general lines of management of a case of acute poisoning
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
I now have comprehensive information from Goldman-Cecil Medicine, the management algorithm image, and supplementary antidote content. Let me compile the complete answer.
General Lines of Management of Acute Poisoning
The management of acute poisoning follows a structured, stepwise approach regardless of the specific toxin. The framework below is based on Goldman-Cecil Medicine (Chapter 96 — Nelson & Calello).
1. Initial Assessment & Diagnosis
History — gather:
- Toxicant(s) involved (name, estimated amount, formulation)
- Time and route of exposure (ingestion, inhalation, dermal, injection)
- Symptoms onset and progression
- Treatment already given
- Available medications at home (patient's, family's)
- Occupational/avocational exposures
The history may be incomplete or inaccurate if the patient is confused or suicidal; corroborate with relatives, EMS, and scene findings.
Physical Examination — focus on:
- Vital signs (BP, HR, RR, temperature, GCS)
- Eyes (pupils: miosis = opioid/cholinergic; mydriasis = anticholinergic/adrenergic)
- Neurologic (level of consciousness, tone, reflexes, seizures)
- Cardiopulmonary (arrhythmia, bronchospasm, pulmonary edema)
- GI (bowel sounds, vomiting, abdominal pain)
- Skin (diaphoresis, flushing, color, burns)
Toxidromes — recognize characteristic clusters:
| Toxidrome | Features | Example Agents |
|---|---|---|
| Opioid | Miosis, coma, respiratory depression | Heroin, fentanyl, morphine |
| Anticholinergic | Mydriasis, dry flushed skin, tachycardia, urinary retention, delirium | Atropine, TCAs, antihistamines |
| Cholinomimetic | SLUDGE (salivation, lacrimation, urination, defecation, GI cramps, emesis) + bradycardia, miosis, bronchospasm | Organophosphates, carbamates |
| Adrenergic | Mydriasis, hypertension, tachycardia, hyperthermia, diaphoresis | Cocaine, amphetamines |
| Sedative-hypnotic | CNS depression, slurred speech, ataxia | Benzodiazepines, barbiturates |
Laboratory:
- Blood glucose (always), ABG/VBG, electrolytes, renal/hepatic function, CBC, coagulation
- Anion gap and osmol gap (screen for toxic alcohols)
- ECG (QRS widening → TCAs; QTc prolongation → many agents)
- Specific levels where indicated (paracetamol, salicylates, digoxin, ethanol, lithium, iron, carbamazepine)
- Urine toxicology screen (qualitative, limited specificity)
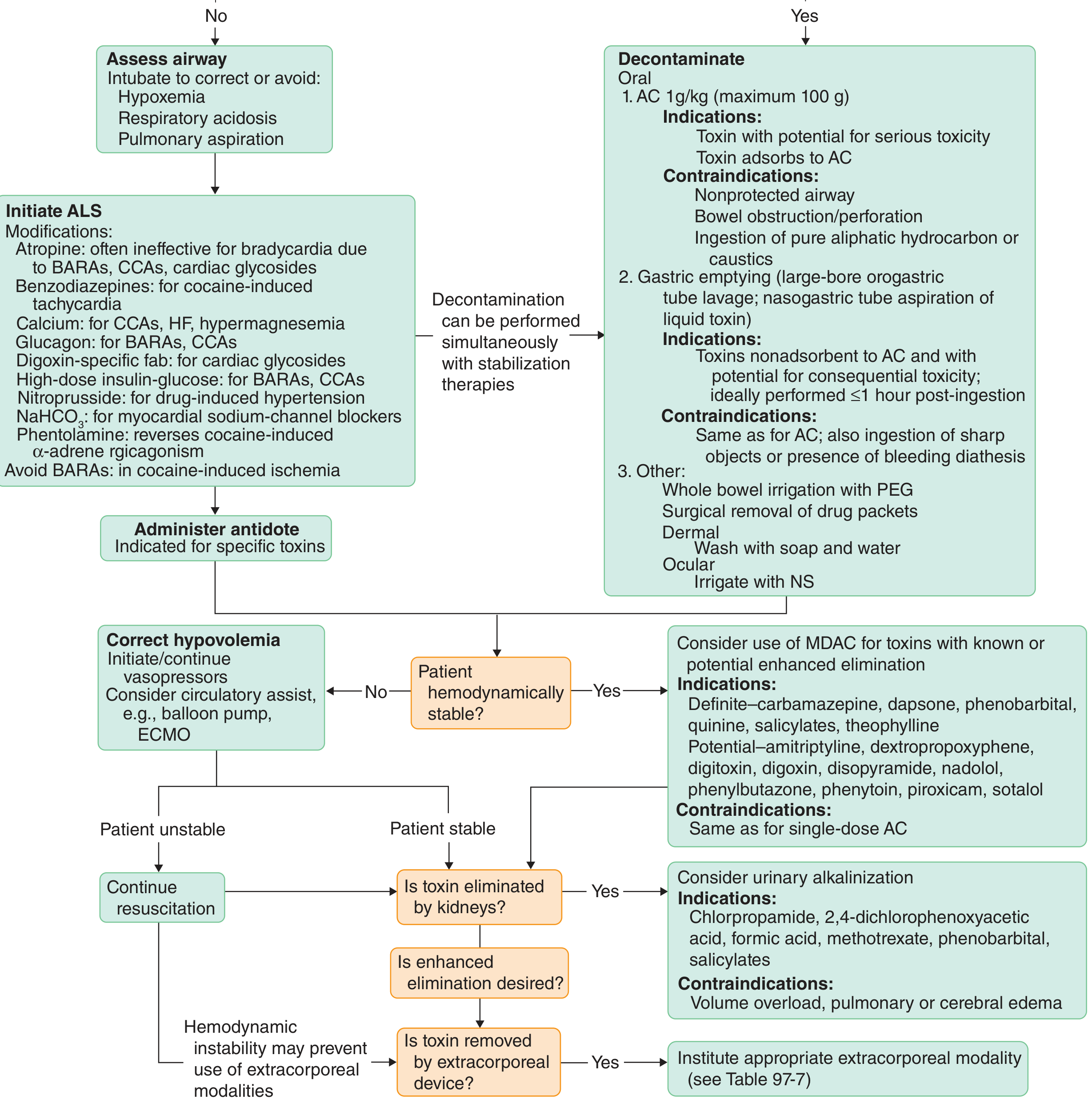
2. Stabilization (ABC + ALS)
Airway:
- Protect the airway; intubate if necessary to correct or prevent:
- Hypoxemia
- Respiratory acidosis
- Pulmonary aspiration
Breathing: Supplemental O₂; assisted ventilation as needed.
Circulation: IV access × 2; cardiac monitoring; correct hypotension with IV fluids; vasopressors if refractory.
ALS Modifications (toxin-specific):
- Atropine is often ineffective for bradycardia due to β-adrenergic receptor antagonists (BARAs), calcium-channel antagonists (CCAs), or cardiac glycosides
- Benzodiazepines for cocaine-induced tachycardia/agitation and seizures
- Calcium for CCAs, hydrofluoric acid, hypermagnesemia
- Glucagon for BARAs and CCAs
- Digoxin-specific Fab for cardiac glycoside toxicity
- High-dose insulin-glucose for BARAs and CCAs
- NaHCO₃ for myocardial sodium-channel blockers (TCAs, flecainide)
- Nitroprusside for drug-induced hypertension
- Phentolamine to reverse cocaine-induced α-adrenergic effects
- Avoid BARAs in cocaine-induced ischemia
Glucose — give IV dextrose for any altered consciousness with hypoglycaemia; precede with thiamine 100 mg IV if alcoholism suspected.
"Coma cocktail" (dextrose, thiamine, naloxone, flumazenil) — empirical use is rarely helpful and may be harmful in polydrug overdose; use only when there is strong suspicion of a specific agent.
3. Decontamination
Decontamination can be performed simultaneously with stabilization.
A. Oral (Gastrointestinal) Decontamination
1. Activated Charcoal (AC) — 1 g/kg body weight (max 100 g)
- Indications: Toxin with potential for serious toxicity that adsorbs to charcoal; ideally within 1 hour of ingestion (though benefit may extend to 2 hours for some agents)
- Contraindications: Unprotected airway; bowel obstruction or perforation; ingestion of pure aliphatic hydrocarbons or caustics; altered consciousness without secured airway
2. Gastric Emptying (Orogastric Lavage)
- Use large-bore orogastric tube; alternatively, nasogastric tube aspiration for liquid toxins
- Indications: Toxins non-adsorbent to AC with potential for consequential toxicity; ideally performed ≤1 hour post-ingestion
- Contraindications: Unprotected airway; ingestion of sharp objects; bleeding diathesis; same contraindications as AC; caustics
Ipecac-induced emesis is no longer recommended.
3. Whole Bowel Irrigation (WBI)
- Polyethylene glycol (PEG) solution at 500 mL/hour orally or via NGT, titrated to 2000 mL/hour, continued until rectal effluent clears
- Indications: Iron; sustained-release/enteric-coated medications; agents not adsorbed by AC; body packers (drug smugglers)
- Contraindications: Bowel perforation, obstruction, hemorrhage; hemodynamic or respiratory instability
B. Dermal Decontamination
- Remove contaminated clothing
- Wash thoroughly with soap and water
C. Ocular Decontamination
- Irrigate copiously with 0.9% normal saline
4. Antidotes
Few toxicants have specific antidotes. Their use does not replace the need for ongoing supportive care.
| Antidote | Indication |
|---|---|
| Naloxone | Opioid overdose (0.4–2 mg IV; repeat every 2–3 min; infusion at 0.8 mg/kg/hr) |
| Flumazenil | Benzodiazepine overdose (0.2 mg/min IV; max 1 mg) — caution in TCA co-ingestion/chronic BZD users |
| N-acetylcysteine (NAC) | Paracetamol (acetaminophen) overdose |
| Atropine + pralidoxime | Organophosphate/carbamate toxicity |
| Digoxin-specific Fab | Digoxin/cardiac glycoside toxicity |
| Physostigmine | Anticholinergic toxidrome (select cases) |
| Fomepizole | Methanol/ethylene glycol poisoning |
| Hydroxocobalamin | Cyanide poisoning |
| Calcium gluconate | Calcium-channel blocker / HF / hypermagnesemia |
| Glucagon | Beta-blocker / calcium-channel blocker |
| Edetate calcium disodium (CaNa₂EDTA) | Lead poisoning |
| Octreotide | Sulfonylurea-induced hypoglycaemia |
| Sodium bicarbonate | TCA / Na-channel blocker toxicity |
| Pyridoxine (B₆) | Isoniazid overdose |
| Methylene blue | Methaemoglobinaemia |
| Deferoxamine | Iron poisoning |
5. Enhanced Elimination
Used when the toxin is absorbed and elimination needs to be accelerated.
A. Multiple-Dose Activated Charcoal (MDAC)
- Average dose: 12.5 g every 4–6 hours (after initial 1 g/kg loading dose)
- Works via: interruption of enterohepatic/enteroenteric recirculation; "GI dialysis"
- Definite benefit: Carbamazepine, dapsone, phenobarbital, quinine, salicylates, theophylline
- Potential benefit: Amitriptyline, digitoxin, digoxin, phenytoin, sotalol, nadolol, piroxicam
- Contraindications: Same as single-dose AC
B. Urinary Alkalinization
- IV sodium bicarbonate to achieve urine pH 7.5–8.5
- Indications: Chlorpropamide, 2,4-dichlorophenoxyacetic acid, formic acid, methotrexate, phenobarbital, salicylates
- Contraindications: Volume overload, pulmonary oedema, cerebral oedema
C. Extracorporeal Removal
- Consider when patient is hemodynamically stable (instability may preclude use)
- Modalities: haemodialysis, haemoperfusion, haemofiltration, exchange transfusion, plasmapheresis
- Indications: Lithium, salicylates, methanol, ethylene glycol, theophylline, valproate (see specific extracorporeal criteria)
6. Disposition & Psychiatric Review
- All cases of intentional self-poisoning require psychiatric assessment before discharge
- Recurrent purposeful self-poisoning rate is 12–18%, with most events within 3 months
- Risk-stratify for ICU admission vs. monitored ward vs. discharge with follow-up
- Notify the Poison Control Centre where available — they provide real-time management guidance and collect data
Source: Goldman-Cecil Medicine, International Edition — Chapter 96: Acute Poisoning (Nelson LS, Calello DP), pp. 1111–1124.
This is a shared conversation. Sign in to Orris to start your own chat.