Tripple assessment of breast with interpretation in details
Reading File
Finding Sources
Finding Sources
Searching PubMed
"triple assessment" AND breast
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
I now have sufficient comprehensive material from authoritative surgical textbooks to construct a detailed answer. Let me compile the complete response.
Triple Assessment of the Breast
The triple assessment of the breast is the gold-standard diagnostic approach for evaluating breast symptoms. It combines three independent components: clinical examination, radiological imaging, and tissue sampling (cytological or histological). When all three components are concordant, the positive predictive value and diagnostic accuracy approaches 100%. It is mandatory for any patient presenting with a breast lump, nipple discharge, skin changes, or other breast symptoms.
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 937
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 962
Component 1 - Clinical Assessment
History
The clinical assessment begins with a thorough history, covering:
- Duration and change in size of the lump
- Relationship to the menstrual cycle (cyclical vs. non-cyclical)
- Associated pain, nipple discharge (character, colour, unilateral/bilateral)
- Skin changes (redness, dimpling, peau d'orange)
- Family history of breast or ovarian cancer
- Hormonal history (OCP, HRT, menarche, menopause, pregnancies)
- Prior breast biopsies or surgery
Clinical Examination Technique
Examination is performed in two stages - inspection followed by palpation:
Inspection (arms by sides, raised above head, pressing on hips):
- Asymmetry or change in breast contour
- Skin dimpling or tethering
- Nipple retraction or inversion (new vs. long-standing)
- Peau d'orange (dermal lymphatic oedema - a sign of locally advanced cancer)
- Erythema or ulceration
Palpation (patient supine, arm raised):
- Use the pad of three fingers (index, middle, ring)
- Apply the dial of a clock method - systematic examination from the periphery inward in a radial pattern (Figure 58.3 shows this technique)
- Axillary, supraclavicular, and infraclavicular nodes must also be palpated

Interpretation of the Lump
| Clinical Feature | Benign | Malignant |
|---|---|---|
| Texture | Soft, rubbery | Hard, stony |
| Margins | Well-defined, smooth | Irregular, ill-defined |
| Mobility | Mobile | Fixed to skin/chest wall |
| Skin overlying | Normal | Tethering, dimpling, peau d'orange |
| Tenderness | Often present | Usually painless |
| Nipple | Normal | Retraction, bloody discharge |
| Nodes | Absent | Firm, matted axillary nodes |
Key rule: the likelihood of malignancy rises sharply with age - from ~10% in women under 40 to ~60% in women over 50 with a palpable mass. Most (~95%) palpable masses are benign overall.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 962
Component 2 - Radiological Imaging
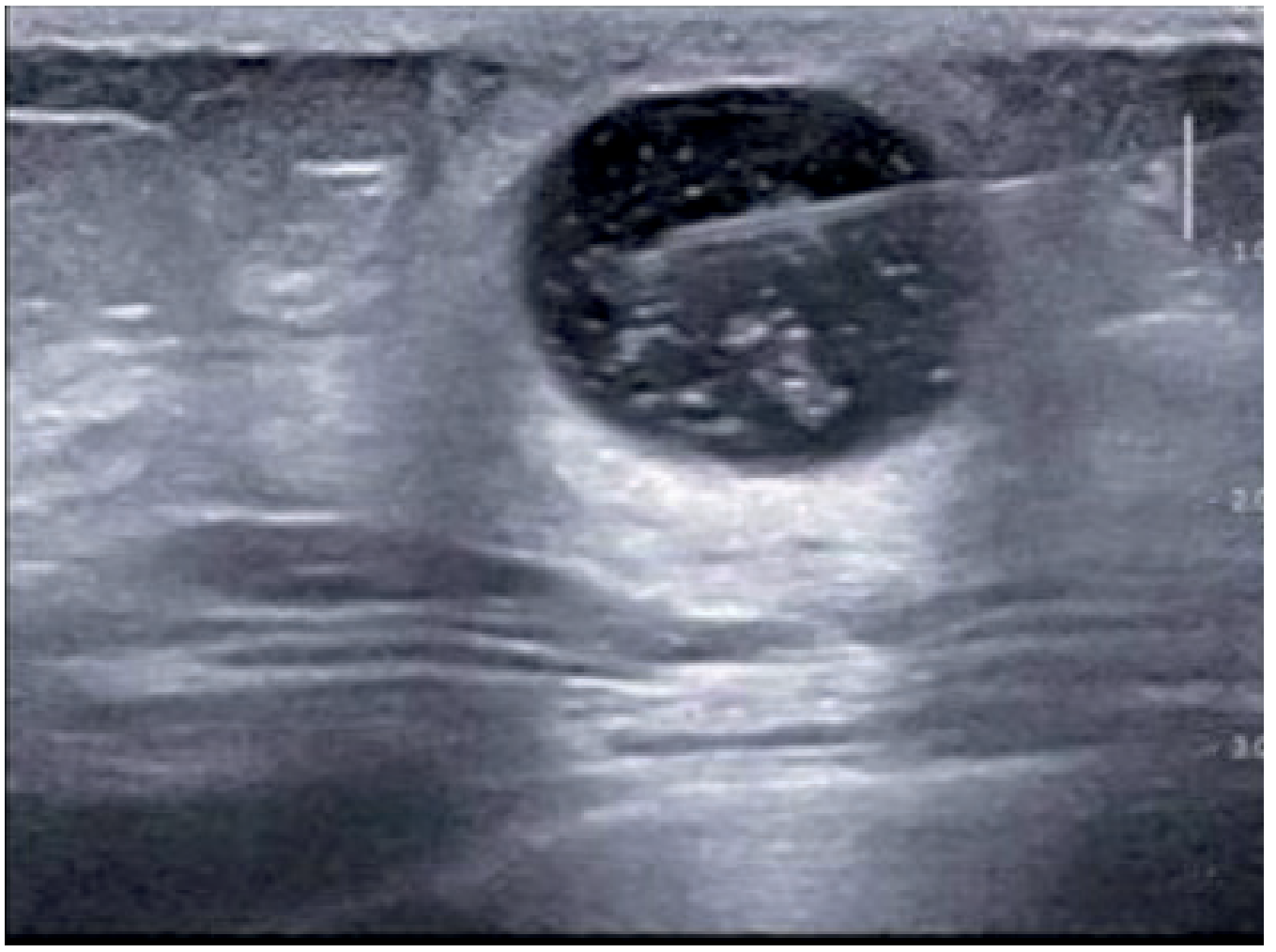
A. Ultrasonography (USG)
USG is the first-line and primary imaging modality in:
- Women under 40 years (dense breast tissue makes mammography hard to interpret)
- Evaluation of a palpable mass in any age group
- Characterising cystic vs. solid lesions
Interpretation of Ultrasonographic Findings:
| Finding | Interpretation | BI-RADS | Action |
|---|---|---|---|
| Anechoic, smooth-walled, no internal echoes | Simple cyst | 2 | Reassure; no further workup |
| Anechoic with debris/internal echoes | Complicated cyst | 2-3 | Aspiration if symptomatic |
| Well-circumscribed, oval, homogeneous, horizontal orientation, wider-than-tall | Fibroadenoma | 3 | Reassure + imaging follow-up |
| Irregular, ill-defined, spiculated or angular margins, vertical orientation | Suspicious for malignancy | 4-5 | Biopsy mandatory |
USG of the axilla is also performed when breast cancer is confirmed, with percutaneous guided biopsy of any suspicious lymph nodes.
B. Mammography
Mammography is the first-line investigation in women over 40 presenting with breast symptoms, and the principal tool for population-based screening. The breast is compressed between plates and exposed to low-voltage X-rays (dose ~1 mGy per film).
Standard Views:
- Mediolateral-oblique (MLO)
- Craniocaudal (CC)
Mammographic Features of Malignancy:
- Spiculated or irregular mass with ill-defined margins
- Clustered pleomorphic microcalcifications (may indicate DCIS)
- Architectural distortion
- Asymmetric density
- Skin thickening or nipple retraction
- Lymphadenopathy (in advanced cases)
Limitations: 10-15% of clinically evident cancers have no visible mammographic abnormality. Sensitivity is significantly reduced in dense breast tissue (BI-RADS C and D density). Mammography is not the first choice in women under 40 due to dense glandular tissue.
Technical Advances:
-
Digital mammography - superior for younger women and dense breasts
-
Digital Breast Tomosynthesis (DBT/3D mammography) - multi-sectional images reducing tissue overlap; shown to improve cancer detection rate (STORM-2 trial, 9,672 patients)
-
Contrast-enhanced mammography (CEM) - IV iodine contrast exploiting tumour neovascularity; approaches MRI accuracy
-
CAD/AI - software-assisted detection to improve sensitivity
-
Sabiston Textbook of Surgery, p. 1874-1880
C. MRI Breast
MRI is a valuable adjunctive (not first-line) tool due to its high sensitivity for invasive breast cancer. It is not routinely used in standard triple assessment but has specific indications:
Indications for MRI:
- High-risk screening (BRCA1/2 carriers, strong family history)
- Extent assessment of known malignancy before surgery (multifocal/multicentric disease)
- Assessment of response to neoadjuvant chemotherapy
- Dense breasts where mammography and USG are inconclusive
- Occult primary with axillary metastasis
- Discordant clinical and imaging findings
- Implant integrity evaluation
The BI-RADS Scoring System (Breast Imaging Reporting and Data System)
Developed by the American College of Radiology (ACR). Applied to mammography, ultrasound, and MRI.
| BI-RADS Score | Category | Recommendation |
|---|---|---|
| 0 | Incomplete - further imaging needed | Additional evaluation |
| 1 | Negative - no abnormality | Routine screening |
| 2 | Benign finding | Routine follow-up, no biopsy |
| 3 | Probably benign (<2% malignancy risk) | 6-month short interval follow-up |
| 4 | Suspicious (2-95% malignancy risk) | Biopsy recommended |
| 4A | Low suspicion | Biopsy |
| 4B | Intermediate suspicion | Biopsy |
| 4C | Moderate-high suspicion | Biopsy |
| 5 | Highly suggestive of malignancy (>95%) | Biopsy mandatory |
| 6 | Known biopsy-proven malignancy | Treatment planning |
Biopsy is required for definitive diagnosis in lesions with BI-RADS 4 or 5.
- Current Surgical Therapy, 14th ed.; Sabiston Textbook of Surgery
Component 3 - Tissue Sampling (Pathology)
A. Fine Needle Aspiration Cytology (FNAC)
A 22-25 gauge needle on a 10-20 mL syringe is passed into the lesion, aspirate is smeared onto glass slides, fixed, and stained (Papanicolaou or May-Grunwald Giemsa).
Cytological Reporting (C-grading system):
| C-Grade | Interpretation | Action |
|---|---|---|
| C1 | Inadequate / acellular specimen | Repeat |
| C2 | Benign - no malignant cells | Reassure if concordant |
| C3 | Atypia, probably benign | Repeat or core biopsy |
| C4 | Suspicious for malignancy | Core biopsy / surgery |
| C5 | Malignant | Treat as malignant if concordant |
Advantages of FNAC:
- Quick, inexpensive, minimally invasive
- Suitable for palpable lumps, superficial nodes, thyroid
- Results available within hours
Limitations of FNAC:
- Cannot distinguish invasive from non-invasive (in situ) carcinoma
- Cannot determine receptor status (ER, PR, HER2) reliably
- High false-negative rate if sample is inadequate
- Operator dependent
B. Core Needle Biopsy (CNB / Tru-cut)
A 14-gauge cutting needle (or vacuum-assisted 8-11G device) is used to obtain a cylinder of tissue for histological analysis, under ultrasound or stereotactic guidance for impalpable lesions.
Histological Reporting (B-grading system):
| B-Grade | Interpretation |
|---|---|
| B1 | Unsatisfactory / normal tissue only |
| B2 | Benign |
| B3 | Uncertain malignant potential (e.g. papilloma, atypical hyperplasia, radial scar) |
| B4 | Suspicious for malignancy |
| B5a | Malignant - in situ (DCIS) |
| B5b | Malignant - invasive |
Advantages over FNAC:
- Histological (architectural) diagnosis
- Can distinguish DCIS from invasive carcinoma
- Allows receptor status (ER, PR, HER2) and Ki-67 assessment
- Supports neoadjuvant treatment planning
- Now the standard of care for tissue diagnosis
Core biopsy specimen allows histology, receptor and genomic analysis, and can identify patients best suited for neoadjuvant systemic treatment.
- Fischer's Mastery of Surgery, 8th ed.; Schwartz's Principles of Surgery, 11th ed.
C. Vacuum-Assisted Biopsy (VAB) and Open Excision Biopsy
- VAB (Mammotome) used for stereotactic biopsy of microcalcifications and small non-palpable lesions; single needle insertion with multiple cores
- Open excision biopsy (wire- or seed-localised) reserved when percutaneous biopsy is non-diagnostic, or to excise B3 lesions
Interpretation and Concordance
The key principle is concordance between all three components. Each component is scored independently; only when results are concordant does the combination achieve near-100% accuracy.
Concordant Benign (C2/B2 + BI-RADS 2-3 + benign clinical features):
- Reassurance and routine follow-up
- No surgery required
Concordant Malignant (C5/B5 + BI-RADS 4-5 + suspicious clinical features):
- Proceed to definitive surgical treatment
- Neoadjuvant chemotherapy if indicated
Discordant Results:
When clinical, imaging, and pathological findings do not agree with each other, the most suspicious result always takes precedence. Discordance mandates:
- Repeat biopsy (preferably core needle)
- Multidisciplinary team (MDT) discussion
- Consider open excision biopsy if still unresolved
The combination of careful clinical assessment, imaging, and biopsy (core biopsy and/or FNAC) identifies >99.5% of breast malignancies in patients with symptomatic breast disease.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 962
Summary: Triple Assessment at a Glance
TRIPLE ASSESSMENT
│
├── 1. CLINICAL
│ History + Inspection + Palpation
│ → P1 (normal) to P5 (malignant)
│
├── 2. IMAGING
│ USG (<40 yrs) / Mammography (>40 yrs) ± MRI
│ → BI-RADS 1-6
│
└── 3. PATHOLOGY
FNAC → C1-C5
Core Biopsy → B1-B5
| Combination | Conclusion |
|---|---|
| All 3 benign | Discharge / routine follow-up |
| All 3 malignant | Definitive treatment |
| Any discordance | MDT review, repeat biopsy, consider excision |
Clinical Indications for Triple Assessment
-
Palpable breast lump (any age)
-
Nipple discharge (especially unilateral, bloody, spontaneous)
-
Nipple retraction (new onset)
-
Skin changes (peau d'orange, dimpling, erythema)
-
Nodular breast (without pain)
-
Mammographic abnormality detected on screening
-
Follow-up of previously treated breast cancer
-
During pregnancy/lactation with a new breast mass
-
Male breast with gynaecomastia needing exclusion of carcinoma
-
Bailey and Love's Short Practice of Surgery, 28th ed., pp. 937-942
-
Grainger & Allison's Diagnostic Radiology, p. 1049
-
Current Surgical Therapy, 14th ed.
This is a shared conversation. Sign in to Orris to start your own chat.