G protinex couple receptor expline this topic
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed for a thorough explanation. Let me compile the complete answer.
G Protein-Coupled Receptors (GPCRs)
GPCRs are the largest and most diverse family of cell surface receptors in the human body. They are also called heptahelical receptors or serpentine receptors because they contain seven membrane-spanning alpha-helices. Hundreds of hormones, neurotransmitters, and sensory signals (light, smell, taste) work through these receptors.
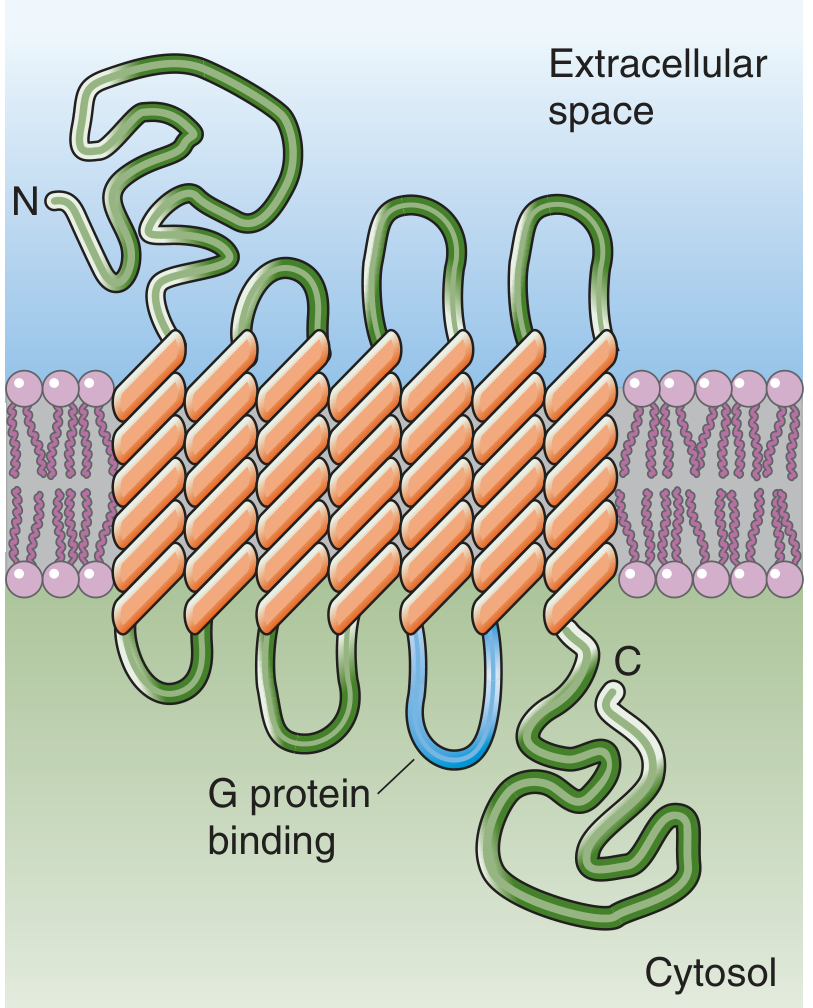
1. Structure of GPCRs
| Feature | Detail |
|---|---|
| Transmembrane domains | 7 alpha-helices spanning the lipid bilayer |
| N-terminus | Extracellular - contains the ligand-binding region |
| C-terminus | Intracellular |
| G protein binding site | 3rd intracellular loop (highlighted blue in the diagram above) |
| No intrinsic kinase activity | Signal is transduced via G proteins |
The extracellular binding domain of each receptor is specific for one primary ligand (polypeptide hormone, catecholamine, chemokine, or neurotransmitter), though some receptors respond to multiple related signals.
2. The Heterotrimeric G Protein
GPCRs work by coupling to heterotrimeric G proteins on the intracellular membrane surface. These are composed of three subunits:
| Subunit | Size | Function |
|---|---|---|
| Ga (alpha) | 42-50 kDa | Binds and hydrolyzes GTP; interacts with downstream effectors (e.g., adenylyl cyclase) |
| Gb (beta) | 33-35 kDa | Part of the βγ complex; anchors the trimer to the membrane |
| Gg (gamma) | 8-10 kDa | Anchors via lipid modification; βγ complex also signals independently |
There are at least 16 different Gα subunits, 5 Gβ subunits, and 11 Gγ subunits in mammalian tissue, enabling great diversity of signaling.
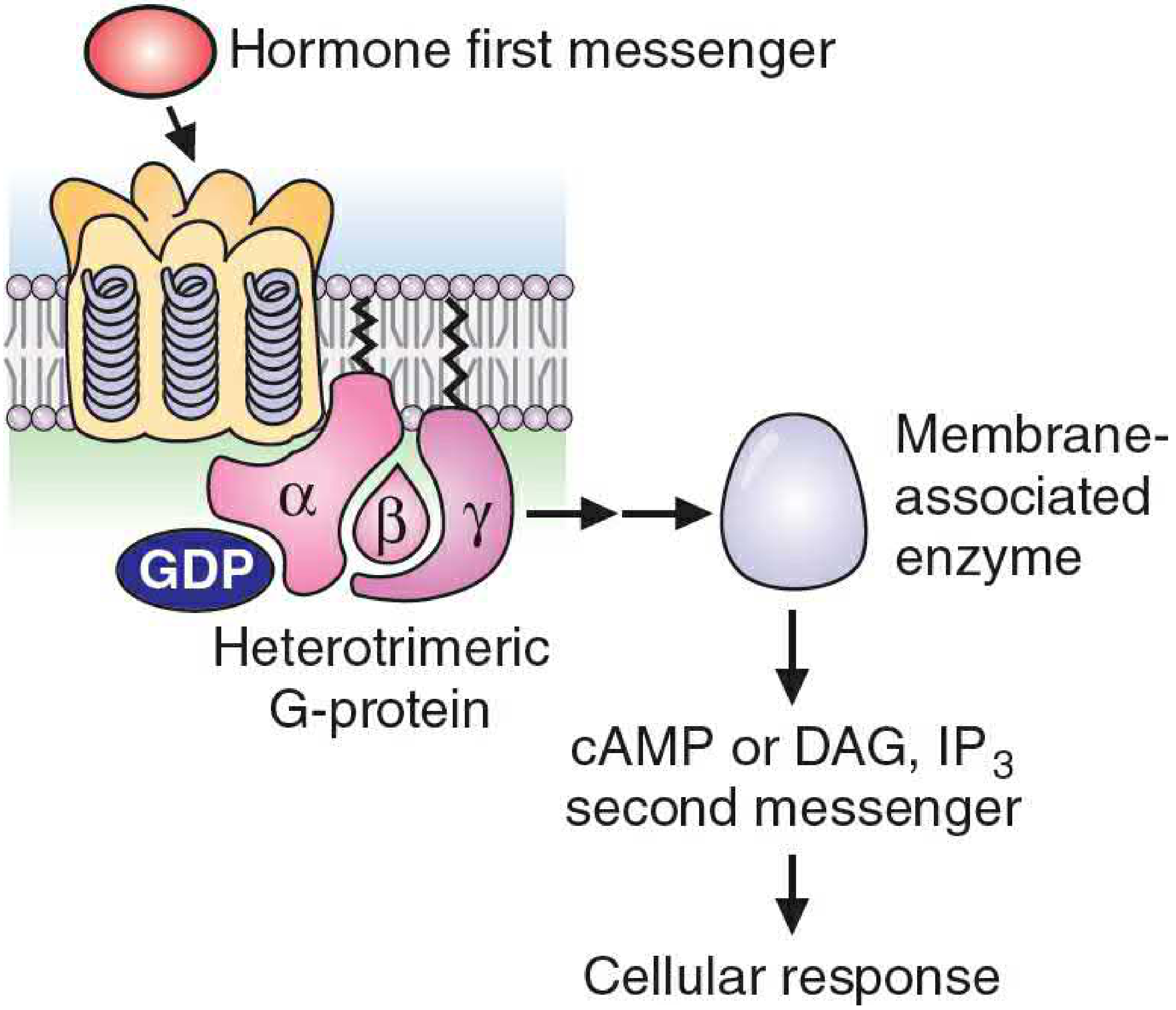
3. The G Protein Activation Cycle (Step by Step)
Step 1 - Resting state:
The Gα subunit holds GDP and remains associated with Gβγ, either free in the membrane or loosely bound to the unoccupied receptor.
Step 2 - Ligand binds:
When a hormone/neurotransmitter binds the GPCR, it causes a conformational change that promotes GDP dissociation and GTP binding on the α subunit. This causes the α subunit to dissociate from both the receptor and the βγ complex.
Step 3 - Effector activation:
- The GTP-Gα subunit binds and activates/inhibits its target enzyme (e.g., adenylyl cyclase) → generates second messengers.
- The free βγ complex simultaneously targets other proteins (e.g., K+ channels, phospholipase C, adenylyl cyclase isoforms).
Step 4 - Self-inactivation:
Over time, the Gα subunit hydrolyzes GTP to GDP via its intrinsic GTPase activity. This causes the α subunit to dissociate from its effector, terminating the signal. (GTPase-activating proteins [GAPs] can accelerate this hydrolysis.)
Step 5 - Reassembly:
The GDP-bound Gα reassociates with Gβγ and the receptor, restoring the resting state.
This built-in GTPase "internal inactivation signal" means that sustained elevation of a second messenger requires continued presence of the hormone. - Basic Medical Biochemistry, p. 339
4. Major G Protein Classes and Their Pathways
| G Protein Type | Gα Subunit | Effect on Effector | Second Messenger | Examples of Receptors |
|---|---|---|---|---|
| Gs | Gαs | Stimulates adenylyl cyclase | ↑ cAMP | β1, β2-adrenergic; glucagon-R; H2 histamine |
| Gi | Gαi | Inhibits adenylyl cyclase | ↓ cAMP | α2-adrenergic; M2 muscarinic; opioid |
| Gq | Gαq | Activates phospholipase Cβ | ↑ IP3 + DAG | α1-adrenergic; M1, M3 muscarinic; H1 histamine |
| G12/13 | Gα12/13 | Activates Rho GTPase | No classic second messenger | Thrombin receptor |
5. Second Messenger Pathways in Detail
A. The cAMP Pathway (Gs)
- Gαs activates adenylyl cyclase → converts ATP to cyclic AMP (cAMP)
- cAMP activates Protein Kinase A (PKA)
- PKA phosphorylates serine/threonine residues on target proteins (enzymes, transcription factors, ion channels)
- Net effects: glycogen breakdown, lipolysis, smooth muscle relaxation, cardiac stimulation, gene expression changes
- Signal terminated by phosphodiesterase (cleaves cAMP to AMP)
B. The IP3/DAG Pathway (Gq)
- Gαq activates Phospholipase Cβ (PLCβ)
- PLCβ cleaves PIP2 (phosphatidylinositol-4,5-bisphosphate) into two second messengers:
- IP3 (inositol trisphosphate) → cytosolic; binds ER receptor → releases Ca²+ from intracellular stores
- DAG (diacylglycerol) → membrane-associated; activates Protein Kinase C (PKC)
- PKC phosphorylates various target proteins
- Ca²+ acts as a third messenger, activating calmodulin-dependent kinases
C. The βγ Complex Pathway
The Gβγ complex is not just a passive anchor - it independently signals:
- Opens GIRK channels (G protein-coupled inwardly rectifying K+ channels) in the heart (via M2 muscarinic receptors) → slows heart rate
- Modulates adenylyl cyclase (stimulates some isoforms, inhibits others)
- Activates phospholipase A2 and phospholipase C isoforms
- Recruits βARK (β-adrenergic receptor kinase) to the membrane → leads to receptor desensitization
6. Receptor Desensitization (Signal Termination at the Receptor Level)
Prolonged GPCR activation triggers several shutdown mechanisms:
- Phosphorylation by GRKs (G protein-coupled receptor kinases, including βARK): phosphorylates the ligand-bound receptor
- β-arrestin binding: phosphorylated receptor recruits β-arrestin, which uncouples the receptor from G proteins
- Endocytosis: the receptor-ligand-arrestin complex is internalized via clathrin-coated pits → reduces surface receptor number (downregulation)
- Receptor recycling or degradation: receptors may be resensitized and returned to the membrane, or degraded
- PKA feedback: cAMP-activated PKA can also phosphorylate Gα-coupled receptors, switching their G protein preference (e.g., β2 receptor shifts from Gs to Gq) - Basic Medical Biochemistry, p. 337, Katzung Pharmacology, p. 1706
7. Examples of Clinically Important GPCRs
| Receptor | Ligand | G Protein | Effect |
|---|---|---|---|
| β1-adrenergic | Epinephrine/Norepinephrine | Gs | ↑ HR and contractility (heart) |
| β2-adrenergic | Epinephrine | Gs | Bronchodilation (lungs) |
| α1-adrenergic | Norepinephrine | Gq | Vasoconstriction |
| α2-adrenergic | Norepinephrine | Gi | ↓ NE release (presynaptic); ↓ cAMP |
| M1 muscarinic | Acetylcholine | Gq | ↑ secretions, CNS excitation |
| M2 muscarinic | Acetylcholine | Gi (+ βγ → GIRK) | ↓ HR (vagal slowing) |
| M3 muscarinic | Acetylcholine | Gq | Smooth muscle contraction, gland secretion |
| Glucagon receptor | Glucagon | Gs | ↑ glycogenolysis, gluconeogenesis |
| Rhodopsin | Light (retinal) | Gt (transducin) | Vision phototransduction |
| Olfactory receptors | Odorants | Golf (Gs-like) | Smell perception |
8. Clinical Significance and Pharmacological Targets
GPCRs are the most common drug targets in medicine (~34% of all approved drugs act on GPCRs):
- Beta-blockers (propranolol, metoprolol): antagonize β-adrenergic GPCRs → used in hypertension, heart failure, angina
- Beta-agonists (salbutamol): activate β2 GPCRs → bronchodilation in asthma
- Opioids (morphine): activate Gi-coupled opioid receptors → analgesia
- Antipsychotics (haloperidol): block D2 dopamine GPCRs
- Atropine: blocks muscarinic GPCRs → raises heart rate
- Cholera toxin: locks Gαs in the GTP-bound active state → constant cAMP production → massive secretory diarrhea
- Pertussis toxin: inactivates Gαi → blocks inhibitory signaling
Sources: Basic Medical Biochemistry - A Clinical Approach 6e, pp. 337-343 | Medical Physiology (Boron & Boulpaep), pp. 79-82 | Neuroscience: Exploring the Brain 5e, Chapter 6 | Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.