Steps of whippples procedure
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a detailed breakdown of the Whipple procedure (pancreaticoduodenectomy), sourced directly from Fischer's Mastery of Surgery (8th ed.).
Whipple Procedure (Pancreaticoduodenectomy) - Operative Steps
The Whipple is divided into two major phases: Resection and Reconstruction.
Structures Removed
- Head, neck, and uncinate process of the pancreas
- Duodenum (entire)
- Distal stomach (classic Whipple) - preserved in pylorus-preserving variant
- Gallbladder
- Common bile duct (CBD)
- Regional lymph nodes
PHASE 1: RESECTION
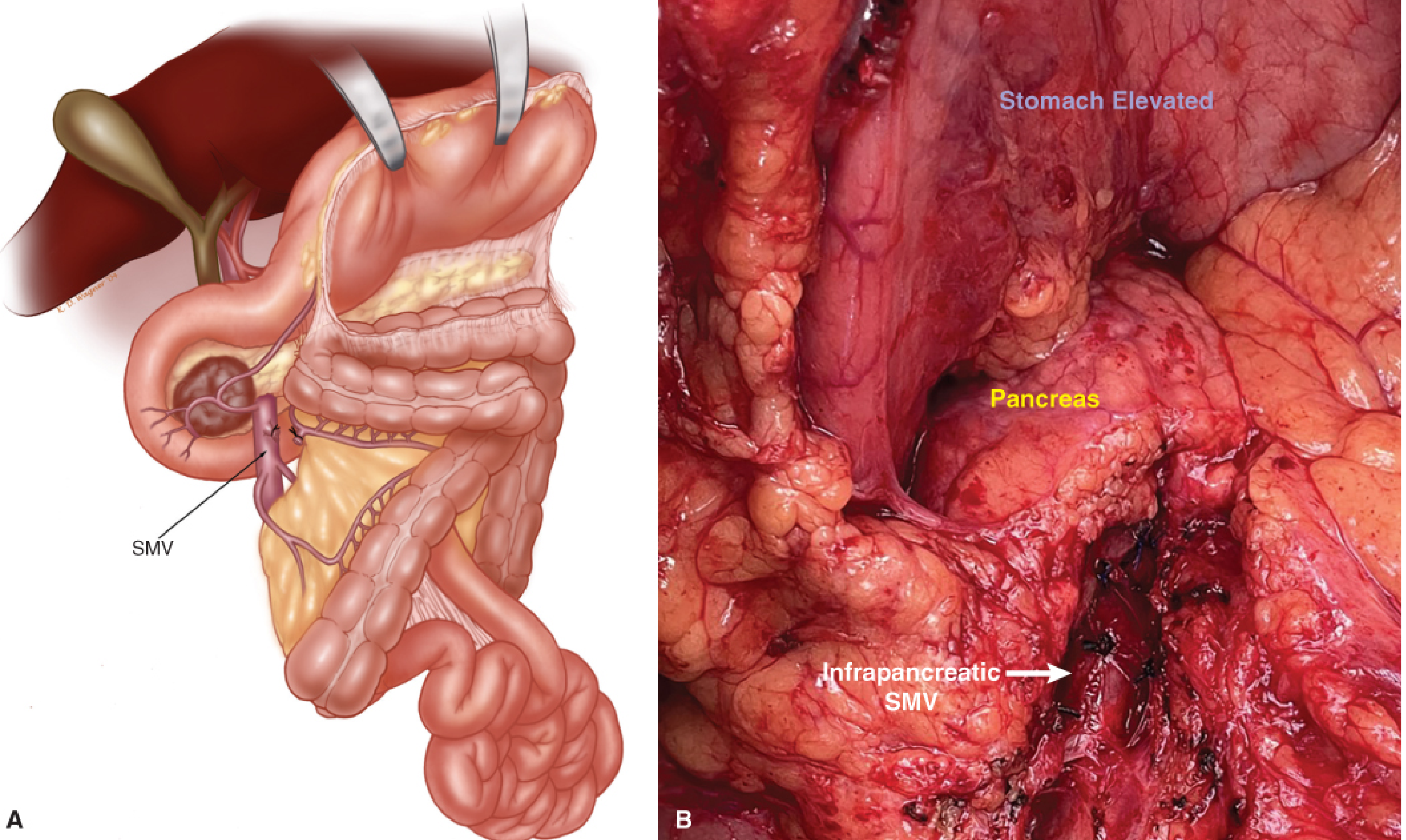
Step 1 - Entry into the Lesser Sac and Identification of the Infrapancreatic SMV
The lesser sac is entered by dividing the gastrocolic omentum off the transverse colon. The posterior wall of the stomach confirms entry. The gastrocolic trunk (trunk of Henle) is carefully identified at the base of the areolar plane - it drains the right gastroepiploic vein, right colic vein, and pancreaticoduodenal veins into the SMV. The trunk is ligated (preserving colic veins if possible) to expose the infrapancreatic SMV.
Step 2 - Hepatoduodenal Ligament Dissection
The hepatoduodenal ligament is dissected. The portal triad is identified:
- Bile duct (lateral/right)
- Hepatic artery (medial/left)
- Portal vein (posterior)
The cystic duct and cystic artery are divided and the gallbladder is taken off the liver bed. The CBD is divided at the level of the hepatic duct bifurcation. Any replaced or accessory right/left hepatic artery from the SMA must be identified at this step to avoid injury. The gastroduodenal artery (GDA) is identified arising from the common hepatic artery, ligated, and divided - this is a key landmark confirming the proper hepatic artery is intact before division.
Step 3 - Antral/Duodenal Division
- Classic Whipple: The stomach is divided at the antrum (distal ~40%) using a linear stapler, preserving the right gastric and right gastroepiploic vessels on the specimen side.
- Pylorus-preserving Whipple (PPPD): The duodenum is divided ~2 cm distal to the pylorus, preserving the entire stomach.
Step 4 - Tunnel Behind the Pancreatic Neck (SMV-PV Tunnel)
A bloodless tunnel is developed posterior to the pancreatic neck, anterior to the SMV-portal vein confluence. A soft silastic drain is passed through this tunnel. This confirms the absence of tumor adherence to the portal vein and establishes the plane for pancreatic transection.
Step 5 - Division of the Jejunum
The proximal jejunum is divided approximately 10-15 cm distal to the ligament of Treitz using a stapler. The mesentery is divided and ligated. The jejunum and duodenum are passed under the mesenteric vessels (posterior to the SMA/SMV) to the right side, delivering them into the operative field with the pancreatic head.
Step 6 - Division of the Pancreatic Neck and SMA Dissection (Uncinate Process)
The pancreatic neck is divided over the SMV-PV tunnel using electrocautery or a scalpel (cold knife preferred for margin). The pancreatic duct is identified. The pancreatic neck margin is sent for frozen section.
The SMV is then retracted medially, exposing the SMA below. A periadventitial dissection plane is developed along the SMA, and all tissue to the right of it (uncinate process) is taken with the specimen. The inferior pancreaticoduodenal artery (IPDA) is identified and suture-ligated - there may be multiple branches. This is the most technically demanding step.
Important: If there is a replaced right hepatic artery (RHA) from the SMA, it must be traced before ligating the IPDA to avoid inadvertent injury.
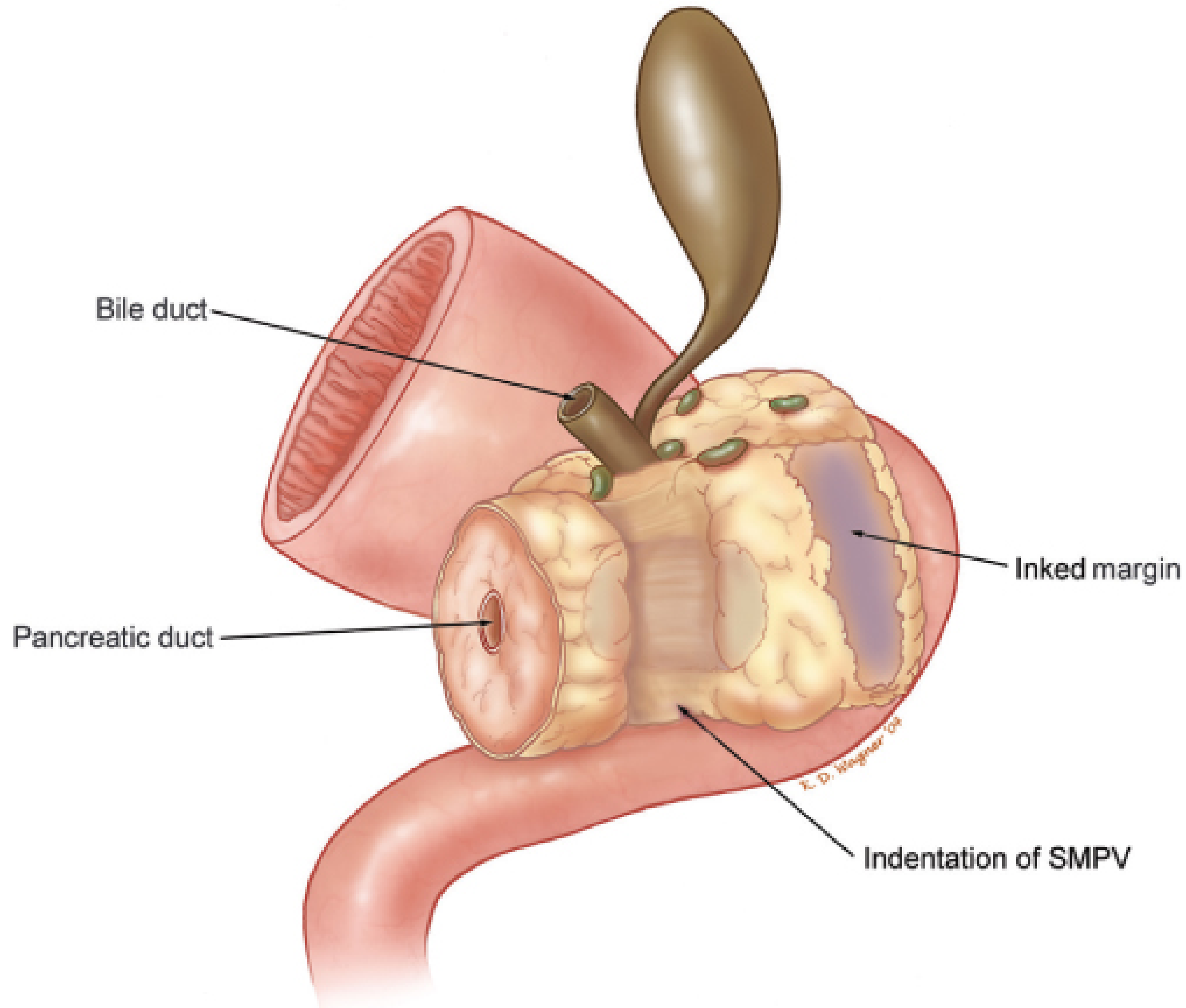
Specimen Removal and Margin Assessment
Once the specimen is freed, margins are assessed:
- Pancreatic neck margin - frozen section
- Bile duct margin - frozen section
- SMA (retroperitoneal/uncinate) margin - inked but NOT sent for frozen section (periadventitial dissection means no tissue remains here)
PHASE 2: RECONSTRUCTION
Reconstruction restores GI, biliary, and pancreatic continuity. A Roux-en-Y configuration with a single jejunal loop is standard. Three anastomoses are performed in sequence from proximal to distal:
Anastomosis 1 - Pancreaticojejunostomy (PJ)
- The most technically demanding anastomosis and the most feared for complications (pancreatic fistula/leak).
- A duct-to-mucosa technique is standard when the pancreatic duct is dilated (>3 mm). An invagination (dunking) technique is used for soft pancreas/small duct.
- A pancreatic stent (internal or external) is often placed across the anastomosis.
- Performed ~10 cm from the cut end of the jejunum.
Anastomosis 2 - Hepaticojejunostomy (HJ)
- The bile duct is anastomosed end-to-side to the jejunum, approximately 10 cm distal to the PJ.
- A single-layer interrupted absorbable suture technique is standard.
- A biliary stent may be placed if the duct is small (<5 mm).
Anastomosis 3 - Gastrojejunostomy (GJ) or Duodenojejunostomy
- The gastric remnant (classic) or pylorus/duodenum (PPPD) is anastomosed to the jejunum ~45-50 cm distal to the HJ.
- A retrocolic (posterior to transverse colon) or antecolic (anterior) position is used - antecolic is generally preferred in the modern era to reduce delayed gastric emptying.
Drain Placement and Closure
- A single surgical drain is placed near (but not directly on) the pancreatic anastomosis.
- The falciform ligament is harvested as a vascularized pedicle flap and placed over the GDA stump to protect against pseudoaneurysm formation from amylase-rich fluid in the event of a PJ leak.
- Omentum (if available) is placed over the pancreaticojejunal anastomosis for reinforcement.
- The abdomen is closed in standard fashion.
Summary Table
| Phase | Step | Key Action |
|---|---|---|
| Resection | 1 | Enter lesser sac, expose infrapancreatic SMV |
| Resection | 2 | Dissect hepatoduodenal ligament, divide CBD, cholecystectomy |
| Resection | 3 | Divide stomach (classic) or proximal duodenum (PPPD) |
| Resection | 4 | Create SMV-PV tunnel posterior to pancreatic neck |
| Resection | 5 | Divide proximal jejunum, pass under mesenteric vessels |
| Resection | 6 | Divide pancreatic neck, dissect uncinate/SMA margin, IPDA ligation |
| Reconstruction | 1 | Pancreaticojejunostomy (duct-to-mucosa or dunking) |
| Reconstruction | 2 | Hepaticojejunostomy (~10 cm distal to PJ) |
| Reconstruction | 3 | Gastrojejunostomy or duodenojejunostomy (~45-50 cm distal to HJ) |
| Closure | - | Drain near PJ, falciform flap over GDA stump |
Source: Fischer's Mastery of Surgery, 8th ed. - Chapter 183 (Pancreaticoduodenectomy)
According to sabiston
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Content
"The first step" in /textbooks/9780443124341
Finding Sources
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Pds suture
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.