Hey
Hey! How can I help you today?
Can I teach me coronary circulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich content from multiple textbooks. Let me compile a thorough, well-illustrated lesson on coronary circulation.
Coronary Circulation
1. Overview
The coronary circulation is the blood supply system of the heart muscle itself. The heart cannot rely on the blood inside its chambers for nourishment - only the innermost 0.1 mm of the endocardium can absorb nutrients directly from luminal blood. All the rest of the myocardium depends entirely on the coronary arteries.
Coronary artery disease is responsible for about one-third of all deaths in industrialized countries, making this one of the most important topics in medicine.
- Guyton and Hall Textbook of Medical Physiology
2. Anatomy of the Coronary Arteries
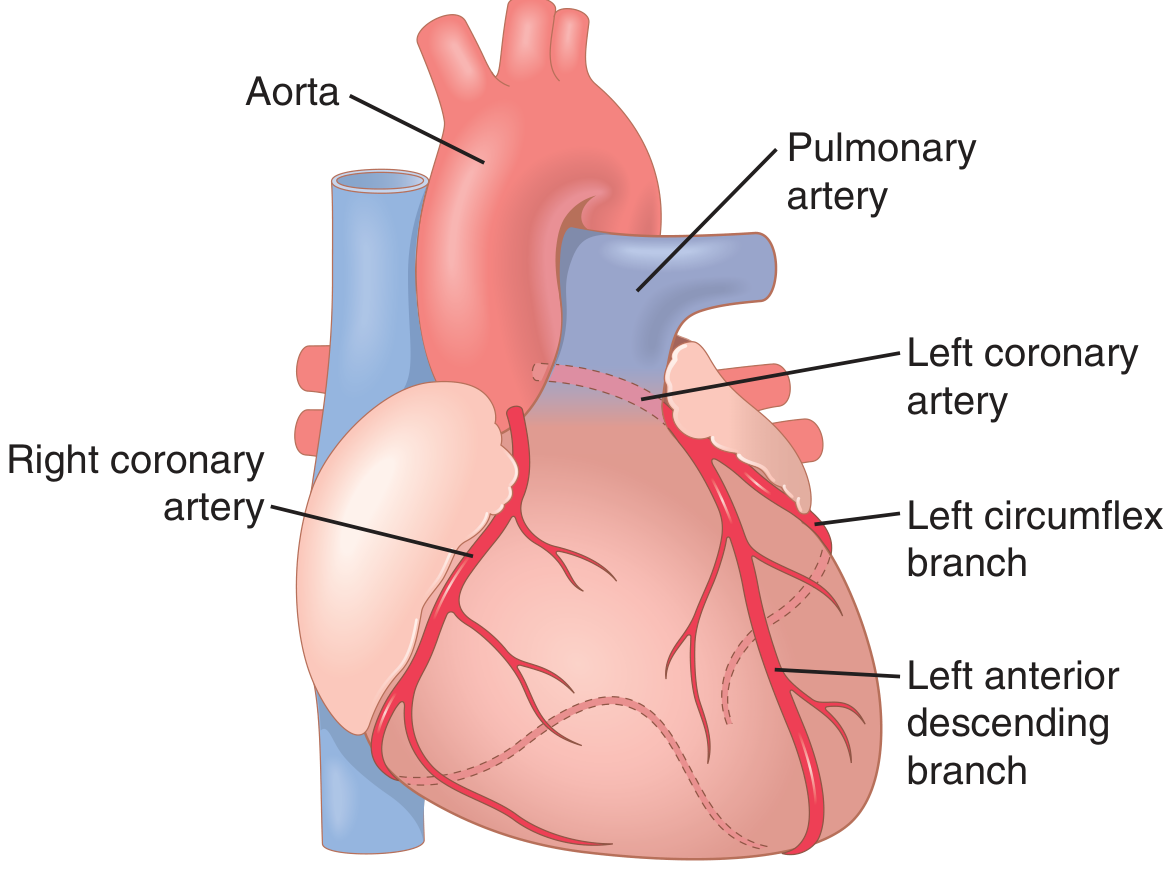
Coronary arteries - Guyton and Hall
The two main coronary arteries arise from the aortic sinuses (sinuses of Valsalva) at the root of the ascending aorta.
Right Coronary Artery (RCA)
- Originates from the right aortic sinus
- Runs anteriorly then descends in the coronary sulcus (atrioventricular groove) between right atrium and right ventricle
- Turns posteriorly toward the diaphragmatic surface of the heart
Key branches:
| Branch | Supplies |
|---|---|
| Sinoatrial nodal branch | SA node (the pacemaker) |
| Right marginal branch | Acute (inferior) margin of the heart toward apex |
| AV nodal branch | Atrioventricular node |
| Posterior interventricular branch (posterior descending artery, PDA) | Posterior interventricular septum |
The RCA supplies: right atrium, right ventricle, SA and AV nodes, interatrial septum, a portion of the left atrium, the posteroinferior one-third of the interventricular septum, and a portion of the posterior left ventricle.
In 80-90% of people, the RCA is dominant (gives off the PDA).
Left Coronary Artery (LCA)
- Originates from the left aortic sinus
- Passes between the pulmonary trunk and the left auricle, then divides into its two main branches
| Branch | Course | Supplies |
|---|---|---|
| Left Anterior Descending (LAD) | Descends in the anterior interventricular sulcus toward the apex | Anterior left ventricle, anterior 2/3 of interventricular septum, AV bundle and its branches |
| Left Circumflex (LCx) | Runs in the coronary sulcus to the base/diaphragmatic surface | Left atrium, lateral and posterior left ventricle |
| Left marginal artery (branch of LCx) | Across the obtuse margin of the heart | Lateral left ventricle |
The LCA overall supplies: most of the left atrium and left ventricle, the anterior 2/3 of the interventricular septum, and the AV bundle (His-Purkinje system).
- Gray's Anatomy for Students
3. Coronary Venous Drainage
Blood returns to the right side of the heart via three routes:
- Coronary sinus - receives ~75% of left ventricular venous flow; empties into the right atrium. Main tributaries: great, middle, and small cardiac veins.
- Anterior cardiac veins - drain most of right ventricular blood, empty directly into the right atrium (not via coronary sinus).
- Thebesian veins (venae cordis minimae) - tiny vessels that drain small amounts directly into all four cardiac chambers.
- Guyton and Hall Textbook of Medical Physiology
4. Coronary Blood Flow - Normal Values
- At rest: ~70 mL/min per 100 g of heart weight, or approximately 225 mL/min total
- This represents about 4-5% of total cardiac output
- During strenuous exercise, coronary flow increases 3-4 fold to meet the 6-9 fold increase in cardiac work
5. Phasic Nature of Coronary Flow (Systole vs. Diastole)
This is a unique and clinically important feature:
- During systole: The contracting left ventricular muscle compresses the intramyocardial coronary vessels. Blood flow in the left coronary artery drops sharply - even briefly reverses.
- During diastole: Myocardium relaxes, compression is relieved, and the majority of left coronary filling occurs.
Clinical pearl: This is why tachycardia is dangerous in coronary artery disease - a fast heart rate shortens diastole disproportionately, reducing the window for left coronary perfusion.
The right ventricle is less affected because it generates much lower intramural pressure.
Epicardial vs. Subendocardial blood flow: The subendocardial layers are most vulnerable because they face the highest compressive forces during systole. A subendocardial plexus of extra vessels partially compensates, but subendocardial ischemia occurs first when coronary pressure falls.
- Guyton and Hall Textbook of Medical Physiology
6. Regulation of Coronary Blood Flow
A. Local Metabolic Control (Primary)
The dominant controller of coronary flow is local metabolic demand. Blood flow tracks oxygen consumption of the myocardium.
- ~70% of oxygen in coronary arterial blood is extracted at rest - one of the highest extraction rates in the body
- There is very little oxygen reserve, so increased demand must be met by increased flow
- When O2 demand rises, local hypoxia and adenosine accumulate, causing coronary arteriolar vasodilation → increased flow (active hyperemia)
Adenosine is the most important mediator: when cardiac work increases, ATP breakdown produces adenosine, which is a potent vasodilator of coronary arterioles.
Other local vasodilators: CO2, H+, K+, NO (nitric oxide from the endothelium).
B. Mechanical Compression
As described above, systolic compression reduces coronary flow temporarily. At the end of systole (when compression is released), reactive hyperemia repays the "oxygen debt" incurred during the compression period.
C. Neural and Hormonal Control (Minor Role)
-
Sympathetic nerves have both α1 (vasoconstricting) and β2 (vasodilating) receptors on coronary vessels
-
During exercise, sympathetic activation can cause vasoconstriction, but the powerful local metabolic vasodilation overrides this - net result is increased flow
-
Vagal (parasympathetic) stimulation has minimal direct coronary effect
-
Costanzo Physiology 7th Edition; Guyton and Hall Textbook of Medical Physiology
7. Summary Table
| Feature | Details |
|---|---|
| Origin of coronary arteries | Aortic sinuses (root of ascending aorta) |
| LCA territory | Anterior/lateral LV, anterior IVS, AV bundle |
| RCA territory | RV, posterior LV, SA node, AV node |
| Dominant vessel (80-90%) | RCA (gives posterior descending artery) |
| Normal coronary flow | ~225 mL/min at rest (4-5% of cardiac output) |
| Primary flow regulator | Local metabolic demand (adenosine, hypoxia) |
| When does LCA fill? | Predominantly during diastole |
| Most vulnerable layer | Subendocardium (highest compressive force) |
| Main venous drainage | Coronary sinus → right atrium |
8. Clinical Relevance
- LAD occlusion ("widow maker") - causes anterior MI; worst prognosis
- RCA occlusion - can cause inferior MI + heart block (knocks out SA/AV nodes)
- LCx occlusion - causes lateral MI; often "silent" on ECG
- Subendocardial ischemia appears first on ECG as ST depression
- Transmural (full thickness) ischemia causes ST elevation (STEMI)
This foundation is the basis for understanding ECG localization of MI, coronary angiography interpretation, and interventional cardiology (PCI, CABG).
This is a shared conversation. Sign in to Orris to start your own chat.