: inversion (recent change = malignancy), discharge (colour - bloody = duct papilloma/carcinoma, milky = galactorrhoea, green = duct ectasia), Paget's disease
Palpation (patient supine, arm above head):
- All 4 quadrants + axillary tail
- Use flat of fingers in circular motion
- Any lump: size, shape, consistency (smooth = fibroadenoma/cyst; hard irregular = malignancy), fixity, tenderness
- Nipple discharge: express gently
- Axillary nodes: anterior, posterior, central, apical groups
- Supraclavicular nodes
PART 4 - DOCUMENTATION AND FORMULATION
After history and examination, document clearly:
Obstetric summary example:
"Mrs. X, 28 years, G3P2+0 (2 normal vaginal deliveries, one early miscarriage), 32 weeks gestation by dates, consistent with scan. Baby cephalic, LOA, engaged 4/5. SFH = 31 cm. FHR 140 bpm. BP 130/85, urine protein 1+."
Gynaecological summary example:
"Mrs. Y, 45 years, P2, LMP 2 weeks ago (normal). Presenting with 6-month history of menorrhagia. No IMB, PCB or PMB. No pelvic pain. Speculum: cervix normal, no lesions, smear up to date (normal 2023). Bimanual: uterus 10-12 week size, irregular, mobile, non-tender. No adnexal masses."
PART 5 - COMMON SIGNS AND THEIR SIGNIFICANCE
| Sign | Description | Significance |
|---|---|---|
| Chadwick's sign | Blue-purple discolouration of vaginal mucosa | Early pregnancy (6-8 weeks) |
| Hegar's sign | Softening of the lower uterine segment | Early pregnancy |
| Goodell's sign | Softening of the cervix | Early pregnancy |
| Chandelier sign | Cervical motion tenderness | PID |
| Linea nigra | Darkening of linea alba | Pregnancy |
| Cul-de-sac fullness | Mass/tenderness in pouch of Douglas | Ectopic, PID, endometriosis, ovarian cancer |
| Uterosacral nodularity | Nodules on uterosacral ligaments | Endometriosis |
| Shifting dullness | Fluid wave on percussion of flanks | Ascites (think ovarian malignancy) |
Quick Summary Table
| Section | Key Components |
|---|---|
| History | CC, SOCRATES, Menstrual Hx (PALM-COEIN), Obstetric Hx (GTPAL), Sexual Hx (5P's), Contraceptive Hx, Smear, PMH, DH, FH, SH |
| General Exam | Vitals, BMI, pallor, lymph nodes, thyroid, breasts, cardiovascular |
| Abdominal Exam | IPPA, fundal height, Leopold's maneuvers (in pregnancy), ascites |
| Speculum Exam | External genitalia, vaginal walls, cervix, OS, discharge, swabs, Pap smear |
| Bimanual Exam | Vagina, cervix (position, mobility, CMT), uterus (size/shape/position/mobility/tenderness), adnexae |
| Rectovaginal Exam | Uterosacral ligaments, posterior uterine surface, rectovaginal septum |
| Pelvimetry | Diagonal conjugate, ischial spines, sacrum curvature, subpubic angle |
Sources: Berek & Novak's Gynecology (16th Ed.); Schwartz's Principles of Surgery (11th Ed., Table 41-1); Williams Obstetrics (24th Ed.) via StatPearls (NBK560814); Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.