Anatomy and blood supply of Spinal Cord
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Let me compile it.
Anatomy and Blood Supply of the Spinal Cord
1. General Overview
The spinal cord is a cylindrical extension of the brainstem that passes through the vertebral canal. It is shorter than the vertebral column, terminating as the conus medullaris at approximately L1-L2 in adults (L3 in neonates). From the conus, a fibrous strand - the filum terminale - descends to attach to the dorsum of the first coccygeal segment.
The cord is enclosed in three meningeal layers:
- Pia mater - innermost, closely adherent
- Arachnoid mater - middle layer; separated from pia by the subarachnoid space (contains CSF)
- Dura mater - outermost tough layer
2. Spinal Cord Segments and Nerve Roots
The cord gives rise to 31 pairs of spinal nerves (8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal).
Key rule for nerve root exit:
- C1-C7: exit above the pedicle for which they are named (C6 root exits between C5 and C6 pedicles)
- C8: exits between C7 and T1 pedicles
- T1 and below: exit below the pedicle for which they are named (L4 root exits between L4 and L5 pedicles)
Because the cord is shorter than the column, lumbar and sacral roots travel long distances inside the canal before exiting, forming the cauda equina below the conus.
3. External Features
| Feature | Details |
|---|---|
| Cervical enlargement | C4-T1; for the brachial plexus/upper limb |
| Lumbosacral enlargement | L1-S3; for the lumbosacral plexus/lower limb |
| Anterior median fissure | Deep midline groove on ventral surface |
| Posterior median sulcus | Shallow midline groove on dorsal surface |
| Anterolateral sulcus | Exit of ventral (motor) roots |
| Posterolateral sulcus | Entry of dorsal (sensory) roots |
4. Internal Structure - Cross-Sectional Anatomy
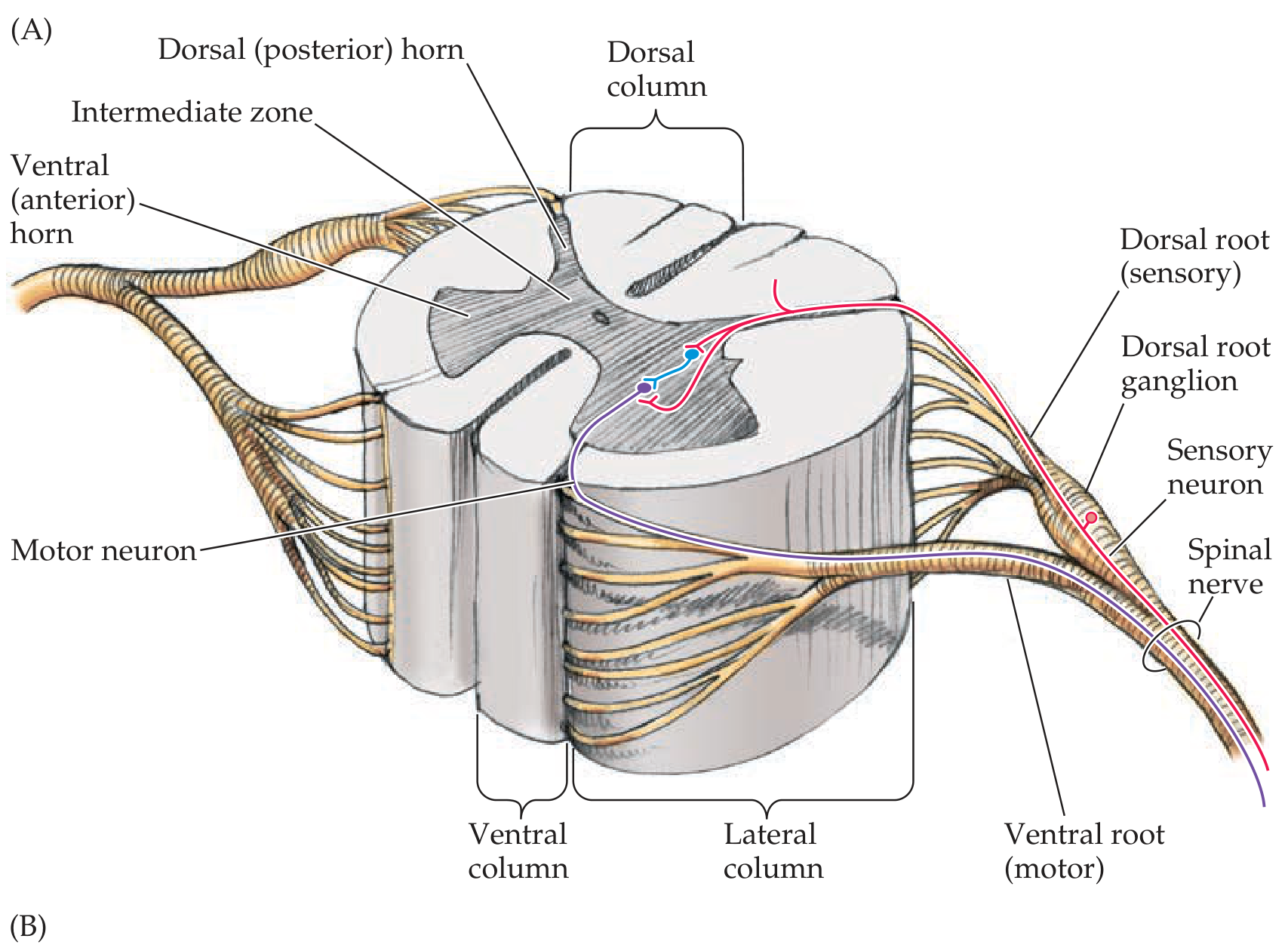
Basic spinal cord anatomy showing gray matter, white matter, dorsal and ventral roots - Neuroanatomy through Clinical Cases, 3rd Ed.
A. Gray Matter (H- or butterfly-shaped)
The gray matter has a characteristic "H" shape with two lateral columns joined by a gray commissure. It contains:
Dorsal (posterior) horn - primarily sensory processing
Ventral (anterior) horn - contains lower motor neurons (LMNs); more prominent at cervical and lumbosacral enlargements
Intermediate zone - interneurons and specialized nuclei
Intermediolateral (IML) column - T1 to L2 only; preganglionic sympathetic neurons
Sacral parasympathetic nucleus - S2-S4; preganglionic parasympathetic neurons
Rexed's Laminae (10 laminae):
| Laminae | Region | Function |
|---|---|---|
| I | Dorsal horn (marginal zone) | Pain & temperature |
| II | Dorsal horn (substantia gelatinosa) | Pain modulation |
| III-IV | Dorsal horn (nucleus proprius) | Touch, proprioception relay |
| V | Dorsal horn | Wide dynamic range neurons |
| VI | Dorsal horn (base) | Proprioceptive input |
| VII | Intermediate zone | Clarke's column (T1-L2), IML, interneurons |
| VIII-IX | Ventral horn | Motor interneurons, alpha/gamma LMNs |
| X | Around central canal | Gray commissure |
B. White Matter (surrounds gray matter)
Three funiculi (columns) on each side:
Dorsal (posterior) funiculus - between posterior horns; carries the dorsal column medial lemniscal system
- Fasciculus gracilis (medial): from lower body (below T6) - fine touch, vibration, proprioception
- Fasciculus cuneatus (lateral): from upper body (above T6) - same modalities; only present at cervical levels
Lateral funiculus - between dorsal and ventral horns; contains:
- Lateral corticospinal tract (descending, main motor pathway - 85%)
- Rubrospinal tract (descending)
- Lateral spinothalamic tract (ascending - pain, temperature)
- Dorsal and ventral spinocerebellar tracts
Ventral (anterior) funiculus - between ventral horns and anterior median fissure; contains:
- Anterior corticospinal tract (descending - 15%)
- Vestibulospinal, tectospinal, reticulospinal tracts (descending)
- Anterior spinothalamic tract (crude touch, pressure)
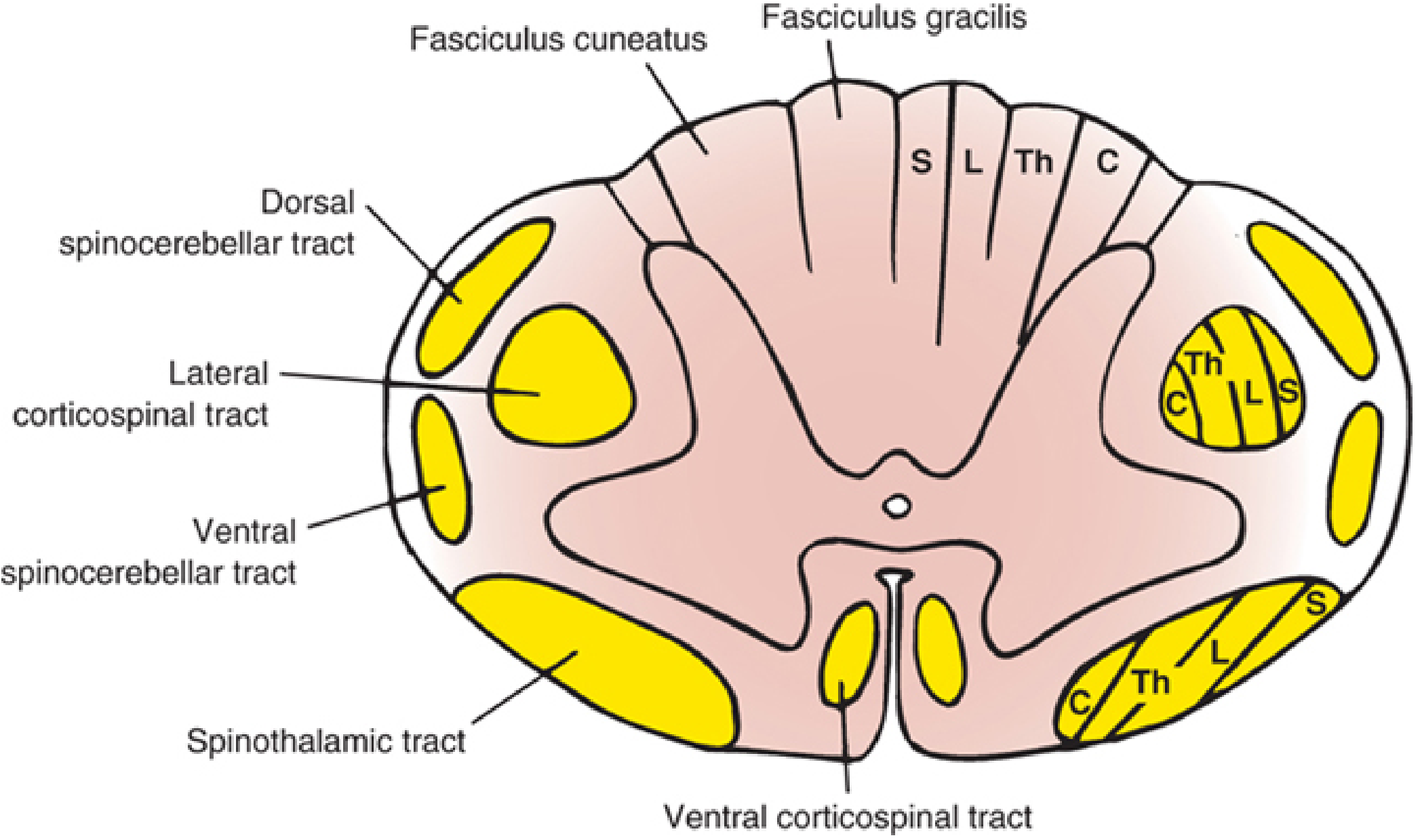
Tract lamination: fibers in the dorsal columns and spinothalamic tracts are arranged somatotopically - sacral most lateral, cervical most medial/anterior. This explains clinical differences between central cord syndrome (affects cervical fibers first) and peripheral cord lesions - Localization in Clinical Neurology, 8e.
5. Variation by Level
| Level | White Matter | Gray Matter | Notable |
|---|---|---|---|
| Cervical | Most abundant (all ascending fibers present, most descending not yet terminated) | Enlarged ventral horn | Fasciculus cuneatus present |
| Thoracic | Moderate | Relatively small | IML column present |
| Lumbar | Less | Large (especially ventral horn) | No IML |
| Sacral | Least | Mostly gray | Parasympathetic nucleus |
6. Blood Supply of the Spinal Cord
The spinal cord has both an extrinsic and an intrinsic vascular network.
A. The Three Longitudinal Arteries
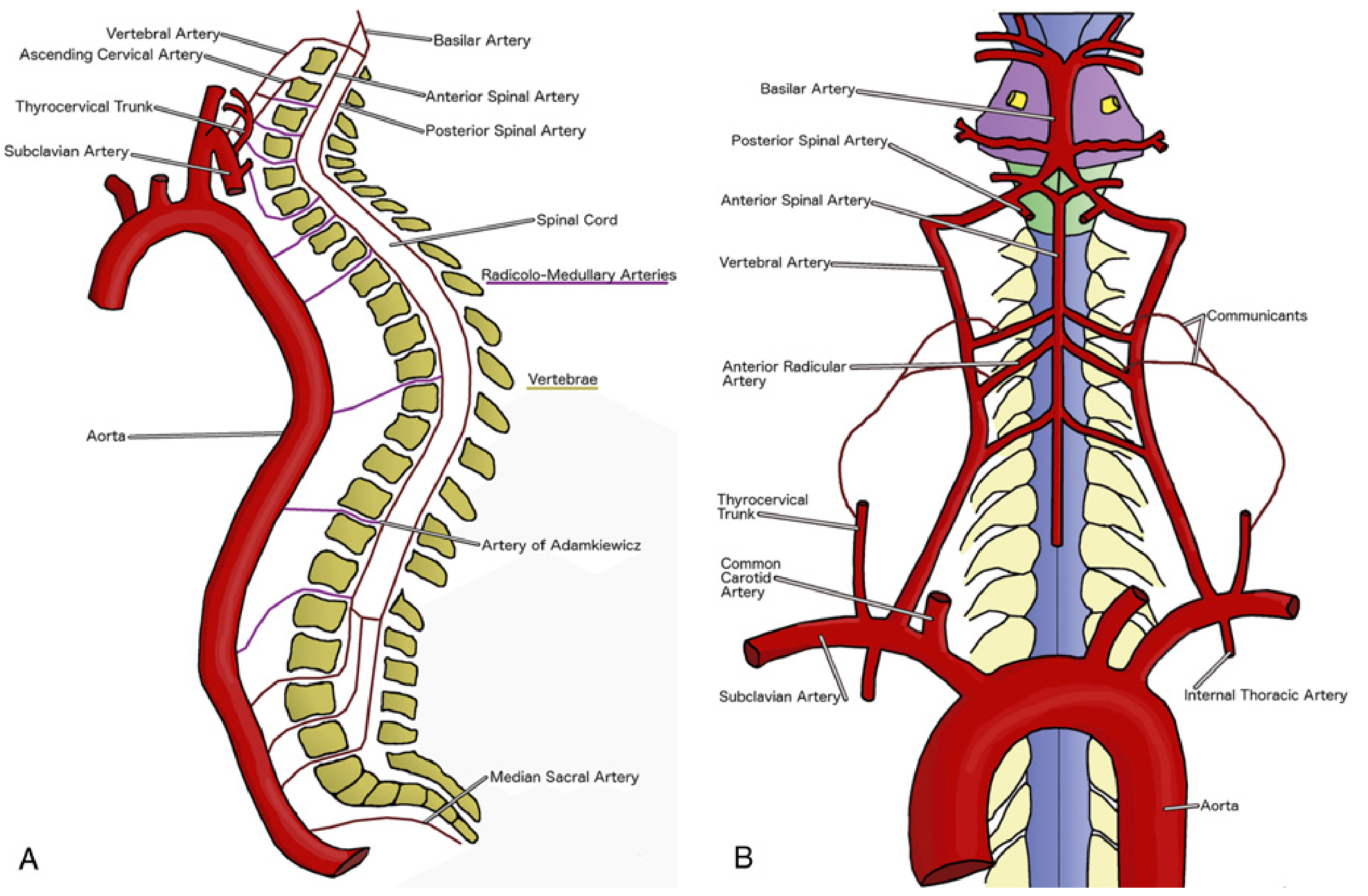
Complete overview of spinal cord arterial supply showing the anterior spinal artery, posterior spinal arteries, radiculomedullary arteries, and the artery of Adamkiewicz - Miller's Anesthesia, 10e.
1. Anterior Spinal Artery (ASA) - Single
- Formed by fusion of two branches from the terminal vertebral arteries at the cervicomedullary junction
- Runs the entire length of the cord in the anterior median fissure
- Supplies the anterior 2/3 of the cord via:
- Sulco-commissural (central) arteries - penetrate deeply to supply anterior gray columns, lateral gray columns, and ventral white matter
- Pial radial network - supplies peripheral rim of the anterior white matter
2. Posterior Spinal Arteries (PSA) - Paired
- Arise from the vertebral arteries or posterior inferior cerebellar arteries (PICA)
- Run bilaterally along the posterolateral surfaces of the cord
- Supply the posterior 1/3 of the cord - the dorsal columns and dorsal horns
- Form a rich anastomotic spinal arterial plexus around the cord (the vasocorona)
- Relatively protected from ischemia because of the dual supply (two PSAs vs one ASA)
B. Radiculomedullary (Segmental) Arteries - Extrinsic Input
The longitudinal spinal arteries are reinforced along their length by radiculomedullary arteries that enter through the intervertebral foramina alongside nerve roots. Of the 31 segmental arteries, only 6-10 are true radiculomedullary arteries that actually reach the cord.
Lazorthes divided these into three groups:
| Group | Level | Source |
|---|---|---|
| Upper (cervicothoracic) | C1-T2 | Vertebral, ascending cervical, thyrocervical, and costovertebral arteries |
| Middle (thoracic) | T3-T8 | Usually a single T7 radicular artery from aorta |
| Lower (thoracolumbar) | T9-L2 | Artery of Adamkiewicz |
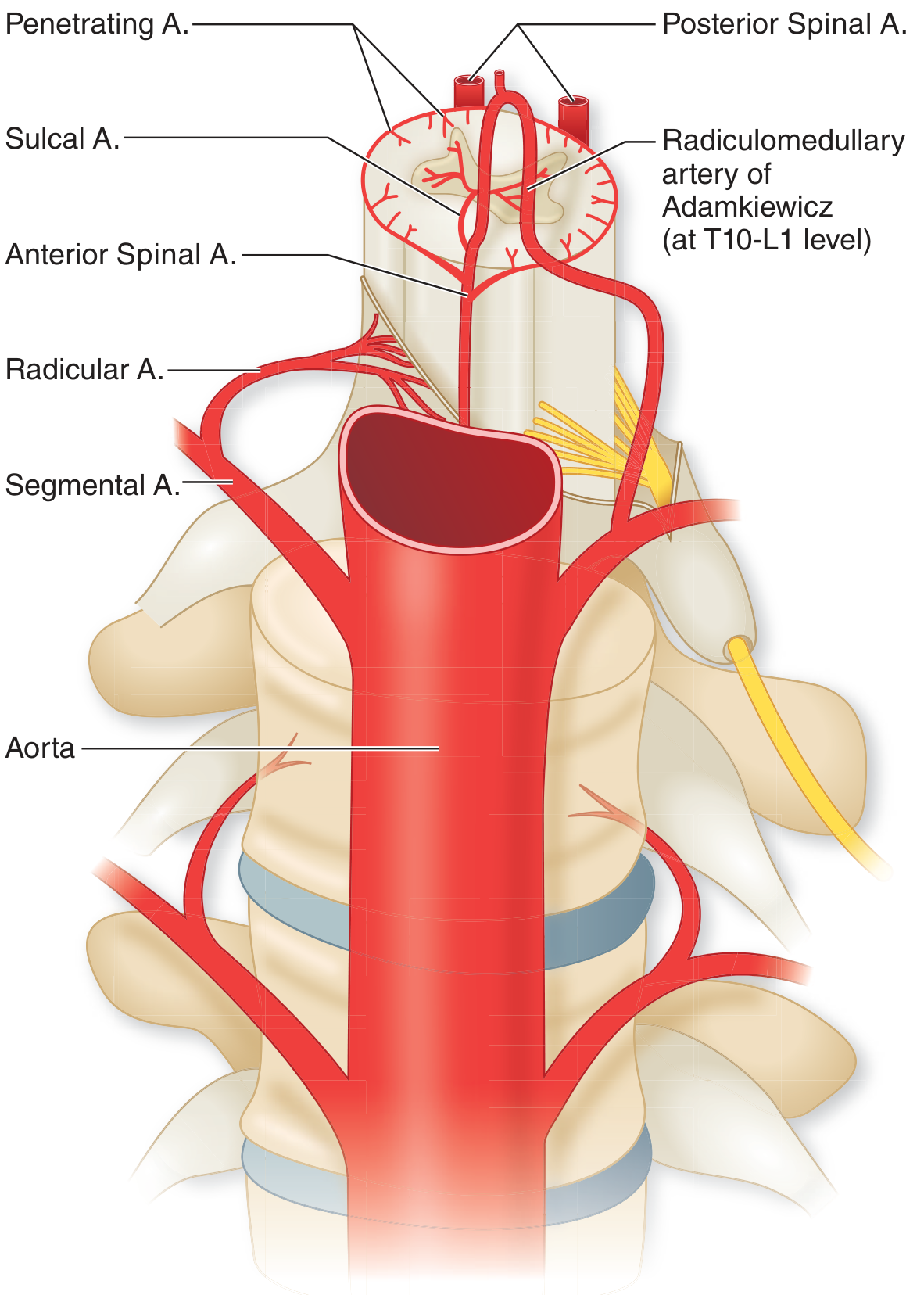
Detailed view of segmental arterial supply - note the artery of Adamkiewicz entering at T10-L1 and joining the anterior spinal artery - Adams & Victor's Principles of Neurology, 12e.
C. Artery of Adamkiewicz (Arteria Radicularis Magna)
- The largest and most important anterior radiculomedullary artery
- Supplies the lower 2/3 of the anterior spinal artery territory (including the lumbosacral enlargement)
- Origin: typically from a left posterior intercostal artery arising from the descending aorta, usually between T9 and T12 (range: T7-L5)
- Its characteristic hairpin configuration on angiography/imaging is pathognomonic
- Because it is the sole major supply to the lower thoracic cord, this region is a watershed zone highly susceptible to ischemia during aortic surgery or hypotension
D. Additional Sources by Region
| Region | Arterial Source |
|---|---|
| Cervical cord | Vertebral arteries, ascending cervical and deep cervical (thyrocervical trunk) |
| Thoracic cord | Segmental posterior intercostal arteries from aorta |
| Lumbar cord | Lumbar segmental arteries from aorta |
| Sacral cord | Median sacral artery, lateral sacral arteries (internal iliac) |
E. Intrinsic Cord Vessels (Cross-section)
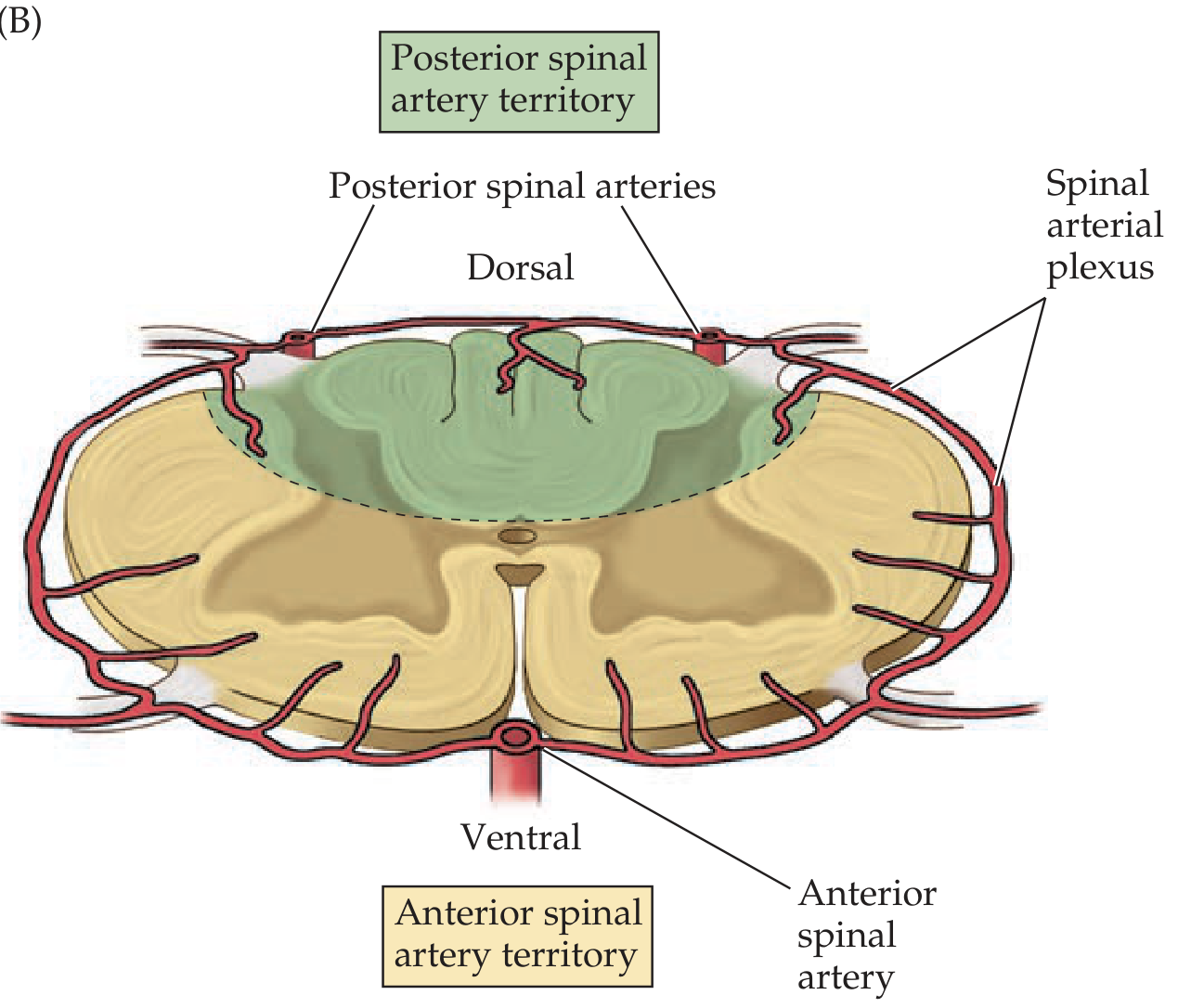
Cross-sectional vascular territories: the ASA supplies the anterior 2/3 (yellow-tan); the PSAs supply the dorsal third (green). The peripheral rim is supplied by the pial arterial plexus (vasocorona) - Neuroanatomy through Clinical Cases, 3rd Ed.
7. Venous Drainage
- Six longitudinal venous channels run the cord's length (anterior and posterior median veins, anterolateral and posterolateral veins)
- These drain via anterior and posterior radicular veins into the internal vertebral venous plexus (Batson's plexus) in the epidural space
- From there, drainage proceeds to the external vertebral plexus and then into the azygos/hemiazygos system, iliac veins, and inferior vena cava
8. Clinical Correlations
| Vascular Syndrome | Artery | Cord Region Affected | Clinical Features |
|---|---|---|---|
| Anterior spinal artery syndrome | ASA | Anterior 2/3 (spinothalamic + corticospinal + anterior horn) | Bilateral weakness, loss of pain/temperature; preserved vibration/proprioception (dorsal columns spared) |
| Posterior spinal artery syndrome | PSA | Posterior 1/3 (dorsal columns) | Loss of vibration, proprioception, fine touch; weakness may occur |
| Adamkiewicz occlusion | Artery of Adamkiewicz | Lower thoracic/lumbar cord | Paraplegia with anterior cord syndrome; common in aortic surgery |
| Watershed infarction | T3-T8 | Mid-thoracic cord (least collateral flow) | Paraplegia; most common location of spinal cord infarct |
Sources:
- Campbell's Operative Orthopaedics, 15th Ed. (2026), p. 2225
- Neuroanatomy through Clinical Cases, 3rd Ed., pp. 250-253
- Adams and Victor's Principles of Neurology, 12th Ed., p. 658-666
- Localization in Clinical Neurology, 8th Ed., pp. 242-243
- Miller's Anesthesia, 10th Ed., pp. 8015-8017
- Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.