Diplopia clinical evaluation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive material across all key areas. Let me compile the full clinical evaluation guide.
Diplopia: Clinical Evaluation
1. First Step - Monocular vs. Binocular
The single most important initial question is: does the diplopia persist when one eye is covered?
| Feature | Monocular Diplopia | Binocular Diplopia |
|---|---|---|
| Persists with one eye covered? | Yes | No - resolves |
| Cause | Intrinsic to the eye | Misalignment of visual axes |
| Clinical urgency | Usually benign | Can be emergent |
Monocular diplopia is caused by ocular-level pathology and carries no dire neurological implications. The second image is often a blurry "ghost" or halo. A pinhole may dramatically reduce symptoms. Causes include:
- Refractive error / uncorrected astigmatism
- Keratoconus, pterygium, corneal surface abnormality
- Tear film disorder / dry eye
- Cataract, lens subluxation, intraocular lens decentration
- Epiretinal membrane or retinal scar
- Malingering / psychiatric disease
A special subtype is cerebral polyopia (occipital/parieto-occipital lesion): multiple images persist with equal clarity, are not improved by pinhole, and are unchanged monocularly vs. binocularly. Associated findings include homonymous field defects, visual agnosia, and dyschromatopsia. - Localization in Clinical Neurology, 8e
Binocular diplopia resolves when either eye is covered and always signals a disruption of ocular alignment requiring further evaluation.
2. History
Once binocular diplopia is confirmed, the history should address:
- Direction: purely horizontal vs. vertical vs. oblique/torsional
- Gaze position: which direction of gaze worsens it (maximum separation = paretic direction)
- Onset: sudden (vascular, aneurysm) vs. gradual (tumor, demyelination, thyroid)
- Intermittency and diurnal variation: fatigable worsening in the evening suggests myasthenia gravis
- Pain: orbital or periorbital pain narrows the differential significantly
- Associated neurological symptoms: dysarthria, dysphagia, ataxia, vertigo, limb weakness - these point to brainstem pathology
- Systemic history: diabetes, hypertension (microvascular ischemia), thyroid disease, recent trauma, cancer, prior MS
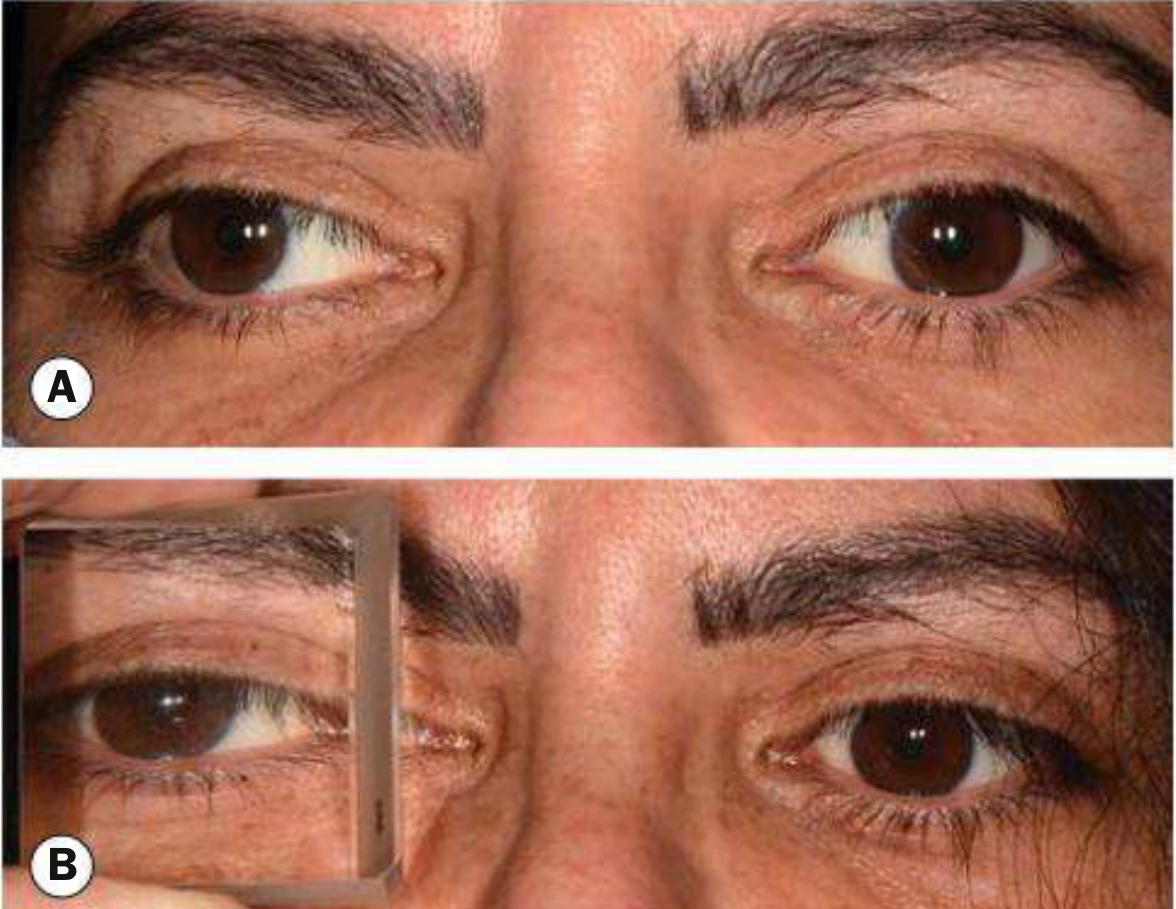
3. Cover Test
The cover test is the most sensitive bedside method for detecting ocular misalignment, often revealing a defect even when formal motility testing looks full. - Harrison's 22E
Cover-uncover test: The patient fixates a distant target. Cover one eye - watch the other (uncovered) eye for a refixation movement. A shift indicates a tropia (manifest deviation):
- Eye shifts inward on uncovering = exotropia
- Eye shifts outward on uncovering = esotropia
Cross-cover (alternate cover) test: Prevents binocular fusion by always keeping one eye covered. Reveals phorias (latent deviations overcome by fusion) in addition to tropias. Many normal people are slightly exophoric.
The cover test should be performed in primary gaze, then with head turned and tilted in each direction while fixating a central distant target. A subtle CN VI palsy may only be unmasked by turning the head so the eyes enter the paretic direction.
Comitant vs. incomitant deviation:
- Comitant: misalignment equal in all gaze directions - indicates congenital strabismus, not a new cranial nerve palsy
- Incomitant: misalignment that changes with gaze direction - indicates a paretic or restrictive cause
4. Cranial Nerve Palsies
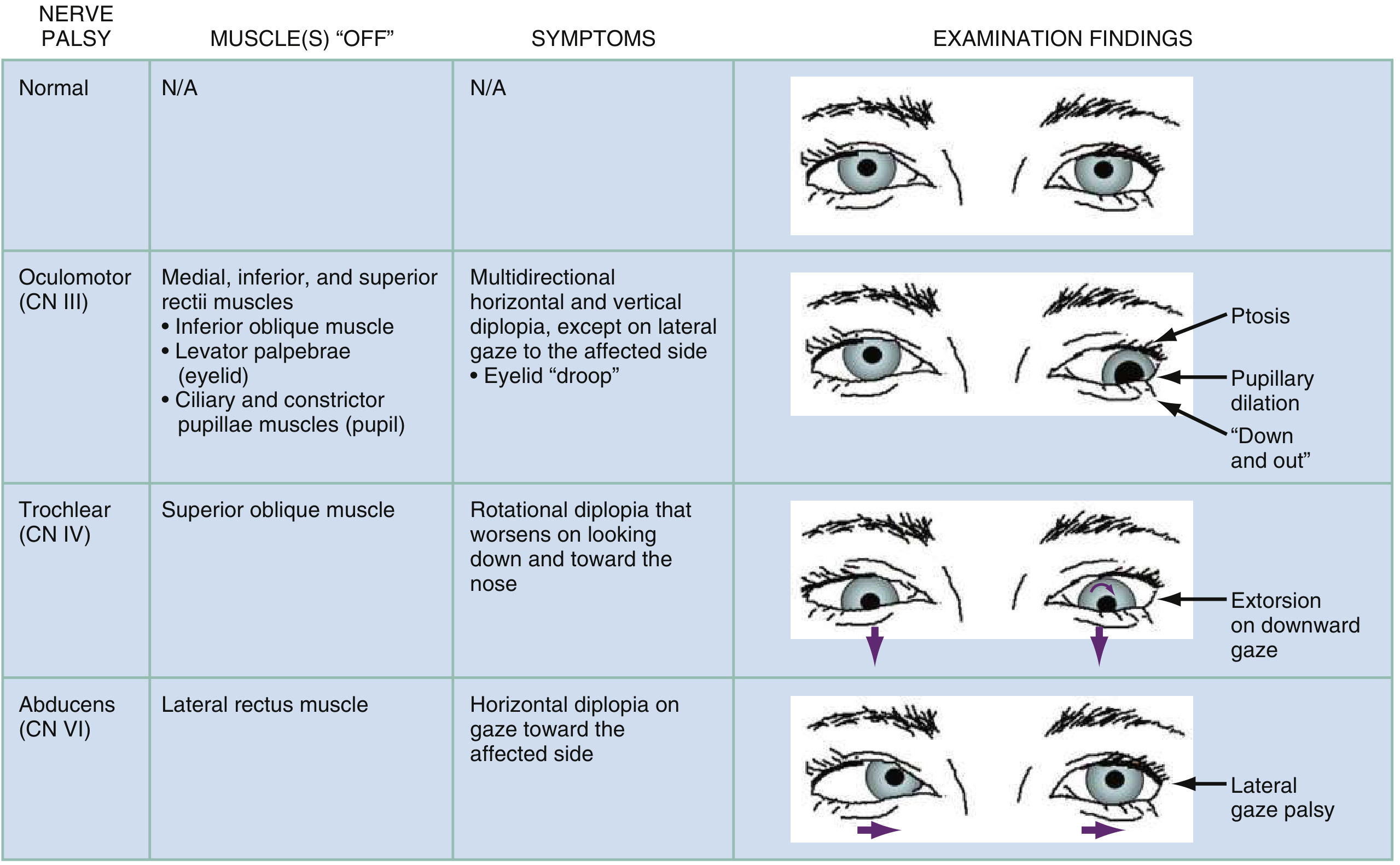
CN III (Oculomotor) Palsy
CN III innervates the medial, inferior, and superior recti; inferior oblique; levator palpebrae; and the pupillary sphincter/ciliary muscle.
Complete CN III palsy: ptosis + dilated pupil + eye deviated "down and out" (unopposed action of lateral rectus and superior oblique).
Key distinction - pupil involvement:
- Pupil-involving CN III palsy (dilated, poorly reactive): compressive lesion until proven otherwise - posterior communicating artery aneurysm, transtentorial herniation. Requires urgent neuroimaging + CTA/MRA.
- Pupil-sparing CN III palsy: most often microvascular ischemia (diabetes, hypertension). Spontaneous recovery expected over weeks to months. However, pupil-sparing is not fully reliable - partial compression can spare the pupil early.
Pain: can accompany both aneurysmal compression AND microvascular ischemia, so pain alone does not distinguish them.
Nuclear CN III lesion (rostral midbrain) produces distinctive signs: bilateral ptosis (single central subnucleus for levator), plus weakness of the contralateral superior rectus (crossed innervation). - Harrison's 22E
Midbrain fascicular syndromes involving CN III:
- Weber's syndrome: CN III palsy + contralateral hemiparesis (cerebral peduncle)
- Benedikt's syndrome: CN III palsy + contralateral tremor/chorea (red nucleus)
- Nothnagel's syndrome: CN III palsy + contralateral cerebellar ataxia (superior cerebellar peduncle)
- Claude's syndrome: combines Benedikt + Nothnagel features
Aberrant regeneration: after trauma or compression (not microvascular ischemia). Miswired fibers cause lid elevation on downgaze or adduction; pupil constriction on adduction. Its presence excludes microvascular etiology.
CN IV (Trochlear) Palsy
CN IV innervates the superior oblique (depresses, intorts, and abducts the adducted eye).
Symptoms: vertical/torsional diplopia worst on looking down and toward the nose - difficulty descending stairs, reading, watching TV in bed. - Rosen's Emergency Medicine
CN IV is the most susceptible to trauma (lies against the tentorium). Bilateral CN IV palsy after head trauma is well recognized.
Three-step test for identifying the paretic vertical muscle:
- Step 1: Determine which eye is hypertropic (higher) in primary gaze
- Step 2: Look to each side - note which lateral gaze position worsens the hypertropia
- Step 3: Look up and down in that direction - the gaze that worsens it identifies the muscle (downgaze = superior oblique; upgaze = inferior rectus)
Bielschowsky head-tilt test (Step 4 / confirmatory):
- Tilting the head toward the side of a weak superior oblique increases image separation
- Head tilt to the opposite side makes images fuse
- Mechanism: normal head tilt triggers ocular counterrolling via paired superior oblique + superior rectus contraction; with SO palsy, only the superior rectus contracts, elevating and intorting the eye, worsening the hypertropia. - Localization in Clinical Neurology, 8e
A compensatory head tilt away from the affected side in a patient's photographs or posture should always prompt evaluation for a CN IV palsy.
CN VI (Abducens) Palsy
CN VI innervates only the lateral rectus.
Symptoms: horizontal diplopia that worsens on gaze toward the affected side. The eye fails to abduct. Patient often adopts a face turn toward the side of the palsy.
CN VI is the most common cranial nerve palsy (50% of all CN palsies) due to its long intracranial course. It is also uniquely vulnerable to raised intracranial pressure (false localizing sign). - Rosen's Emergency Medicine
Bilateral CN VI palsies suggest elevated ICP - look for papilledema, headache, nausea/vomiting (idiopathic intracranial hypertension).
5. Restrictive vs. Neurogenic Diplopia
When cranial nerve palsies are not present, orbital restriction must be considered.
| Feature | Neurogenic (CN palsy) | Restrictive (Orbital) |
|---|---|---|
| Onset | Often sudden | Usually gradual |
| Pain | Variable | Common (mass effect) |
| Proptosis | Absent | Often present |
| Conjunctival injection | Absent | May be present |
| Forced duction test | Negative | Positive |
| Imaging | Normal orbit | Abnormal orbital contents |
Causes of restrictive diplopia:
- Thyroid eye disease (Graves'): inferior and medial recti most affected → restriction of elevation and abduction. Associated with proptosis, lid retraction, lid lag, chemosis. Can precede systemic thyroid abnormalities.
- Orbital blowout fracture: inferior rectus entrapment → limitation of upgaze, worsening vertical diplopia on upgaze
- Orbital pseudotumor / myositis: painful, often with proptosis and injection
- Orbital infection/abscess: fever, periorbital swelling, restricted motility
- Orbital tumor or metastasis
Dedicated high-resolution MRI with fat saturation and gadolinium is the imaging of choice for orbital causes. - Harrison's 22E
6. Neuromuscular Junction Disorders
Myasthenia Gravis
A major and common cause of painless, fluctuating diplopia. Key features:
- Intermittent and variable - not confined to any single CN distribution
- Fatigable ptosis - worsens with sustained upgaze or at the end of the day
- Pupils always normal (critical distinguishing feature)
- Can mimic any CN palsy pattern
- Purely ocular form common; seronegative (anti-AChR and anti-MuSK negative) cases frequent in ocular myasthenia
If restrictive disease and myasthenia gravis are excluded, a cranial nerve lesion is the most likely diagnosis. - Harrison's 22E
Botulism (food or wound) can closely mimic ocular myasthenia and should be considered with descending flaccid paralysis, multiple cranial nerve palsies, and autonomic features (dry mouth, decreased bowel sounds, urinary retention).
7. Supranuclear and Internuclear Causes
These cause gaze palsies rather than isolated muscle weakness and often do not produce diplopia in the classic sense, but they are part of the ocular motility examination.
Internuclear Ophthalmoplegia (INO)
Caused by damage to the medial longitudinal fasciculus (MLF), which connects the abducens nucleus (pons) to the contralateral oculomotor nucleus (midbrain).
- Ipsilateral adduction failure on lateral gaze (the eye that should adduct does not)
- Contralateral abducting nystagmus (the abducting eye has gaze-evoked nystagmus)
- Convergence may be preserved (distinguishes INO from a medial rectus palsy)
- Bilateral INO in a young patient = multiple sclerosis until proven otherwise
- Other causes: stroke, brainstem tumor, trauma
One-and-a-half syndrome: MLF lesion + ipsilateral PPRF or abducens nucleus lesion. Only movement preserved is abduction of the contralateral eye. - Harrison's 22E
Parinaud's Syndrome (Dorsal Midbrain Syndrome)
Caused by damage to the posterior commissure (pineal tumor, hydrocephalus, midbrain infarct, cysticercosis).
- Loss of upgaze (may also affect downgaze)
- Convergence-retraction nystagmus on attempted upgaze
- Downward ocular deviation ("setting sun" sign)
- Lid retraction (Collier's sign)
- Light-near dissociation of pupils
- Skew deviation
Cavernous Sinus and Orbital Apex Syndromes
Multiple CN palsies (III, IV, VI) on the same side = cavernous sinus or orbital apex pathology.
- Cavernous sinus: CN VI often involved first (traverses through sinus; III and IV lie in the wall). Associated V1/V2 facial numbness/dysesthesia. Bilateral involvement possible (sinuses communicate).
- Orbital apex: same as cavernous sinus but also involves the optic nerve → decreased visual acuity is the distinguishing feature.
- Causes: thrombosis, infection (mucormycosis in diabetics/immunocompromised), tumor, trauma, herpes zoster ophthalmicus, Tolosa-Hunt syndrome.
8. Brainstem / Diffuse Neurological Causes
Red flags suggesting a brainstem origin:
- Diplopia + vertigo, nausea, dysphagia, dysarthria, ataxia
- Sudden painless onset + fluctuation → impending basilar artery occlusion (emergency)
- Gradual progressive → brainstem mass
- Young patient with headache + ophthalmoplegia → ophthalmoplegic migraine
Botulism: gradual combination of double vision, slurred speech, dysphagia, dry mouth, descending flaccid paralysis, autonomic signs.
Miller Fisher syndrome (GBS variant): ophthalmoplegia + ataxia + areflexia triad; anti-GQ1b antibodies.
9. Approach Summary
Diplopia
│
├─ Monocular (persists with fellow eye covered)
│ → Ocular cause: refraction, cornea, lens, retina, dry eye
│ → Cerebral polyopia if: images equal clarity, no pinhole improvement
│
└─ Binocular (resolves with either eye covered)
│
├─ Comitant deviation → Congenital strabismus
│
└─ Incomitant deviation
│
├─ Restrictive signs (proptosis, injection, forced duction+)
│ → Thyroid eye disease, orbital fracture, tumor, infection
│
├─ Fatigable, variable, pupils normal
│ → Myasthenia gravis; exclude botulism
│
├─ Single CN palsy
│ ├─ CN III with pupil involvement + pain → Aneurysm (URGENT CTA/MRA)
│ ├─ CN III pupil-sparing, microvascular risk → Ischemic, observe
│ ├─ CN IV → Trauma, head tilt, three-step test
│ └─ CN VI → Vascular, elevated ICP if bilateral
│
├─ Multiple CN palsies (same side)
│ → Cavernous sinus / orbital apex (add: VA, facial sensation)
│
├─ INO (adduction failure + contralateral nystagmus)
│ → MS (bilateral), brainstem stroke/tumor
│
└─ Brainstem signs (vertigo, dysarthria, ataxia, diplopia)
→ Basilar artery territory (urgent), MS, tumor
Key "Do Not Miss" diagnoses:
| Diagnosis | Clue |
|---|---|
| Posterior communicating artery aneurysm | CN III + pupil dilation + pain |
| Basilar artery occlusion | Sudden diplopia + brainstem signs, fluctuating |
| Cavernous sinus thrombosis | Multiple CN palsies + fever + proptosis, may be bilateral |
| Transtentorial herniation | CN III palsy with altered consciousness |
| Idiopathic intracranial hypertension | CN VI palsy + papilledema + headache, vision change |
| Orbital apex syndrome | Multiple CN palsies + decreased visual acuity (optic nerve) |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Rosen's Emergency Medicine, 10e; Adams and Victor's Principles of Neurology, 12e; Localization in Clinical Neurology, 8e
All cover tests in details
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from Kanski's Clinical Ophthalmology, Wills Eye Manual, and Bradley & Daroff's Neurology. Let me compile the full, detailed reference.
Cover Tests in Detail
Cover tests form the core of objective ocular alignment assessment. They work by systematically disrupting binocular fusion to unmask deviations. There is a strict sequence: always perform the cover-uncover test before the alternate cover test, as the latter destroys the information the former is designed to detect.
Preliminary: Light Reflex Tests (Not True Cover Tests, but the Starting Point)
Before any cover test, the examiner should use corneal light reflex tests when patients are uncooperative or have poor fixation in one eye.
Hirschberg Test
A pen torch is shone from arm's length with the patient fixating the light. The corneal reflex position is observed in each eye.
- Normal: reflex centred symmetrically in both pupils (or both slightly nasal - "angle kappa")
- In strabismus: the reflex is decentred in the squinting eye, in the direction opposite to the deviation
- Reflex displaced temporally = esotropia
- Reflex displaced nasally = exotropia
Quantification: 1 mm of decentration = 7° of deviation (1° ≈ 2 prism diopters).
- At pupil edge (2 mm off centre): ~15°
- At limbus: ~45°
Limitation: Accuracy depends on pupil size. Best used as a rough estimate or to exclude pseudostrabismus. - Kanski's Clinical Ophthalmology, 10e
Krimsky Test
Combines the Hirschberg with prisms to quantify a manifest deviation more accurately.
- Prisms are placed in front of the fixating eye (apex toward the deviation direction) until corneal light reflexes become symmetrical
- More commonly used than the prism reflection test because placing the prism before the fixating eye reduces parallax error
Prism reflection test (variant): prisms placed before the deviating eye instead.
Test 1: Cover-Uncover Test
Purpose: Detects a tropia (manifest deviation present when both eyes are open).
This is the first cover test to perform. It should always be done before the alternate cover test.
Requirements
- Adequate vision in each eye to fixate on a target
- Foveal fixation in each eye
- Full or adequate range of ocular motility
- Patient cooperation
- Best optical correction worn
- Wills Eye Manual
Target
Use an accommodative target (a letter on the distance chart), not a light source. A light does not stimulate accommodation and will not reveal accommodative esotropia. Test at distance (6 m) and at near (1/3 m). - Kanski's Clinical Ophthalmology
Procedure - Part 1 (Cover test): Detecting tropia
- Ask the patient to fixate a distance target.
- Cover one eye (e.g., left eye) and watch the uncovered eye (right eye).
- If the right eye moves to take up fixation → it was misaligned = tropia present
- If the right eye does not move → it was already fixing = no deviation of the right eye (either orthotropia or the right eye was already the fixating eye in a left tropia)
- Repeat by covering the other eye (right eye), observing the left eye.
Interpreting the movement of the uncovered eye:
| Movement of uncovered eye | Diagnosis |
|---|---|
| Moves inward (adducts) | Exotropia (eye was deviated outward) |
| Moves outward (abducts) | Esotropia (eye was deviated inward) |
| Moves downward | Hypertropia (eye was deviated upward) |
| Moves upward | Hypotropia (eye was deviated downward) |
| No movement | No tropia in that eye (orthotropia or that eye is fixating) |
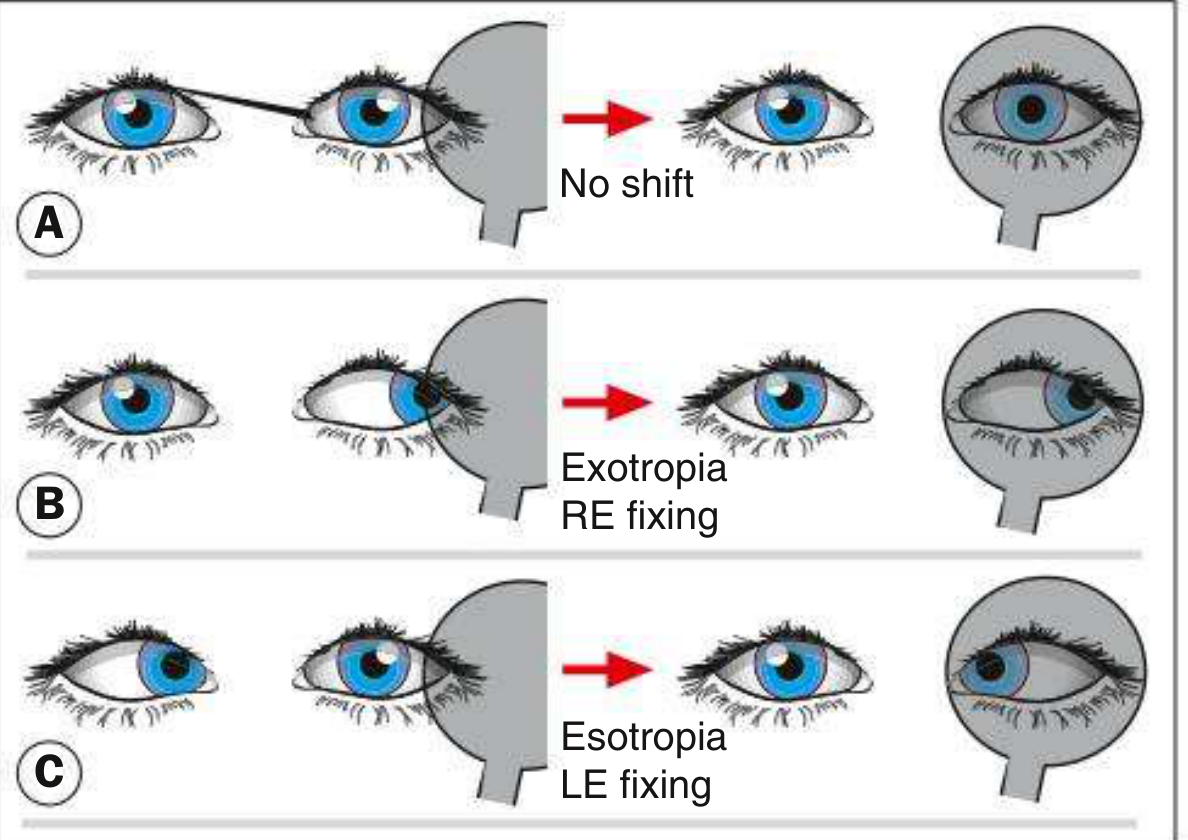
Key rule: always watch the eye that is not being covered. - Bradley & Daroff's Neurology in Clinical Practice
A movement of the uncovered eye may not occur if it is already the preferred (fixating) eye. If you cover the fixating eye, the deviating eye must take up fixation and will move. If you cover the deviating eye, the fixating eye was already on target and will not move.
Procedure - Part 2 (Uncover test): Detecting phoria
After covering one eye for 2-3 seconds, remove the cover and watch the previously covered eye.
- No movement: the eye maintained alignment under cover = orthophoria (or the deviation is too small to detect)
- Movement to regain fixation: the eye drifted under cover and now refixates = heterophoria (latent deviation normally suppressed by fusion)
- Eye moves inward (adducts) on uncovering → it had drifted outward = exophoria
- Eye moves outward (abducts) on uncovering → it had drifted inward = esophoria
- Eye moves downward on uncovering → hyperphoria
Speed and smoothness of recovery reflects the strength of motor fusion. Slow, effortful recovery indicates poor fusional reserves. - Kanski's Clinical Ophthalmology
Test 2: Alternate Cover Test (Cross-Cover Test)
Purpose: Detects the total deviation (tropia + phoria combined) by completely dissociating the eyes. It does not distinguish manifest from latent deviation on its own.
Rule: Always perform the cover-uncover test first. The alternate cover test must come second. - Wills Eye Manual; Kanski's; Bradley & Daroff
Procedure
- Patient fixates a distant accommodative target.
- Cover one eye for at least 4 seconds.
- Rapidly shift the cover to the other eye (do not allow any binocular viewing).
- Repeat several times back and forth, always keeping one eye covered.
- Observe the eye being uncovered for a refixation movement.
The constant alternation prevents fusion at all times. The covered eye, freed from the obligation to fuse, drifts to its position of rest (the anatomical resting position, typically slightly divergent).
Interpretation
- Orthotropic patient with orthophoria: no movement seen at all; the covered eye stays aligned and the uncovered eye doesn't shift
- Orthotropic patient with exophoria: the eye drifts outward under cover; when uncovered, it swings back inward (adducts) to refixate
- Tropia present: larger refixation movements seen that represent the total deviation
Because the alternate cover test always has one eye covered, it continuously disrupts fusion and shows the maximum possible deviation - the sum of the manifest tropia (if any) and the latent phoria component. This total is always ≥ the tropia measured by the cover-uncover test alone. - Wills Eye Manual
What it cannot do: It cannot tell you what portion of the total deviation is tropia vs. phoria. For that, you compare the two tests.
Comitance Check
After establishing the total deviation, repeat the alternate cover test in all nine diagnostic positions of gaze:
- Primary position
- Right and left gaze
- Up, down, and the four oblique directions
If the deviation stays the same in all positions = comitant (congenital strabismus, not a new palsy).
If the deviation varies with gaze direction = incomitant (paralytic or restrictive). - Bradley & Daroff
Test 3: Alternate Cover Test with Prism (Prism Alternate Cover Test - PACT)
Purpose: Measures the angle of the total deviation in prism diopters (Δ).
This is the standard method for quantifying strabismus and is the most precise cover-based measurement. - Wills Eye Manual; Kanski's

Procedure
- Perform the alternate cover test first to confirm direction and estimate extent of deviation.
- Place a prism in front of one eye with the prism base in the direction of the refixation movement (opposite to the direction of the deviation):
- Esotropia → base-out prism
- Exotropia → base-in prism
- Right hypertropia → base-down prism before right eye (or base-up before left)
- Continue alternating the cover while holding the prism in place. Gradually increase prism strength (using a prism bar) until the refixation movement is eliminated.
- The endpoint: the weakest prism that produces no movement. To confirm, go slightly beyond (reversal point) - a movement in the opposite direction - then reduce to find the neutral value.
Measurements should be taken in:
- Primary gaze (distance and near, with and without glasses)
- Right gaze, left gaze
- Upgaze, downgaze
- Head tilted right, head tilted left (essential when a vertical deviation is present, for the Bielschowsky three-step test)
1 prism diopter = deflects a ray of light 1 cm at 1 m distance. 1° of deviation ≈ 2Δ. - Kanski's Clinical Ophthalmology
Test 4: Simultaneous Prism-Cover Test (SPCT)
Purpose: Measures only the manifest (tropia) component of the deviation, without dissociating a latent component (phoria).
This test is particularly useful when you want to know the true tropia size independent of the phoria, for example, to compare with the PACT and calculate the phoria contribution (PACT - SPCT = phoria component).
Procedure
- With both eyes open, the patient fixates a distance target.
- Simultaneously: place a cover over one eye AND introduce a prism before the other eye.
- The cover prevents the covered eye from fusing. The prism is adjusted until the fixating (uncovered) eye shows no refixation movement.
- The prism power at which no movement occurs = the size of the tropia.
Summary Comparison Table
| Test | What It Detects | What It Measures | Key Limitation |
|---|---|---|---|
| Hirschberg | Manifest deviation (rough) | Estimates angle (~7°/mm) | Not precise; depends on pupil size |
| Krimsky | Manifest deviation | Quantifies with prisms | Parallax error less than prism reflection |
| Cover-Uncover | Tropia (manifest) + Phoria (latent; uncover phase) | Qualitative direction | Cannot measure angle alone |
| Alternate Cover (cross-cover) | Total deviation (tropia + phoria) | Qualitative; maximum dissociation | Cannot separate tropia from phoria |
| Prism Alternate Cover (PACT) | Total deviation | Quantifies angle in prism diopters | Includes both manifest + latent |
| Simultaneous Prism-Cover (SPCT) | Manifest tropia only | Quantifies tropia in prism diopters | Does not capture phoria |
| PACT minus SPCT | Phoria component | Derived calculation | Requires both tests |
Fixation Switch Diplopia (Special Finding on Cover Testing)
In patients with long-standing strabismus who develop decreased acuity in the fixating eye (e.g., due to cataract or refractive error), switching fixation to the previously deviating eye causes misalignment of the previously dominant eye, producing diplopia. This "fixation switch diplopia" can be revealed during cover testing and is usually treatable with optical correction. - Bradley & Daroff's Neurology in Clinical Practice
Postoperative Diplopia Test (Pre-surgical Screening)
Before strabismus surgery in any non-binocular patient aged >7-8 years, this test is mandatory to assess the risk of postoperative diplopia.
- Corrective prisms are placed before one eye and gradually increased to overcorrect the angle.
- The patient reports whether diplopia occurs.
- If suppression persists throughout the overcorrection: low risk of postoperative diplopia.
- If diplopia is reported: the patient may experience diplopia post-surgery → an indication for a diagnostic botulinum toxin test before proceeding. - Kanski's Clinical Ophthalmology, 10e
Practical Sequence for Clinical Use
1. Hirschberg / Krimsky (if uncooperative or poor fixation in one eye)
↓
2. Cover-Uncover Test
- Part 1 (Cover): watch uncovered eye → tropia?
- Part 2 (Uncover): watch previously covered eye → phoria?
- Test at distance AND near, with and without glasses
↓
3. Alternate Cover Test
- Confirm total deviation direction
- Check in all 9 positions of gaze → comitant or incomitant?
↓
4. Prism Alternate Cover Test (PACT)
- Quantify total angle in prism diopters
- Test in all positions (primary, cardinal gazes, head tilts)
↓
5. Simultaneous Prism-Cover Test (optional)
- Quantify manifest tropia component only
- PACT - SPCT = phoria component
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10e; Wills Eye Manual, 8e; Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology, 8e
This is a shared conversation. Sign in to Orris to start your own chat.