Hodgkin lymphoma diagnosis investigation their findings and treatment and when to start
Reading File
Finding Sources
Searching PubMed
"Hodgkin lymphoma" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
Hodgkin Lymphoma: Diagnosis, Investigation, Findings & Treatment
Overview
Hodgkin lymphoma (HL) is a neoplasm of germinal center B cells, distinguished by the presence of Reed-Sternberg (RS) cells set within a reactive inflammatory background. It has a peak incidence in the third decade of life (ages 15–40) and carries an excellent overall prognosis (OS ~86.4%).
Classification
HL is divided into two main groups:
| Type | Frequency | Key Features |
|---|---|---|
| Classic HL (CHL) | 95% | 4 subtypes; RS cells express CD15, CD30 |
| Nodular Lymphocyte-Predominant HL (NLPHL) | 5% | "Popcorn" (LP) cells; CD20+, CD45+, CD15−; indolent course |
Classic HL Subtypes
| Subtype | Frequency | Notes |
|---|---|---|
| Nodular Sclerosis (NS) | 75% | Most common; equal M:F; collagen bands; anterior mediastinal mass; adolescents/young adults |
| Mixed Cellularity (MC) | 15–20% | More common in HIV+ and developing countries; classic RS cells; aggressive |
| Lymphocyte-Rich | 5% | Rare |
| Lymphocyte-Depleted (LD) | <5% | Most aggressive; advanced-stage disease |
Pathogenesis
- RS cells derive from germinal center B cells (confirmed by identical immunoglobulin gene rearrangements in microdissected RS cells).
- EBV is present in RS cells in up to 70% of mixed-cellularity cases; EBV integration precedes clonal expansion.
- RS cells secrete cytokines (IL-5, TGF-β, IL-13) driving the reactive inflammatory infiltrate.
- RS cells evade immunity by overexpressing PD-L1/PD-L2 (chromosome 9p amplification) and losing MHC class I expression — the basis for anti-PD-1 immunotherapy efficacy.
Clinical Presentation & Symptoms
- Asymptomatic peripheral adenopathy is the most common presentation — typically cervical or supraclavicular lymphadenopathy.
- B symptoms (in ~25% of patients):
- Fever >38°C (persistent)
- Drenching night sweats
- Unexplained weight loss >10% body weight over 6 months
- Pruritus — severe, generalized; often precedes diagnosis by months (rare in NHL).
- Mediastinal mass — especially in NS subtype (may cause SVC syndrome, cough, dyspnea).
- HL spreads in a contiguous, stepwise pattern through anatomically adjacent nodal groups (unlike NHL which spreads non-contiguously).
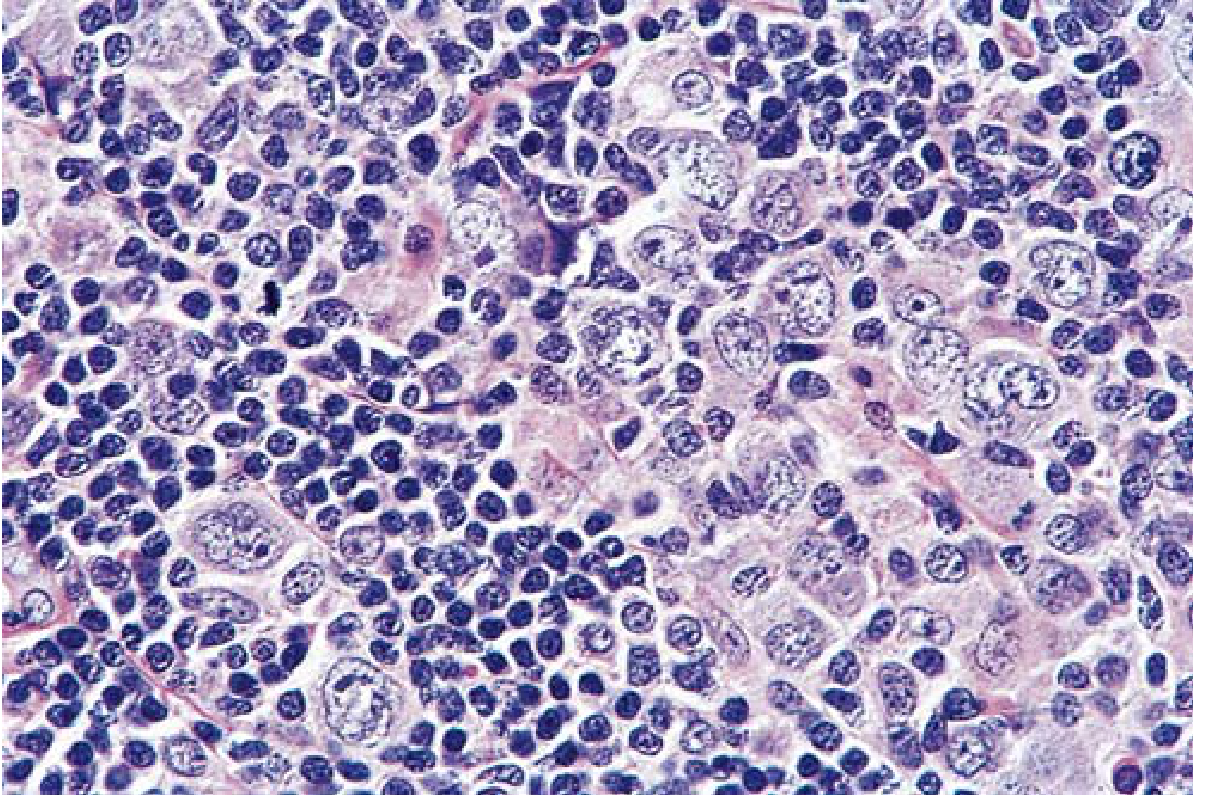
Diagnosis: The Reed-Sternberg Cell
The RS cell is the sine qua non of Hodgkin lymphoma.
Morphology:
- Large cell (15–45 μm diameter)
- Enormous multilobed nucleus
- Exceptionally prominent nucleoli
- "Owl-eye" appearance — two mirror-image nuclei each with a large acidophilic nucleolus surrounded by a clear halo
Immunophenotype (Classic HL):
- ✅ CD15+, CD30+
- ❌ CD45− (leukocyte common antigen negative)
- ❌ B-cell and T-cell markers negative
NLPHL variant:
- "Popcorn" (LP) cells — CD20+, CD45+, CD15−, variably CD30+
Flow cytometry is often non-diagnostic in HL — tissue biopsy is mandatory.
Histology — Mixed-Cellularity HL
Investigation & Workup
1. Tissue Diagnosis
- Excisional lymph node biopsy — required; provides tissue for histology, IHC, and molecular studies.
- IHC panel: CD15, CD30, CD45, CD20, CD3, PAX5.
2. Laboratory Studies
- Full blood count, ESR, LDH, β2-microglobulin, albumin, liver/renal function.
- HIV serology.
3. Imaging — Staging Investigations
- 18F-FDG PET/CT — investigation of choice for staging (sensitivity 97%, specificity 100% for HL). Changes management in ~30% of HL cases vs CT alone. Provides baseline for treatment response monitoring.
- CT chest/abdomen/pelvis — acceptable if PET/CT unavailable.
- CT neck — optional; may assist in radiotherapy planning.
- Chest X-ray — not required for staging.
4. Bone Marrow Biopsy
- No longer required for routine staging if PET/CT has been performed.
5. Additional
- Whole-body MRI — only if PET/CT and CT are both unavailable.
- Echocardiography and pulmonary function tests — baseline before anthracycline/bleomycin therapy.
- Fertility counselling and sperm/egg banking before chemotherapy.
Staging — Ann Arbor System with Cotswolds Modification
| Stage | Definition |
|---|---|
| I | Single lymph node region or lymphoid structure |
| II | ≥2 lymph node regions on the same side of the diaphragm |
| III | Lymph node regions on both sides of the diaphragm (III₁ = splenic/portal nodes; III₂ = para-aortic/iliac/mesenteric) |
| IV | Multiple extranodal sites or nodes + extranodal disease |
Suffix modifiers:
- A — No B symptoms
- B — B symptoms present
- E — Contiguous extranodal involvement
- X — Bulky disease (MMR >0.33 on CXR or >0.35 on CT; or nodal mass >10 cm)
Treatment — When to Start & What to Use
Treatment is started as soon as staging is complete and pathological diagnosis is confirmed. The approach is entirely stage-guided.
Favorable Early-Stage (Stage I–II, No Bulky Disease, No B Symptoms)
- Combined modality: 2–4 cycles ABVD + involved-field/involved-site radiotherapy (ISRT 20–30 Gy)
- If PET-negative after 2 cycles → can omit radiotherapy in selected patients (to reduce long-term toxicity)
- Durable remission rate: 90–95%
Unfavorable Early-Stage (Stage I–II with Bulky Disease or B Symptoms)
- 4–6 cycles ABVD + consolidation radiotherapy
- Durable remission: ~80%
Advanced Stage (Stage III–IV)
- 6–8 cycles ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) — the backbone regimen
- Alternative: BEACOPPescalated (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone) — higher CR rate but greater toxicity; used in high-risk/young fit patients
- PET-adapted therapy — interim PET (after cycle 2) guides de-escalation (switch to ABVD if PET-negative) or escalation
- Durable remission: ~70%
ABVD Regimen
| Drug | Mechanism |
|---|---|
| A – Doxorubicin | Anthracycline (topoisomerase II inhibitor) |
| B – Bleomycin | DNA strand cleavage |
| V – Vinblastine | Vinca alkaloid (microtubule inhibitor) |
| D – Dacarbazine | Alkylating agent |
Relapsed/Refractory Disease
- Salvage chemotherapy (DHAP, ICE, GDP) → high-dose chemotherapy + autologous stem cell transplant (ASCT)
- Brentuximab vedotin (anti-CD30 antibody-drug conjugate) — effective in relapsed/refractory CHL
- Checkpoint inhibitors — nivolumab (anti-PD-1) and pembrolizumab — highly active even in multiply relapsed HL; most tumors respond even after resistance to other therapies (due to PD-L1 amplification on RS cells)
Prognosis Summary
| Disease Stage | 5-Year OS |
|---|---|
| Localized (Stage I–II) | ~92% |
| Advanced (Stage III–IV) | ~70–80% |
| Overall | ~86% |
Long-term follow-up is essential to detect late effects: secondary malignancies (particularly breast cancer with mediastinal RT), cardiac toxicity (anthracyclines), pulmonary fibrosis (bleomycin), and infertility.
Sources:
- Robbins & Kumar Basic Pathology, pp. 417–421
- Cummings Otolaryngology Head and Neck Surgery, pp. 2246–2248
- Grainger & Allison's Diagnostic Radiology, Ch. 64
This is a shared conversation. Sign in to Orris to start your own chat.