Periodic breathing
Reading File
Finding Sources
Finding Sources
Searching PubMed
"periodic breathing" OR "Cheyne-Stokes" respiration
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Here it is:
Periodic Breathing
Periodic breathing is a recurring, cyclical pattern of respiration in which the depth and/or rate of breathing waxes and wanes, often punctuated by brief episodes of apnea (cessation of breathing). The most clinically recognized form is Cheyne-Stokes respiration (CSR).
Definition
- Alternating periods of hyperpnea (increased breathing) and apnea (no breathing) in a rhythmic cycle
- In infants: three or more respiratory pauses >3 seconds duration, with <20 seconds between pauses, without associated bradycardia or cyanosis - this distinguishes it from true apnea
- Apnea is defined separately as a respiratory pause >20 seconds (may include bradycardia/hypoxia)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Cheyne-Stokes Respiration
CSR is the classic disease-associated form of periodic breathing: slowly waxing and waning respiration occurring every 40-90 seconds, with crescendo-decrescendo tidal volumes followed by apnea, then repeat.
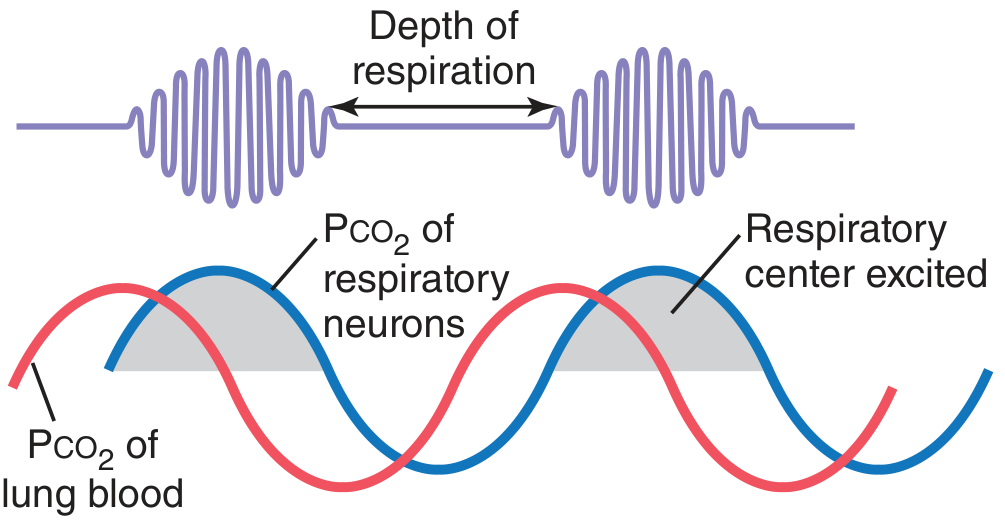
Figure: Cheyne-Stokes breathing. PCO₂ of pulmonary blood (red line) changes in advance of PCO₂ of the respiratory neurons (blue line). The respiratory center is excited only when the neuronal PCO₂ rises above threshold. - Guyton and Hall Textbook of Medical Physiology
Pathophysiology
The fundamental mechanism is an unstable feedback loop in respiratory control. Under normal conditions, blood and tissue buffers "damp" oscillations so they die out - but two specific conditions override this damping:
1. Prolonged Lung-to-Brain Circulation Time (Circulatory Delay)
In states like heart failure, blood flow is slow. When a patient hyperventilates:
- Pulmonary blood PCO₂ drops, PO₂ rises
- But the changed blood takes much longer than normal to reach the brainstem respiratory center
- During this transit delay, ventilation continues lowering alveolar PCO₂ further
- When the low-PCO₂ blood finally arrives at the brain, it oversuppresses the respiratory center → apnea
- During apnea, CO₂ builds up and O₂ falls; again with delay, this reaches the brain and overstimulates breathing
- The cycle repeats
- Guyton and Hall Textbook of Medical Physiology, p. 539
2. Increased Feedback Gain (Hypersensitivity to CO₂)
Damage to respiratory control areas (brain disease, stroke, encephalopathy) can cause an exaggerated ventilatory response to CO₂ - a 10-20-fold increase in ventilation for a 3 mmHg rise in PCO₂ (normally only 2-3-fold). This oscillatory instability alone is sufficient to produce CSR, even without circulatory delay. This form is often a sign of severe brain dysfunction and can be a prelude to death.
- Guyton and Hall, p. 539; Ganong's Review of Medical Physiology, p. 666
Demonstrating Periodic Breathing (Voluntary Hyperventilation Model)
If a normal person voluntarily hyperventilates for 2-3 minutes and then stops:
- Apnea follows - because CO₂ has been "washed out"
- Shallow breaths occur when hypoxia stimulates carotid/aortic chemoreceptors (before PCO₂ has normalized)
- Apnea again as those few breaths eliminate the hypoxic stimulus
- The cycle continues until PCO₂ gradually returns to normal
This does not occur if the hyperventilation is done with a 5% CO₂ mixture, confirming the mechanism is CO₂-dependent.
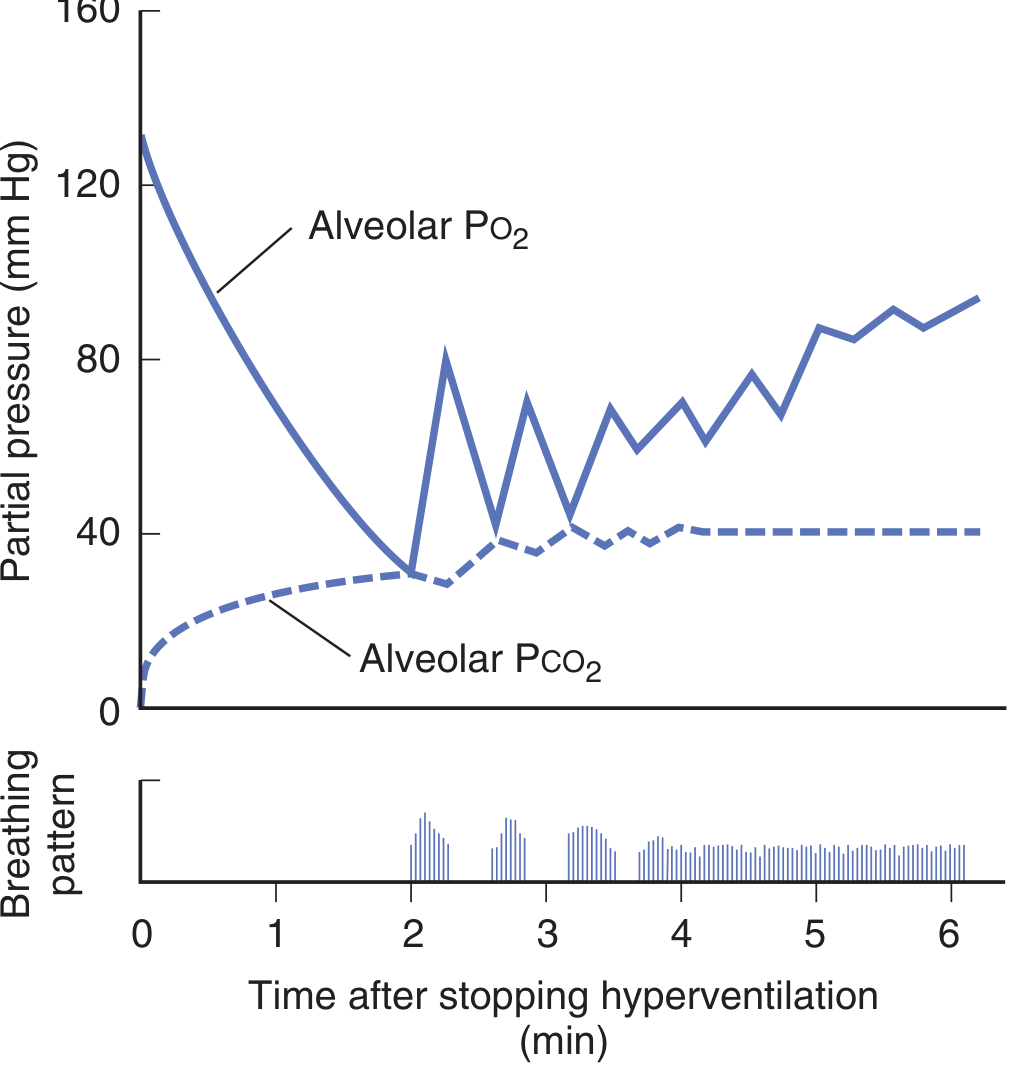
Figure: Changes in alveolar air composition and breathing pattern after 2 minutes of forced hyperventilation. Bars = breathing; blank spaces = apnea. - Ganong's Review of Medical Physiology
Causes / Conditions Associated with Periodic Breathing
| Condition | Mechanism |
|---|---|
| Heart failure (CHF) | Prolonged circulation time (most common cause of CSR) |
| Uremia | Metabolic encephalopathy |
| Brain damage / stroke / encephalopathy | Increased chemosensitivity / disrupted inhibitory pathways |
| High altitude | Hypoxia-driven hyperventilation → hypocapnia → apneic threshold crossed |
| Normal sleep (some individuals) | Reduced CO₂ threshold during sleep |
| Prematurity (infants) | Immature respiratory control centers |
- Ganong's Review of Medical Physiology; Fishman's Pulmonary Diseases and Disorders; Bradley and Daroff's Neurology in Clinical Practice
High-Altitude Periodic Breathing
A physiologically distinct but mechanistically similar form occurs in healthy individuals above ~2000 m:
- Hypoxia stimulates peripheral chemoreceptors (carotid body) → hyperventilation → PCO₂ falls
- The apneic threshold during sleep is reached → central apnea
- Because detection by peripheral chemoreceptors is rapid (short delay), the cycle time is short: 12-34 seconds (compared to 40-90 s in CSR)
- Worsens with altitude; above 5500 m, the breathing frequency is so high apneas paradoxically decrease
- Gender difference: Women have significantly fewer central sleep apnea events than men at altitude (3400 m and 5400 m)
- With acclimatization, periodic breathing diminishes at moderate altitudes (<3000 m) but may persist for over a week at higher altitudes
- Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine
Periodic Breathing in Infants
- More common in premature infants
- Cyclic episodes during sleep: brief apneic pauses of 5-10 seconds interrupt regular breathing, followed by a burst of rapid respiration
- Idiopathic apnea of prematurity treatment: caffeine (standard; early caffeine therapy also associated with better neurodevelopmental outcomes in infants <29 weeks)
- Hypoxic periods require supplemental O₂
- Periodic breathing itself is considered benign; it is the apneic episodes (>20 s) that carry risk
- Bradley and Daroff's Neurology in Clinical Practice
Treatment
| Form | Treatment |
|---|---|
| CSR / Heart failure | Treat underlying cardiac failure; CPAP/ASV; beta blockers |
| High-altitude periodic breathing | Acetazolamide (raises the PCO₂ needed to produce apnea, i.e., shifts the apneic threshold); supplemental O₂ |
| Apnea of prematurity | Caffeine (adenosine receptor antagonist - stimulates respiratory drive) |
| CSR due to brain injury | Supportive; treat underlying cause |
- Fishman's Pulmonary Diseases and Disorders; Kaplan and Sadock's Synopsis of Psychiatry; Bradley and Daroff's Neurology in Clinical Practice
Key Points Summary
- Periodic breathing = oscillating respiratory drive due to unstable CO₂/O₂ feedback
- The core mechanism is either circulatory delay (heart failure) or increased chemoresponsiveness (brain disease)
- CSR cycle: 40-90 s; high-altitude periodic breathing cycle: 12-34 s
- Arousals in CSR occur during the hyperpneic phase (peak of ventilation), not at apnea termination
- Normal damping prevents periodic breathing in healthy individuals at sea level
- Always consider the underlying cause when evaluating periodic breathing in a patient
A person finds it difficult to recognize visual scenes, sounds, and meaningful articulation of words in spite of normal somatic, visual and auditory senses. 1) Name clinical condition. 2) Write probable cortical area affected.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative information from multiple neurology textbooks. Here is the complete answer:
1. Clinical Condition: Agnosia
Agnosia is defined as the inability to recognize objects, persons, or sensory stimuli in the absence of a primary deficit in the sensory modality itself - i.e., the basic senses (sight, hearing, touch) are intact, but the brain cannot attach meaning or identity to what is perceived.
The scenario describes three simultaneous forms of agnosia:
| Symptom | Specific Agnosia |
|---|---|
| Cannot recognize visual scenes despite normal vision | Visual Agnosia (specifically Associative Visual Agnosia) |
| Cannot recognize environmental sounds despite normal hearing | Auditory Agnosia (Agnosia for sounds) |
| Cannot recognize meaningful words in speech despite normal hearing | Auditory Verbal Agnosia = Pure Word Deafness |
Together, this presentation represents multimodal agnosia - failure of the association cortices to interpret and give meaning to incoming sensory information.
2. Probable Cortical Areas Affected
The key distinction is that primary sensory cortices are intact - only the unimodal (secondary) and multimodal association cortices are damaged.
Visual Agnosia
- Brodmann Areas 18 & 19 (secondary visual / visual association cortex, occipital lobe)
- More specifically, ventral stream / inferotemporal cortex (the "what" pathway for object identification)
- Lesions here disrupt the ability to assign meaning to perceived visual stimuli
- "Ventral lesions involving the inferotemporal cortex produce defects in recognition (agnosia)" - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Auditory Agnosia (for environmental sounds / music)
- Secondary auditory cortex - Brodmann Areas 21 & 22 (superior and middle temporal gyri)
- Particularly right temporal lobe (non-dominant hemisphere) for non-verbal sound recognition
- "Lesions of the secondary (unimodal association) zones of the auditory cortex - area 22 and part of area 21 - have no effect on perception of sounds and pure tones. However, appreciation of complex combinations of sounds is severely impaired. This impairment (auditory agnosia) takes several forms: inability to recognize sounds, different musical notes, or words" - Adams & Victor's Principles of Neurology
Pure Word Deafness (Auditory Verbal Agnosia)
- Left superior temporal gyrus / Brodmann Area 22 (Wernicke's area region)
- "Patients with pure word deafness generally have bilateral lesions of the association cortex more anteriorly in the superior temporal gyrus, although unilateral left lesions, presumably disconnecting left from right cortices by subcortical damage, are also reported" - Kaplan & Sadock
- This is a failure of the left temporal lobe to decode acoustic signals of speech and convert them into understandable words
Summary Diagram
Primary Sensory Cortices (INTACT) Association Cortices (DAMAGED)
─────────────────────────────────────────────────────────────────────────
Visual → BA 17 (calcarine) = normal → BA 18, 19 + inferotemporal = LESION
→ Visual Agnosia
Auditory → BA 41, 42 (Heschl) = normal → BA 22, 21 (R > L) = LESION
→ Auditory Agnosia (sounds/music)
Auditory → BA 41, 42 (Heschl) = normal → BA 22 (Left superior temporal) = LESION
→ Pure Word Deafness
The overarching concept is that all primary sensory areas are preserved - the patient can see, hear, and feel - but the unimodal association cortices that integrate and assign meaning to these percepts are damaged, preventing recognition.
- Adams and Victor's Principles of Neurology, 12th Ed.
- Bradley and Daroff's Neurology in Clinical Practice
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Localization in Clinical Neurology, 8e
Describe baroreceptors and their role in regulation of blood pressure.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, authoritative content from multiple textbooks with excellent diagrams. Here is the full answer:
Baroreceptors and Their Role in Blood Pressure Regulation
1. Definition
Baroreceptors (also called pressoreceptors) are spray-type mechanoreceptor nerve endings located in the walls of large arteries. They are stretch-sensitive - when arterial pressure rises, the arterial wall stretches and activates them; when pressure falls, stretch decreases and they become less active. They form the afferent limb of the most powerful short-term neural mechanism for blood pressure control.
2. Location and Anatomy
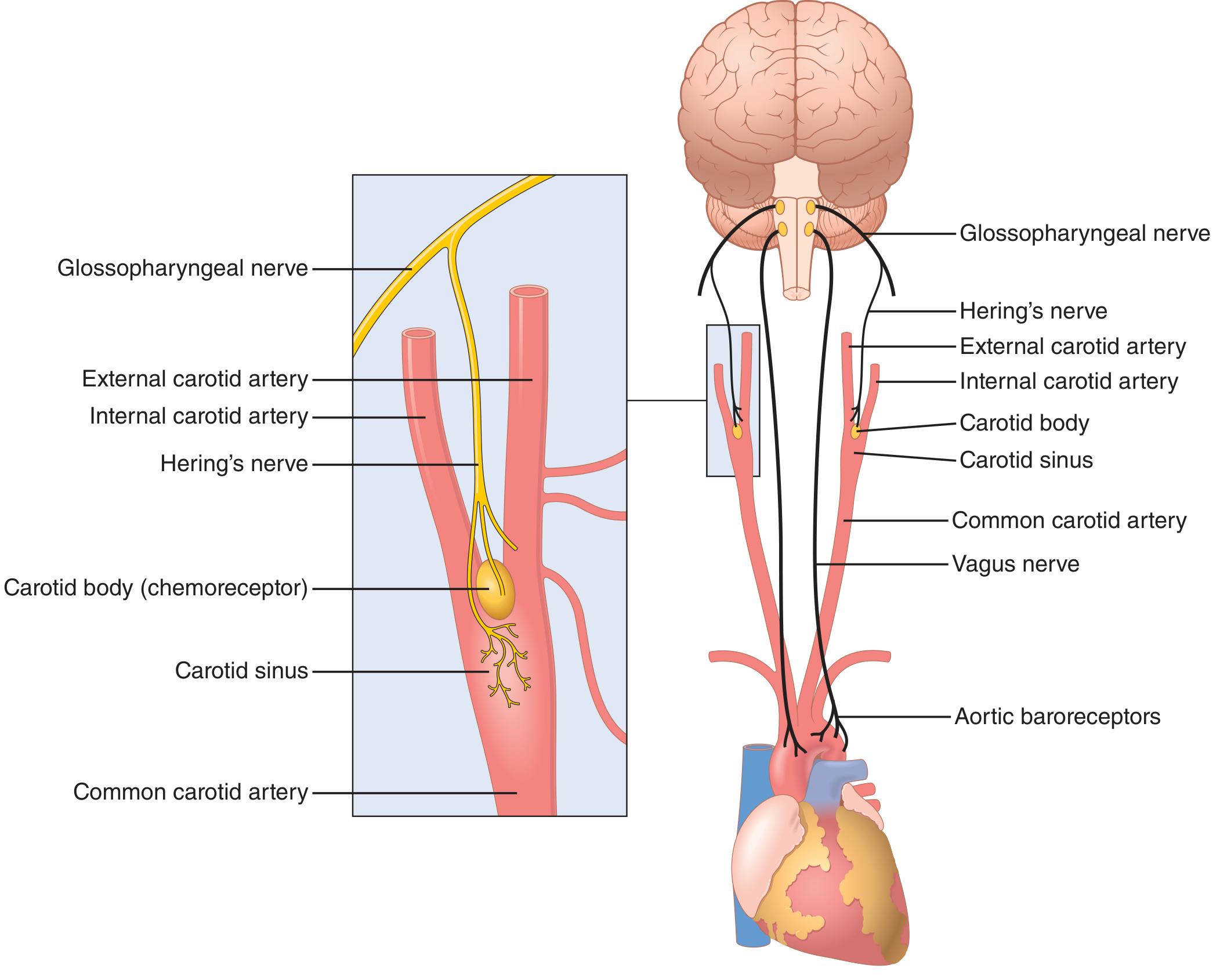
Figure: Baroreceptor system for controlling arterial pressure. - Guyton and Hall Textbook of Medical Physiology
Baroreceptors are present in the walls of almost all large thoracic and neck arteries, but are most concentrated at two critical sites:
| Location | Details |
|---|---|
| Carotid Sinus | Wall of each internal carotid artery, just above the carotid bifurcation; most sensitive and most studied |
| Aortic Arch | Wall of the aortic arch; functionally similar but operates at pressures ~30 mmHg higher than carotid receptors |
Afferent Pathways
- Carotid sinus baroreceptors → Hering's nerve → Glossopharyngeal nerve (CN IX) → Nucleus Tractus Solitarius (NTS), medulla
- Aortic arch baroreceptors → Vagus nerve (CN X) → Nucleus Tractus Solitarius (NTS), medulla
- Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition
3. Mechanism of Action
Baroreceptors are mechanoreceptors sensitive to pressure (stretch):
- A rise in arterial pressure → increased wall stretch → depolarizing receptor potential → increased action potential firing rate in afferent nerves
- A fall in arterial pressure → decreased stretch → hyperpolarizing receptor potential → decreased firing rate
Key properties:
- They are more sensitive to pulsatile pressure than to constant (non-pulsatile) pressure
- They are most sensitive to rapid changes in pressure - a fast pressure rise produces far more firing than a gradual one at the same level
- Threshold: ~50 mmHg (below this, carotid baroreceptors are silent)
- Maximum firing: ~180-200 mmHg
- Maximum sensitivity (steepest ΔI/ΔP): around the normal operating range of ~100 mmHg - exactly where it is most needed
- Ganong's Review of Medical Physiology, 26th Edition
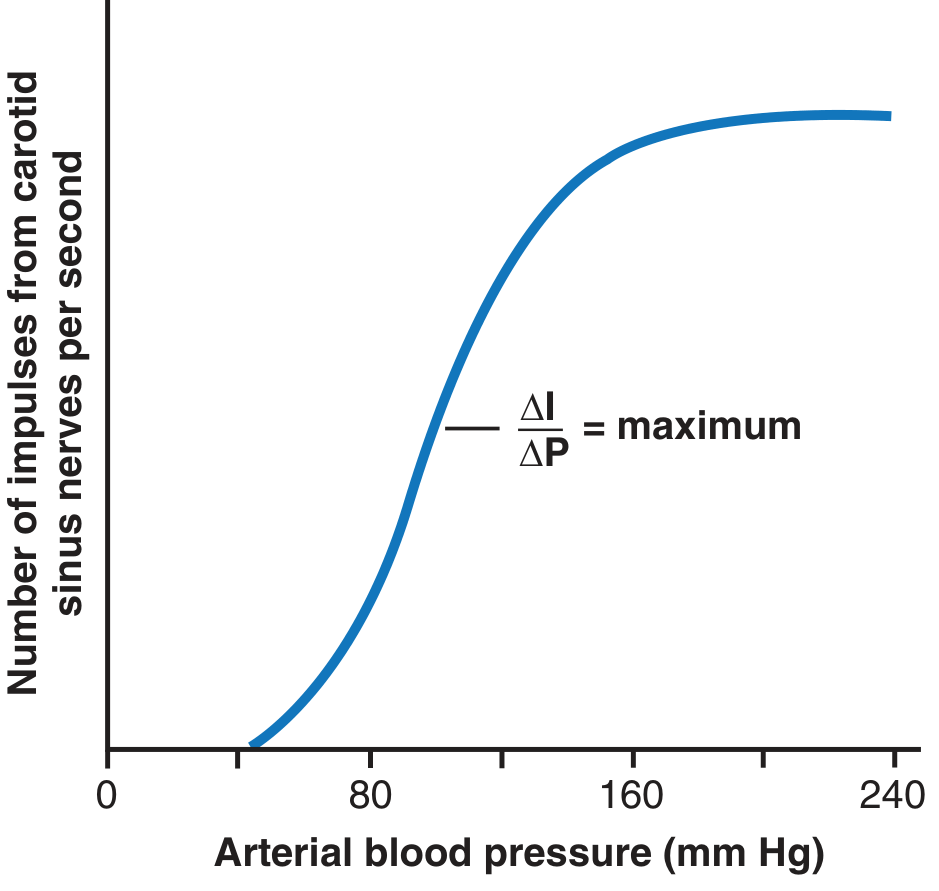
Figure: Activation of baroreceptors at different arterial pressure levels. Maximum sensitivity (ΔI/ΔP) occurs in the normal range. - Guyton and Hall Textbook of Medical Physiology
4. The Baroreceptor Reflex Arc
The complete reflex arc is a negative feedback loop:
Arterial Pressure Change
↓
Baroreceptor Stretch (in carotid sinus / aortic arch)
↓
Afferent signals (CN IX / CN X)
↓
Nucleus Tractus Solitarius (NTS), Medulla
↓
Vasomotor Center + Vagal Center (integration)
↓
Efferent ANS output (sympathetic ↑↓ / parasympathetic ↑↓)
↓
Heart + Blood Vessels
↓
Corrected Arterial Pressure
5. Reflex Responses
A. When Blood Pressure RISES (e.g., sudden standing from lying, exercise, hypertensive surge)
- Baroreceptor firing increases
- Signals enter NTS → inhibit the vasomotor (vasoconstrictor) center + excite the vagal parasympathetic center
- Result:
- Vasodilation of arterioles → decreased peripheral resistance (decreased TPR)
- Vasodilation of veins → decreased venous return
- Decreased heart rate (vagal bradycardia)
- Decreased cardiac contractility
- Net effect: Blood pressure falls back toward normal
B. When Blood Pressure FALLS (e.g., hemorrhage, standing up, shock)
- Baroreceptor firing decreases
- Reduced inhibition of vasomotor center → increased sympathetic outflow; vagal tone decreases
- Result:
- Arteriolar vasoconstriction → increased TPR
- Venous constriction → increased venous return → increased cardiac output
- Increased heart rate (tachycardia)
- Increased cardiac contractility
- Adrenal medulla stimulated → circulating epinephrine released
- Net effect: Blood pressure rises back toward normal
- Costanzo Physiology 7th Edition (Table 4.9: Summary of cardiovascular responses to hemorrhage)
6. The "Pressure Buffer" Function
Because the baroreceptor system opposes both increases and decreases in arterial pressure, the afferent nerves from baroreceptors are called buffer nerves and the whole system is the pressure buffer system.
Experimental evidence (Guyton, Cowley, Liard):
- In a normal dog: mean arterial pressure stays within 85-115 mmHg throughout a 24-hour day
- After baroreceptor denervation: pressure fluctuated from <50 mmHg to >160 mmHg with routine activities (lying down, eating, defecation, noise)
- The baroreceptor system reduces minute-by-minute pressure variation to about one-third of what it would be without the system
- Guyton and Hall Textbook of Medical Physiology, p. 228
7. Practical Importance
| Situation | Role of Baroreceptors |
|---|---|
| Orthostatic hypotension | Immediate sympathetic discharge when standing prevents syncopal drop in cerebral perfusion |
| Hemorrhage / shock | Reflex tachycardia + vasoconstriction; reflex becomes impaired when BP falls below 50 mmHg |
| Carotid sinus massage | Increases baroreceptor firing → reflex bradycardia; used clinically to terminate SVT |
| Carotid sinus hypersensitivity | Hyperactive reflex → excessive bradycardia / hypotension on neck palpation |
8. Baroreceptor Resetting
A critically important limitation:
- If arterial pressure remains elevated for 1-2 days, baroreceptors reset - their firing rate returns toward normal even though the pressure remains high
- They then defend the new (elevated) pressure rather than correcting it
- This explains why baroreceptors are primarily a short-term (moment-to-moment) pressure regulator
- However, they do not reset completely; they may contribute to long-term control by modulating renal sympathetic nerve activity → affecting Na⁺ and water excretion → affecting blood volume
"If the arterial pressure rises from 100 to 160 mm Hg, a very high rate of baroreceptor impulses is at first transmitted. During the next few minutes, the rate diminishes considerably, then more slowly over the next 1 to 2 days, returning to nearly normal despite the mean arterial pressure still remaining at 160 mm Hg."
- Guyton and Hall Textbook of Medical Physiology
Summary
| Feature | Detail |
|---|---|
| Type | Spray-type mechanoreceptors (stretch-sensitive) |
| Location | Carotid sinus (CN IX) + Aortic arch (CN X) |
| CNS relay | Nucleus Tractus Solitarius, medulla |
| Operating range | ~50-200 mmHg; most sensitive at ~100 mmHg |
| Stimulus | Pulsatile pressure; most sensitive to rapid changes |
| High BP response | ↓ HR, ↓ contractility, vasodilation → ↓ BP |
| Low BP response | ↑ HR, ↑ contractility, vasoconstriction → ↑ BP |
| Primary role | Short-term, rapid blood pressure stabilization |
| Limitation | Reset over 1-2 days; limited long-term efficacy |
- Guyton and Hall Textbook of Medical Physiology
- Ganong's Review of Medical Physiology, 26th Edition
- Costanzo Physiology, 7th Edition
- Miller's Anesthesia, 10th Edition
Pace maker potential and its ionic basis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have everything needed for a complete, authoritative answer. Here it is:
Pacemaker Potential and Its Ionic Basis
1. What Is the Pacemaker Potential?
The pacemaker potential (also called the prepotential or phase 4 spontaneous depolarization) is the slow, progressive rise in membrane potential that occurs in SA node cells between action potentials. It is the ionic mechanism responsible for automaticity - the ability of SA node cells to spontaneously generate action potentials without any external neural stimulus.
Unlike ventricular or atrial muscle cells (which have a stable resting membrane potential at -85 to -90 mV), SA node cells have an unstable resting potential that continuously drifts upward toward threshold, triggering the next action potential automatically.
2. Comparison: SA Node vs. Ventricular Action Potential
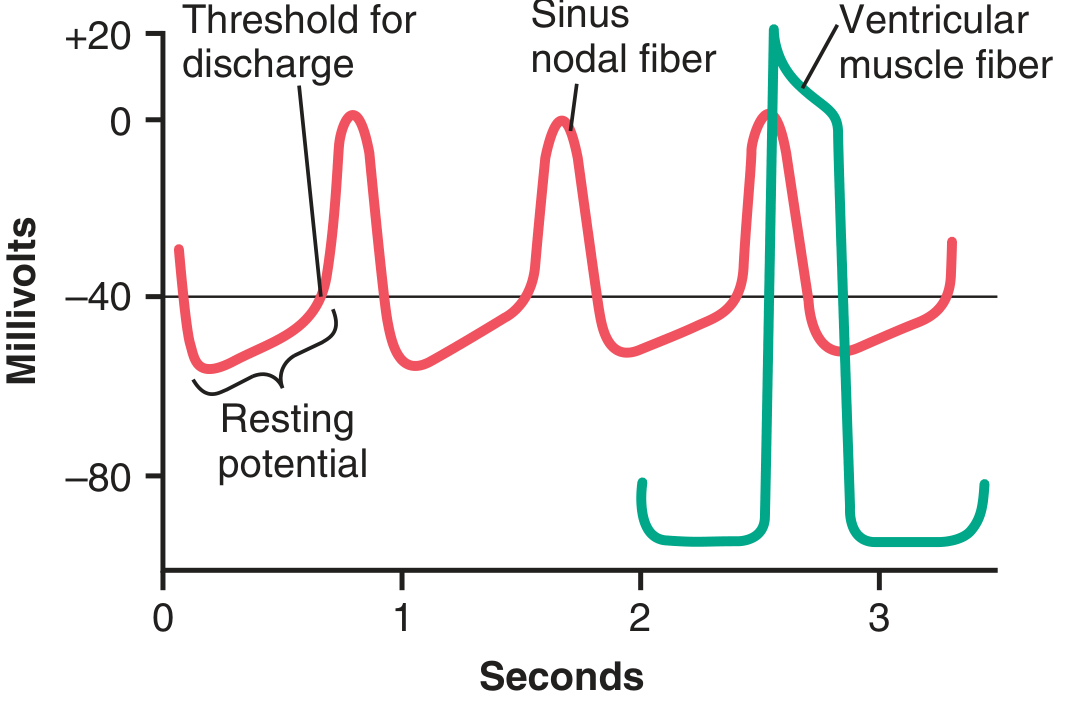
Figure: Rhythmical discharge of a sinus nodal fiber compared with a ventricular muscle fiber action potential. - Guyton and Hall Textbook of Medical Physiology
| Feature | SA Node | Ventricular Muscle |
|---|---|---|
| Resting membrane potential | -55 to -60 mV | -85 to -90 mV |
| Threshold for discharge | ~-40 mV | ~-65 to -70 mV |
| Phase 4 | Slow upward drift (pacemaker potential) | Stable flat line |
| Phase 0 upstroke | Slow, Ca²⁺-dependent | Rapid, Na⁺-dependent |
| Phases 1 & 2 | Absent | Present |
| Automaticity | Yes | No |
3. Phases of the SA Node Action Potential
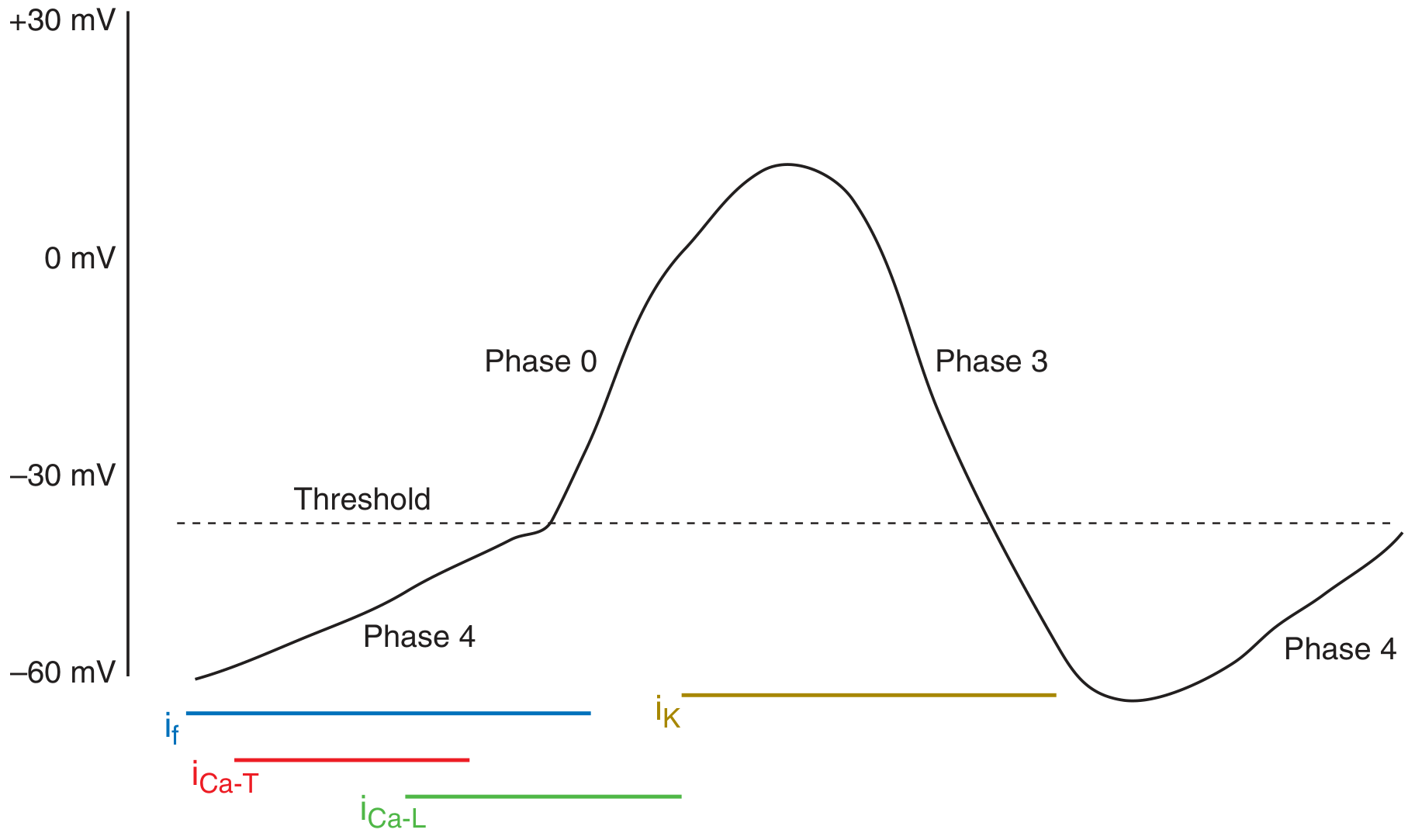
Figure: Cellular ion currents involved in depolarization and automaticity of SA nodal pacemaker cells. - Harrison's Principles of Internal Medicine, 22nd Edition
Phase 4 - The Pacemaker Potential (Prepotential)
This is the most important phase for understanding automaticity.
Maximum diastolic potential (MDP): The most negative value reached is approximately -65 mV (after repolarization from the previous action potential).
From this point, the membrane potential spontaneously drifts upward due to three sequential ionic events:
Step 1: I_f - "Funny" Current (Na⁺ inward, activated on repolarization)
- The dominant initial current responsible for the pacemaker potential
- Carried by HCN (Hyperpolarization-activated Cyclic Nucleotide-gated) channels - a mixed Na⁺/K⁺ channel
- Called "funny" because - unlike all other voltage-gated channels - it is activated by hyperpolarization (opens when the cell repolarizes to -60 mV), not depolarization
- Carries primarily inward Na⁺ current (with some K⁺)
- Turns on immediately after repolarization of the preceding action potential, ensuring each SA node beat is followed by another
- Begins the slow depolarization from MDP
Step 2: I_Ca-T - T-type ("Transient") Calcium Current
- As I_f depolarizes the membrane toward ~-50 mV, T-type Ca²⁺ channels (low-threshold, transient) open
- Inward Ca²⁺ current - adds to the depolarizing drive
- Called "T-type" because they are transient and activate at low (more negative) voltages
- Contributes to acceleration of the pacemaker potential slope in its mid-to-late phase
Step 3: Decay of I_K - Potassium Current (K⁺ outward, decreasing)
- After the previous action potential, K⁺ channels opened during repolarization
- These K⁺ channels progressively close during phase 4
- As outward K⁺ current decreases, it no longer opposes the inward Na⁺ and Ca²⁺ currents
- This removal of repolarizing influence contributes to the net inward drift of the membrane potential
Together, these three currents cause the membrane potential to rise from -65 mV to the threshold of approximately -40 mV.
Phase 0 - Upstroke
- Once threshold (-40 mV) is reached, L-type ("Long-lasting") Ca²⁺ channels open
- Rapid inward Ca²⁺ current produces the action potential upstroke
- Fast Na⁺ channels are absent (or inactivated at the less negative resting potential of SA node) - this is why the upstroke is slower and smaller than in ventricular cells
- T-type channels also contribute to the early upstroke
Phases 1 & 2 - Absent in SA Node
Phase 3 - Repolarization
- L-type Ca²⁺ channels inactivate (~100-150 ms after opening)
- Simultaneously, K⁺ channels (I_K) open massively → large outward K⁺ current
- These two effects together repolarize the cell back to MDP
- K⁺ channels remain open briefly beyond repolarization → hyperpolarization to -55 to -60 mV
- Then I_f activates again and the next cycle begins
4. Complete Ionic Summary
| Phase | Ion Current | Channel Type | Direction | Effect |
|---|---|---|---|---|
| Phase 4 (early) | I_f (funny current) | HCN channels (Na⁺/K⁺ mixed) | Inward Na⁺ | Begins depolarization |
| Phase 4 (mid) | I_Ca-T | T-type Ca²⁺ channels | Inward Ca²⁺ | Accelerates depolarization |
| Phase 4 (throughout) | I_K decay | K⁺ channels closing | Decreasing outward K⁺ | Removes repolarizing brake |
| Phase 0 | I_Ca-L | L-type Ca²⁺ channels | Inward Ca²⁺ | Upstroke (action potential) |
| Phase 3 | I_K | K⁺ channels (I_K) | Outward K⁺ | Repolarization |
5. Why SA Node Cannot Stay Depolarized - The Self-Resetting Mechanism
"Leakiness of Sinus Nodal Fibers to Sodium and Calcium Causes Self-Excitation" - Guyton and Hall
The SA node membrane is naturally leaky to Na⁺ and Ca²⁺, which would keep it permanently depolarized were it not for a self-resetting mechanism:
- During the action potential → L-type Ca²⁺ channels inactivate + K⁺ channels open widely
- Net outward K⁺ current → repolarization → brief hyperpolarization
- Hyperpolarization → K⁺ channels progressively close
- I_f activates (switched on by hyperpolarization) → slow inward Na⁺/Ca²⁺ overcomes declining outward K⁺
- Membrane drifts back to threshold → next action potential
6. Hierarchical Pacemakers and Intrinsic Rates
| Location | Intrinsic Firing Rate |
|---|---|
| SA node (dominant) | 70-80 beats/min |
| AV node | 40-60 beats/min |
| Bundle of His | 40 beats/min |
| Purkinje fibers | 15-20 beats/min |
The fastest pacemaker drives the heart (SA node normally). Slower latent pacemakers are suppressed by "overdrive suppression." If the SA node fails, the next fastest takes over as an ectopic pacemaker (escape rhythm).
7. Autonomic Modulation of Heart Rate
Both divisions of the ANS alter heart rate by changing the slope and/or threshold of phase 4:
| ANS | Mediator | Effect on Phase 4 | Heart Rate |
|---|---|---|---|
| Sympathetic | Norepinephrine / Epinephrine (β₁) | Steepens phase 4 slope (↑ I_f via cAMP); shifts threshold to more negative | ↑ (Tachycardia) |
| Parasympathetic | Acetylcholine (M₂) | Decreases slope of phase 4; makes MDP more negative (↑ K⁺ conductance) | ↓ (Bradycardia) |
Sympathetic stimulation also increases cAMP, which directly enhances HCN channel activity (I_f), explaining why ivabradine (a pure I_f blocker) selectively reduces heart rate without affecting contractility.
- Guyton and Hall Textbook of Medical Physiology
- Costanzo Physiology, 7th Edition
- Ganong's Review of Medical Physiology, 26th Edition
- Harrison's Principles of Internal Medicine, 22nd Edition
Anatomy of Scalp
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, richly illustrated content from multiple authoritative sources. Here is the complete answer:
Anatomy of the Scalp
Extent
The scalp covers the vault (calvaria) of the skull. It extends:
- Anteriorly: from the supraorbital margins (top of forehead)
- Posteriorly: to the superior nuchal line
- Laterally: down to the zygomatic arch and external acoustic meatus on each side
Layers - Mnemonic: SCALP
The five layers are remembered by the mnemonic SCALP, going from superficial to deep:
| Letter | Layer |
|---|---|
| S | Skin |
| C | Connective tissue (dense subcutaneous) |
| A | Aponeurosis (epicranial aponeurosis / galea aponeurotica) + occipitofrontalis muscle |
| L | Loose areolar connective tissue |
| P | Pericranium (periosteum of calvaria) |
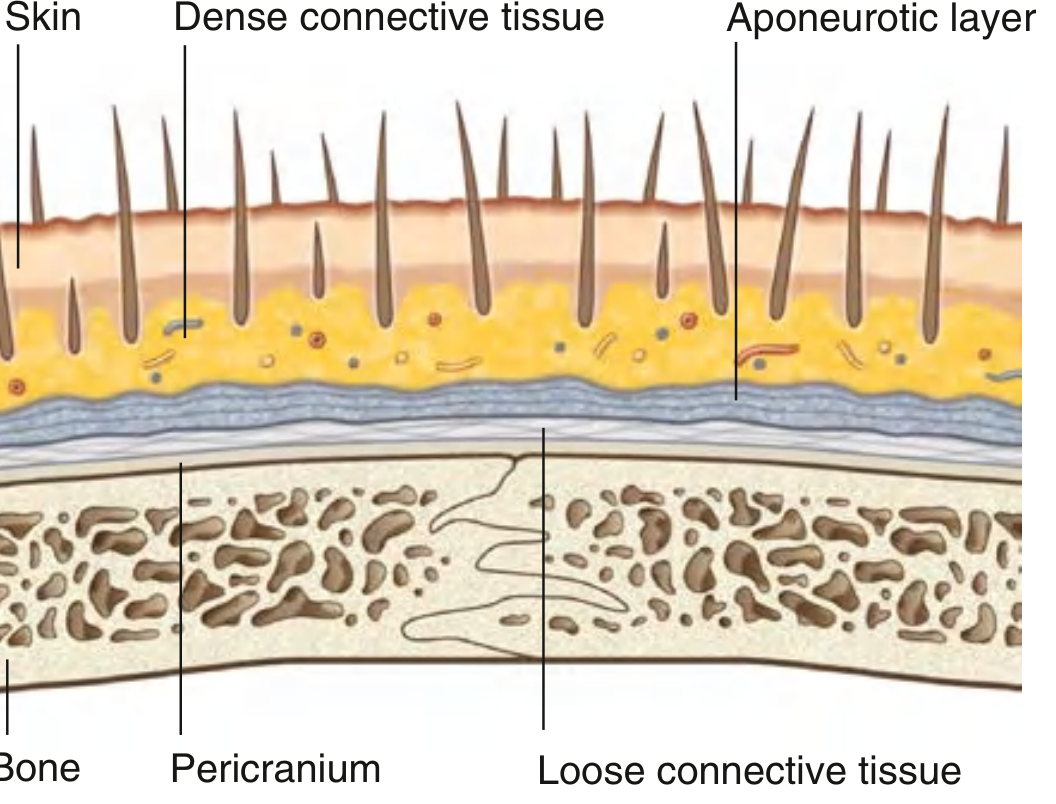
Figure: Layers of the Scalp. - Gray's Anatomy for Students
Layer 1 - Skin (S)
- Thickest skin in the body
- Bears hair follicles, sebaceous glands, and sweat glands
- Contains a rich capillary network
- Structurally like skin elsewhere on the body, except hair covers a large portion of it
Layer 2 - Connective Tissue, dense (C)
- Dense, fibrous subcutaneous layer that firmly anchors the skin to the underlying aponeurosis
- Contains the arteries, veins, and sensory nerves supplying the scalp
- The dense fibrous septa around vessels hold cut vessels open when the scalp is lacerated - this is why scalp wounds bleed profusely (vessels cannot retract and constrict)
- Forms the vascular "skeleton" of the scalp
Layers 1+2+3 are tightly bound together as the "scalp proper" - this is the unit torn away in serious "scalping" injuries.
Layer 3 - Aponeurosis / Epicranial Aponeurosis (Galea Aponeurotica) (A)
This layer is the epicranial aponeurosis (galea aponeurotica) plus the occipitofrontalis muscle (epicranius):
Occipitofrontalis muscle has two parts:
- Frontalis (frontal belly): attaches anteriorly to the skin of the eyebrows; passes upward across the forehead to the aponeurosis. Raises the eyebrows and wrinkles the forehead.
- Occipitalis (occipital belly): arises from the lateral part of the superior nuchal line and the mastoid process of the temporal bone; passes superiorly to join the aponeurosis posteriorly.
Epicranial aponeurosis (galea aponeurotica):
- A flat, tendinous sheet that connects the two bellies
- Covers the top of the skull like a helmet
- All three structures of the aponeurotic layer are anchored together by the dense connective tissue
Innervation of occipitofrontalis:
- Frontal belly: temporal branches of facial nerve (CN VII)
- Occipital belly: posterior auricular branch of facial nerve (CN VII)
Function: The occipitofrontalis muscle moves the entire scalp proper over the calvaria (made possible by the loose layer 4 beneath).
Layer 4 - Loose Areolar Connective Tissue (L)
- A thin, spongy layer that acts as a gliding plane between the scalp proper (layers 1-3) and the pericranium
- Allows free movement of the scalp
- Contains emissary veins - valveless communications between the scalp veins and the intracranial venous sinuses
Critical clinical importance:
- "Danger zone of scalp" - infections spreading into this layer can travel freely in all directions across the entire scalp
- Infections can track through emissary veins directly into the cranial venous sinuses (e.g., superior sagittal sinus) → intracranial sepsis (meningitis, cavernous sinus thrombosis)
- Blood or pus collects here (subgaleal hematoma/abscess) - spreads widely but is limited at the orbital margins anteriorly, zygomatic arches laterally, and superior nuchal lines posteriorly
Layer 5 - Pericranium (P)
- The periosteum on the outer surface of the calvaria
- Firmly attached to the skull bones but removable (unlike dura mater)
- Cannot cross the suture lines (since periosteum attaches into the sutures)
- A cephalohematoma (in newborns) - blood collects between pericranium and skull bone - is therefore limited by the suture lines (distinguishing it from a caput succedaneum which crosses sutures)
Blood Supply
The scalp has one of the richest blood supplies in the body. It receives contributions from both the internal and external carotid arteries.
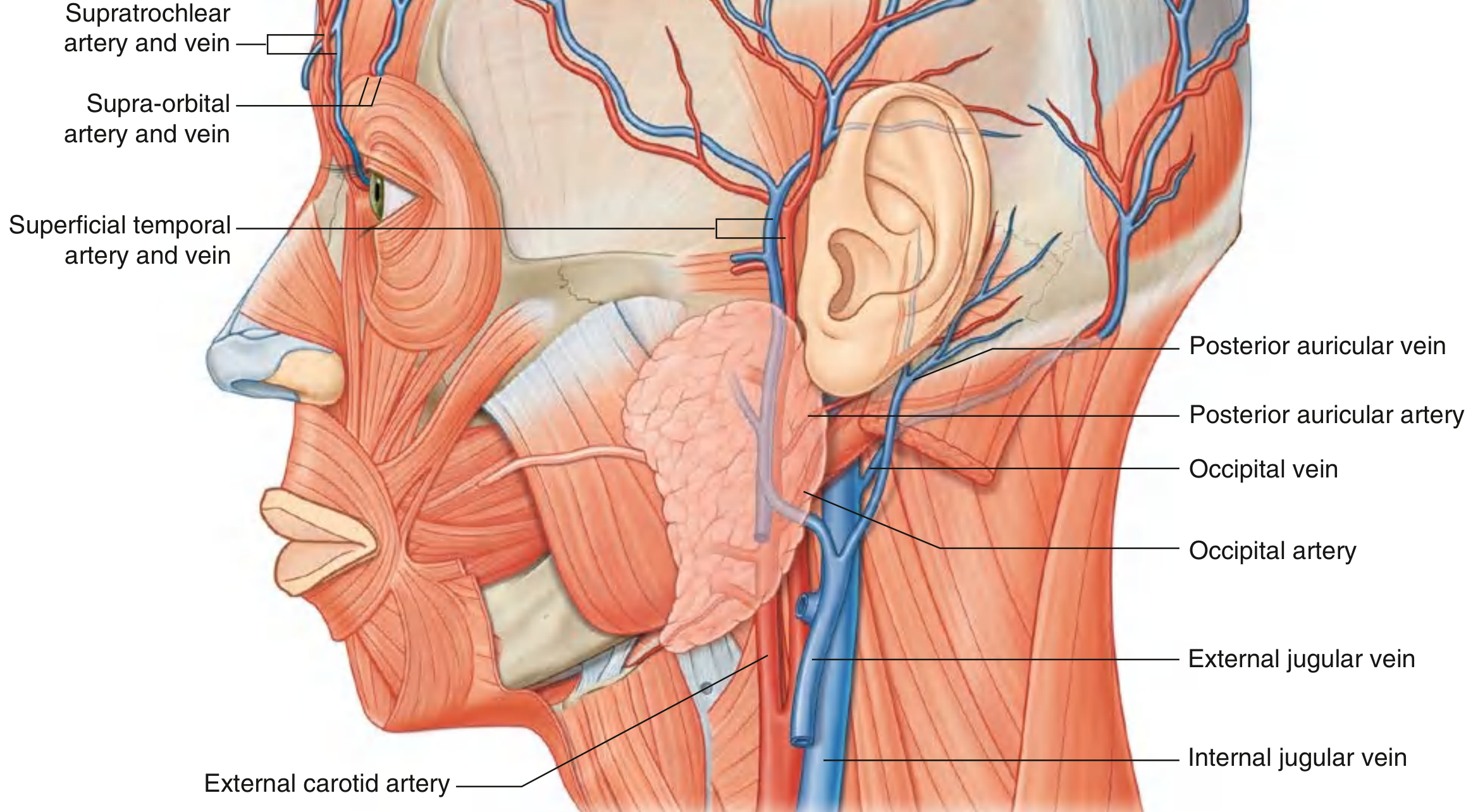
Figure: Vasculature of the Scalp. - Gray's Anatomy for Students
Arteries
From the Ophthalmic Artery (branch of Internal Carotid Artery):
| Artery | Territory |
|---|---|
| Supratrochlear | Anterior scalp - medial forehead to vertex |
| Supra-orbital | Anterior and superior scalp - lateral forehead to vertex |
From the External Carotid Artery:
| Artery | Territory |
|---|---|
| Superficial temporal (terminal branch of ECA) | Almost the entire lateral scalp; divides into anterior and posterior branches anterior to the ear |
| Posterior auricular | Small area posterior to the ear |
| Occipital | Large part of posterior scalp |
All these arteries anastomose freely with each other - this is why scalp flaps survive even when based on a single pedicle, and also why isolated ligation of one vessel rarely controls scalp bleeding.
Veins
Veins follow the arteries closely:
- Supratrochlear and supra-orbital veins → angular vein → facial vein
- Superficial temporal vein → retromandibular vein
- Posterior auricular vein → tributary of retromandibular vein
- Occipital vein → suboccipital venous plexus → vertebral veins
Additionally, emissary veins in layer 4 communicate directly with:
- Superior sagittal sinus (via parietal emissary veins)
- Cavernous sinus (via ophthalmic veins)
- Transverse sinus (via mastoid emissary veins)
Nerve Supply (Sensory Innervation)
The dividing line runs from posterior to the ear, up to the vertex, then to the opposite posterior ear.

Figure: Innervation of the Scalp. - Gray's Anatomy for Students
Anterior to the Ears and Vertex - Trigeminal Nerve (CN V)
| Nerve | Division | Territory |
|---|---|---|
| Supratrochlear | V1 (ophthalmic) | Medial forehead near midline |
| Supra-orbital | V1 (ophthalmic) | Lateral forehead to vertex |
| Zygomaticotemporal | V2 (maxillary) | Small anterior temple area |
| Auriculotemporal | V3 (mandibular) | Temporal region, anterior to ear, to vertex |
Posterior to the Ears and Vertex - Cervical Spinal Nerves (C2-C3)
| Nerve | Root | Territory |
|---|---|---|
| Greater occipital nerve | Posterior ramus C2 | Large part of posterior scalp to vertex (most important) |
| Lesser occipital nerve | Anterior ramus C2 | Posterior and superior to the ear |
| Great auricular nerve | Anterior rami C2, C3 | Small area just posterior to the ear |
| Third occipital nerve | Posterior ramus C3 | Lower posterior scalp |
Lymphatic Drainage
Lymphatics follow the arterial pattern:
| Region | Drains to |
|---|---|
| Occipital | Occipital nodes (at trapezius attachment) → deep cervical nodes |
| Posterior to ear | Mastoid (retroauricular) nodes → deep cervical nodes |
| Temporal | Superficial parotid (pre-auricular) nodes → deep cervical nodes |
| Frontal/parietal | Submandibular nodes → deep cervical nodes |
All eventually drain into the deep cervical lymph nodes.
Clinical Significance Summary
| Clinical Point | Layer Involved | Mechanism |
|---|---|---|
| Profuse scalp bleeding | Layer 2 (dense CT) | Vessels held open by fibrous tissue; cannot retract |
| Danger zone / spread of infection | Layer 4 (loose CT) | Loose tissue allows free spread; emissary veins carry infection intracranially |
| Cephalohematoma (confined to one bone) | Between pericranium and skull | Pericranium attached to sutures - blood cannot cross suture lines |
| Caput succedaneum (crosses suture lines) | Layer 4 (subgaleal/subcutaneous) | Above pericranium, not restricted by sutures |
| Scalp flap viability | Layer 2 (vascular layer) | Rich anastomotic supply allows large flaps to survive |
| Scalp "proper" (avulsed in scalping) | Layers 1-3 | Tightly bound; split at loose layer 4 |
- Gray's Anatomy for Students
- PC Dikshit's Textbook of Forensic Medicine and Toxicology
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.