congenital heart defects in adults
Reading File
Finding Sources
Searching PubMed
"congenital heart disease" AND "adults" AND management
Reading File
Finding Sources
Reading Article
PMID: 41411480
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive content. Let me compile the full, detailed response.
Congenital Heart Defects in Adults (ACHD)
Overview
Thanks to major advances in pediatric cardiology and cardiac surgery, the population of adults with congenital heart disease (ACHD) is now larger than the pediatric population with the same conditions. An estimated 2.4 million people currently live with congenital heart disease in the United States, and roughly two-thirds of them are adults. An overall prevalence of 3-4 per 1,000 adults has been documented. Nearly 300,000 Americans have severe congenital heart disease (defined as two or more abnormalities, typically associated with cyanosis at birth).
Guideline update: The 2025 ACC/AHA/HRS/ISACHD/SCAI Guideline for ACHD management was published in February 2026 (PMID: 41411480), replacing the 2018 guidelines. This is now the current standard of care reference.
Epidemiology: Common Lesions in Adults
| Lesion | Prevalence in Adults |
|---|---|
| Bicuspid aortic valve | ~2% of general population; most common congenital cardiac anomaly in adults |
| Atrial septal defect (ASD) | 30-40% of CHD cases in adults; ostium secundum = 7% of all congenital lesions |
| Ventricular septal defect (VSD) | 15-20% of all congenital lesions (many close spontaneously, so fewer in adults) |
| Patent ductus arteriosus (PDA) | 5-10% of congenital cardiac lesions |
| Pulmonary stenosis / Coarctation of the aorta | 3-10% each |
| Tetralogy of Fallot (ToF) | Most common cyanotic lesion encountered in adults |
More complex lesions (tricuspid atresia, univentricular heart, Ebstein anomaly, double-outlet RV) each account for 2.5% or less.
- Goldman-Cecil Medicine, p. 604
Genetic Associations
About 20% of congenital heart defects are associated with a syndrome or chromosomal anomaly:
-
Down syndrome (trisomy 21): ~50% have endocardial cushion defects and VSD
-
Trisomy 13 and 18: VSDs in 90% of patients
-
Turner syndrome (45,X): aortic coarctation, aortic stenosis, ASD
-
22q11 deletion (DiGeorge / CATCH-22 syndromes): Tetralogy of Fallot (~15% of ToF patients); higher prevalence if right aortic arch is present
-
Noonan syndrome / Williams syndrome: associated with pulmonary stenosis
-
Goldman-Cecil Medicine, p. 604
Individual Lesions in Detail
1. Atrial Septal Defect (ASD)
Types: Ostium secundum (most common, amenable to percutaneous closure), ostium primum, sinus venosus, coronary sinus defect.
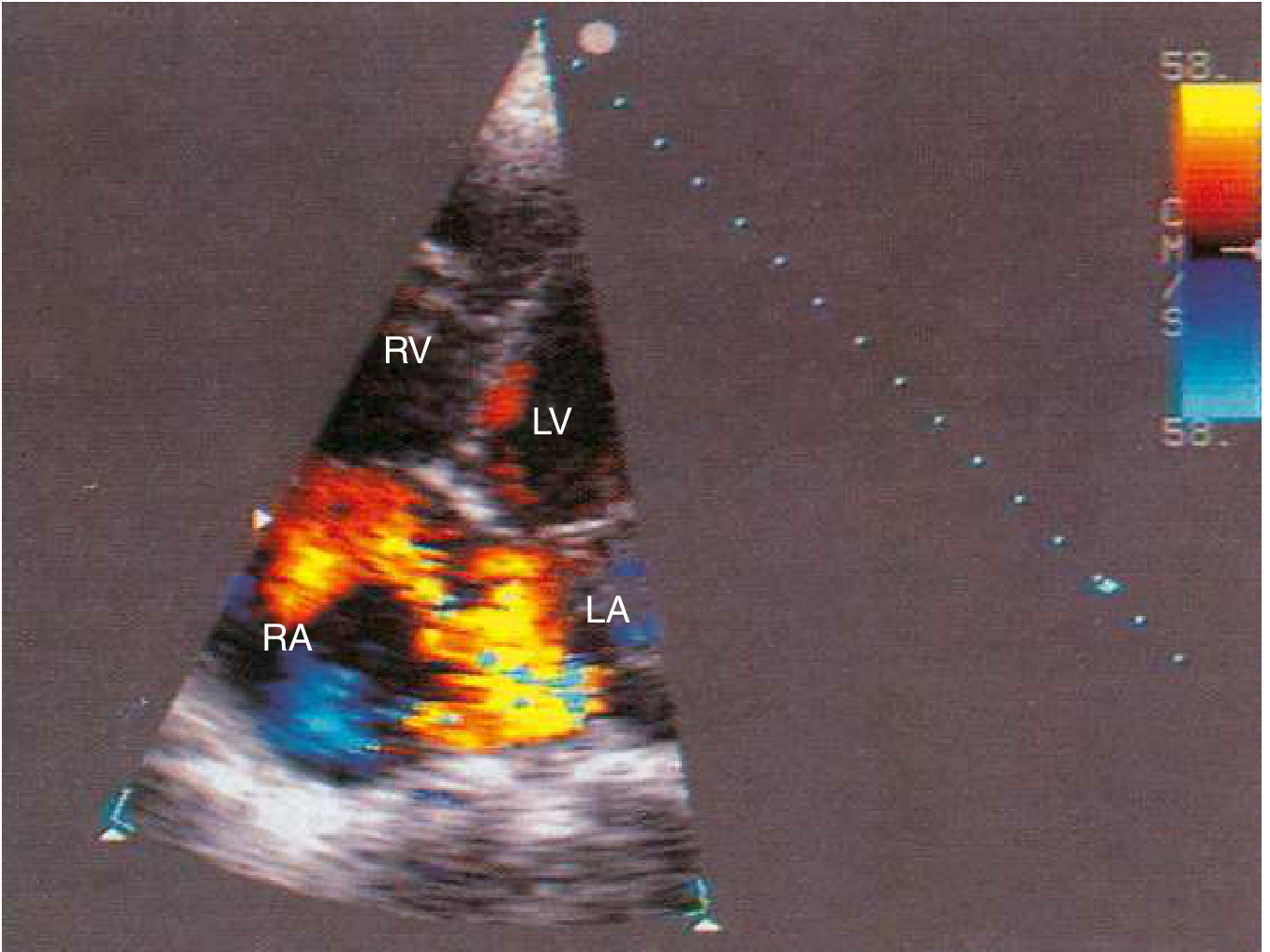
Clinical features in adults: Often asymptomatic and discovered incidentally on imaging. When symptomatic: exercise intolerance, palpitations, exertional dyspnea. Supraventricular arrhythmias develop in ~10% by age 40 and become increasingly common thereafter. Classic exam: wide, fixed splitting of S2; ECG shows rightward QRS axis and incomplete RBBB.
Chamber effects: ASD causes RA + RV + PA enlargement (see table below).
Repair: Indicated when there is right heart dilation ± symptoms with confirmed left-to-right shunt, PVR < 1/3 SVR, PA systolic pressure < 50% systemic, and Qp:Qs ≥ 1.5:1. Percutaneous closure is standard for secundum ASDs; surgical closure is required for sinus venosus, primum, and coronary sinus defects.
- Patients repaired before age 25 have favorable long-term outcomes; surgical repair does not reliably reduce arrhythmia burden in older adults.
Braunwald's Heart Disease, p. 878
2. Ventricular Septal Defect (VSD)
Types: Perimembranous (up to 80%), infundibular/supracristal, inlet, trabecular/muscular.
Natural history: ~50% of all VSDs are small; >50% of small VSDs close spontaneously. Spontaneous closure in adult life is unusual. Adults presenting with VSD typically have a small restrictive lesion.
Hemodynamics:
- Small (Qp:Qs < 1.5, normal PA pressure): minimal physiologic impact
- Moderate (Qp:Qs > 1.2, elevated PA pressure, normal PVR): LA and LV dilation
- Large/severe (Qp:Qs ≥ 1.5:1, elevated PA pressure and PVR): biventricular effects
- Eisenmenger complex develops in ~10% of unrepaired large VSDs
Chamber effects: VSD causes LA + LV + PA enlargement (RV enlargement only with pulmonary hypertension).
Goldman-Cecil Medicine, p. 610
Below is a color-flow Doppler echocardiogram showing a left-to-right atrial-level shunt (ASD):
3. Patent Ductus Arteriosus (PDA)
A moderate-to-large unrepaired PDA leads to progressive LA/LV dilation and pulmonary hypertension. By the fourth decade, mortality rises to 3-4% per year; two-thirds of untreated patients die by age 60. Eisenmenger complex develops in ~5% of isolated PDAs.
Exam: "Machinery" continuous murmur at the left infraclavicular area; bounding pulse with wide pulse pressure. With Eisenmenger physiology, the murmur disappears, lower extremity cyanosis/clubbing predominates (differential cyanosis - toes > fingers).
Treatment: Transcatheter or coil occlusion is the accepted approach in adults. Closure is contraindicated in established Eisenmenger syndrome.
Goldman-Cecil Medicine
4. Coarctation of the Aorta
Often presents in adulthood as unexplained upper extremity hypertension in young men. Features include:
- Blood pressure differential: arm > leg (popliteal systolic BP increase < 10 mmHg vs. arm)
- Pressure differential > 30 mmHg between arms suggests left subclavian involvement
- CXR: classic "3 sign" from dilated left subclavian artery and post-stenotic aortic dilation; bilateral rib notching (3rd-8th ribs)
- Complications: angina, heart failure, aortic dissection, intracranial aneurysm rupture
Treatment: Catheter-based intervention is preferred in adults when peak gradient ≥ 20 mmHg (catheterization) or with significant collateral flow. Up to 50% of patients repaired after age 40 have residual hypertension; those repaired at ages 1-5 have < 10% long-term hypertension prevalence.
Goldman-Cecil Medicine, p. 612
5. Tetralogy of Fallot (ToF)
The most common cyanotic congenital defect in adults. Classic anatomy:
- Large VSD (malalignment type)
- Right ventricular outflow tract (RVOT) obstruction
- RV hypertrophy
- Aorta overriding the VSD
Most adults with ToF have undergone prior surgical repair. Long-term issues post-repair include:
- Pulmonary regurgitation - the most common long-term problem; leads to progressive RV dilation and dysfunction
- Ventricular arrhythmias and sudden cardiac death
- Residual RVOT obstruction
- Re-operation for pulmonary valve replacement is often needed
Goldman-Cecil Medicine; Braunwald's Heart Disease
6. Pulmonary Stenosis
Valvular pulmonary stenosis is one of the more common CHD lesions. Severity classification:
- Mild: peak gradient ≤ 36 mmHg
- Moderate: 36-64 mmHg
- Severe: > 64 mmHg (usually intervened on in childhood)
Adults with mild-to-moderate PS may be asymptomatic but can develop progressive RV hypertrophy, exercise intolerance, and heart failure. If there is an associated PFO/ASD, a noncompliant RV can drive right-to-left shunting and cyanosis with exercise.
Braunwald's Heart Disease, p. 884
7. Eisenmenger Syndrome
A late-stage complication of any large unrepaired left-to-right shunt (ASD, VSD, PDA, AVSD). Elevated pulmonary vascular resistance eventually reverses the shunt direction to right-to-left, producing cyanosis and erythrocytosis.
Key features:
- Central cyanosis, digital clubbing
- Polycythemia/erythrocytosis (compensatory)
- Paradoxical embolism risk
- Closure of the defect is absolutely contraindicated once Eisenmenger physiology is established
Management: Pulmonary vasodilators (endothelin receptor antagonists, PDE-5 inhibitors), management of erythrocytosis, iron supplementation, careful use of anesthesia. Heart-lung transplantation is the definitive option in selected patients.
Goldman-Cecil Medicine; Braunwald's Heart Disease
Functional Capacity by Lesion Type
The chart below shows peak oxygen consumption (pVO2) as a percentage of predicted normal across different ACHD diagnoses - illustrating the wide variation in functional impairment:
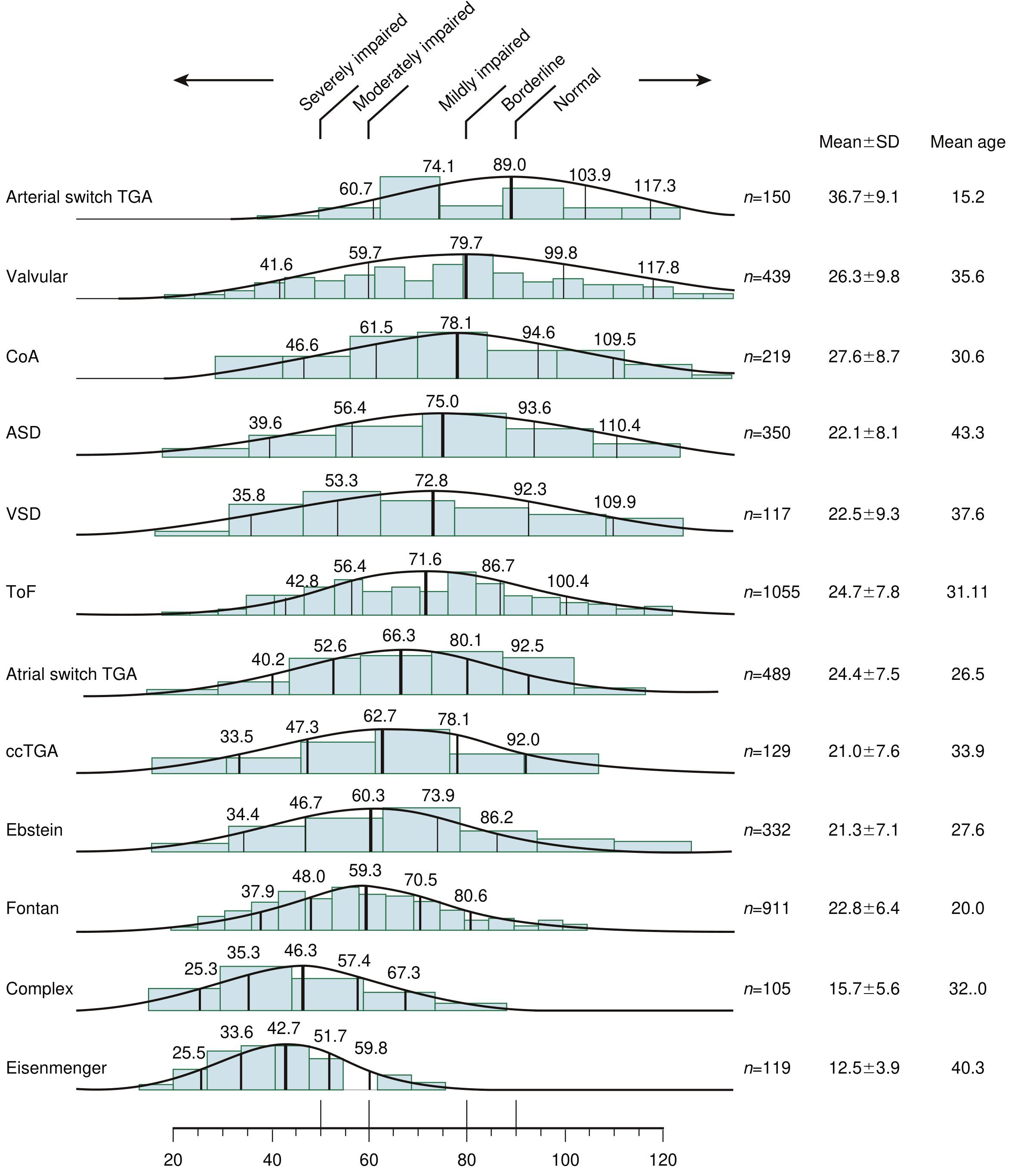
Range of peak oxygen consumption in various ACHD types. Eisenmenger patients have the most severely impaired exercise capacity; arterial switch TGA patients have near-normal values. (Braunwald's Heart Disease, Fig. 82.6)
Key observations:
- Eisenmenger syndrome: severely impaired pVO2 (mean ~51% predicted)
- Complex lesions / Fontan: moderately to severely impaired
- ToF, ccTGA, Ebstein anomaly: mildly to moderately impaired
- Valvular/ASD/CoA: closer to normal range
Complications in Adults with CHD
Regardless of original lesion or repair status, ACHD patients are at increased risk for:
| Complication | Notes |
|---|---|
| Arrhythmias | Atrial flutter/fibrillation very common (especially post-repair); VT/sudden death risk in ToF, Ebstein, systemic RV |
| Heart failure | Ventricular dysfunction from chronic volume/pressure overload or inadequate repair |
| Pulmonary hypertension | From longstanding left-to-right shunts; Eisenmenger is the extreme |
| Infective endocarditis | Risk increases with unrepaired defects, residual shunts, prosthetic material |
| Thromboembolic events | Paradoxical embolism via ASD/PFO; atrial thrombus with arrhythmia |
| Aortic complications | Dilation/dissection in bicuspid aortic valve, Marfan syndrome, CoA |
High-Intensity Exercise: Conditions to Avoid It
Per the AHA/ACC guidelines (Braunwald's, Table 82.8), high-intensity exercise should be avoided in ACHD patients with any of:
- Cyanosis / hypoxemia
- Severe pulmonary hypertension
- Severe ventricular dysfunction
- Severe outflow tract obstruction
- Severe aortic dilation
- Ventricular arrhythmias
- High-risk coronary anomalies
Principles of Adult Management
- Specialist care: All ACHD patients should be followed at ACHD-designated centers; complexity determines follow-up frequency.
- Imaging: Echocardiography is the primary modality; CMR (cardiac MRI) is superior for RV quantification (critical in ToF), aortic anatomy (CoA), and complex anatomy.
- Pregnancy: Many ACHD patients can safely complete pregnancy but require pre-conception risk stratification (modified WHO classification). Eisenmenger syndrome carries >30-50% maternal mortality.
- Reoperation / Reintervention: Common - pulmonary valve replacement in ToF, valve replacement in bicuspid AV disease, conduit revision after Rastelli procedures.
- Endocarditis prophylaxis: Recommended for unrepaired or residual defects, prosthetic valves/material, and prior endocarditis.
Sources
- Goldman-Cecil Medicine International Edition, pp. 604-614 (Chapter 55: Congenital Heart Disease in Adults)
- Braunwald's Heart Disease, pp. 877-884 (Chapter 82: Adult Congenital Heart Disease)
- 2025 ACC/AHA/HRS/ISACHD/SCAI Guideline for Management of Adults With Congenital Heart Disease (PMID: 41411480) - published February 2026, this is the current guideline replacing the 2018 version
This is a shared conversation. Sign in to Orris to start your own chat.