Neisseria gonococcus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Neisseria gonorrhoeae"[MeSH Terms] AND "gonorrhea"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple textbooks. Let me compile the full answer.
Neisseria gonorrhoeae (The Gonococcus)
Classification and Basic Microbiology
Neisseria gonorrhoeae (the gonococcus) is a Gram-negative diplococcus - pairs of kidney/coffee-bean-shaped cocci (~0.6-1.0 µm diameter) with adjacent sides flattened. It is:
- Obligate aerobe, oxidase-positive, catalase-positive
- Fastidious - requires enriched media (chocolate agar, Thayer-Martin, Martin-Lewis) plus 5-10% CO2 at 35-37°C in a humid atmosphere
- Produces acid from glucose only (not maltose, lactose, or sucrose) - key biochemical distinguishing feature from N. meningitidis (which also ferments maltose)
- More fragile than N. meningitidis; lacks a polysaccharide capsule
- Small, smooth, non-pigmented colonies appear in 18-24 hours; well-developed (2-4 mm) by 48 hours
Virulence Factors
| Factor | Function |
|---|---|
| Type IV Pili | Initial attachment to non-ciliated epithelial cells; "twitching" motility via contraction; facilitate transformation (DNA uptake); facilitate movement up fallopian tubes |
| Opa proteins (opacity proteins) | Tight secondary adherence to host receptors (CD66, integrins); mediate gonococcus-to-gonococcus clumping; expressed in opaque colonies |
| Por proteins (Porins: Por1BA, Por1BB) | Insert into host cell membrane; trigger signaling cascades leading to intracellular uptake (parasite-directed endocytosis) |
| Rmp protein | Reduces bactericidal antibody activity |
| LOS (Lipooligosaccharide) | Endotoxin activity; triggers inflammation; sialylation of LOS binds factor H to block complement C3b deposition |
| IgA1 protease | Cleaves secretory IgA, evading mucosal immunity |
| β-lactamase | Confers penicillin resistance (PPNG strains) |
| Iron receptors | Transferrin, lactoferrin, hemoglobin receptors allow iron scavenging from host |
| Catalase / antioxidant systems | Resist oxidative killing inside neutrophils |
Antigenic variation of pili and Opa proteins (via phase variation and gene rearrangement) is a major immune evasion strategy and the reason lasting protective immunity does not develop after infection.
Pathogenesis
Step 1 - Attachment: Gonococci introduced onto a mucosal surface attach via pili to receptors (CD46, CD66) on non-ciliated columnar epithelial cells. Pili-driven twitching motility moves microcolonies across the cell surface.
Step 2 - Tight binding and invasion: Opa proteins mediate tighter attachment, and porin proteins (Por1BA) trigger signaling cascades that induce parasite-directed phagocytosis (endocytosis by the host cell using microfilaments and microtubules). The bacteria transcytose through the cell and exit through the basal membrane into the submucosa.
Step 3 - Survival in submucosa: Despite lacking a capsule, gonococci survive via:
- LOS sialylation (blocks C3b deposition by binding factor H)
- Pili and Opa proteins interfering with effective phagocytosis
- Upregulation of catalase (resists oxidative burst inside PMNs)
Step 4 - Spread: Purulent exudate with "sticky" Opa-mediated gonococcal clusters spreads to adjacent structures: epididymis and prostate (men); paracervical glands, fallopian tubes (women). LOS and peptidoglycan shedding cause epithelial injury and intense inflammation.
Note: Gonococci infect columnar/transitional epithelium only - they cannot infect the squamous epithelium lining the vagina of post-pubescent women (hence cervical columnar epithelium is the primary site in women).
Epidemiology
- Humans are the only natural host
- Transmission is exclusively by direct sexual contact (or vertical at birth)
- ~78 million new cases worldwide annually; ~555,608 cases reported in the US in 2017 (true incidence likely double)
- Highest rates: ages 15-24, Black Americans, residents of southeastern US, individuals with multiple sexual partners
- Asymptomatic carriage is common in women (~50%), driving unrecognized transmission
- Complement deficiency (late components C5-C9) is a risk factor for disseminated gonococcal infection (DGI)
Clinical Diseases
1. Uncomplicated Gonorrhea
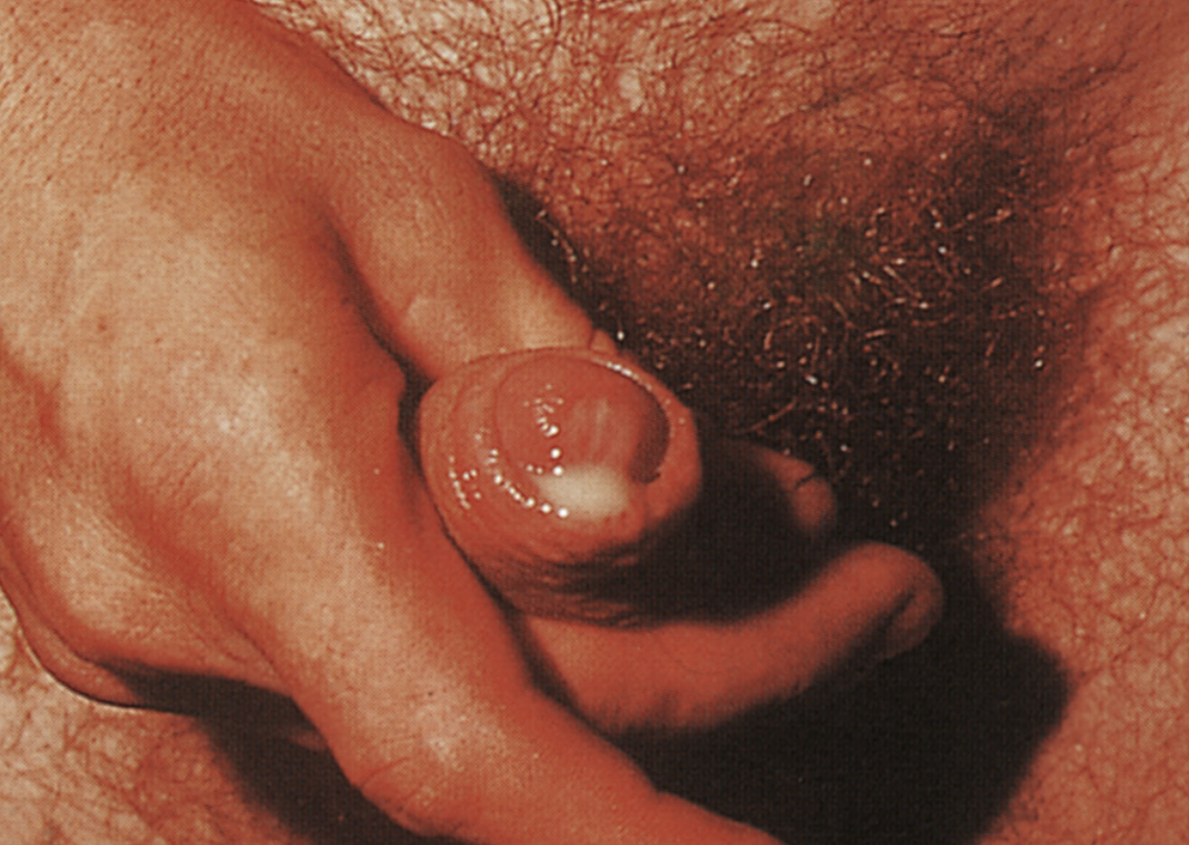
Men:
- Urethritis: purulent urethral discharge + dysuria after a 2-5 day incubation period
- Virtually all infected men are symptomatic
- Complications: epididymitis, prostatitis, periurethral abscesses
Women:
- Primary site: endocervix (columnar epithelium)
- Symptoms: vaginal discharge, dysuria, abdominal pain - but often asymptomatic
- Complications: PID (10-20%), salpingitis, tubo-ovarian abscess, ectopic pregnancy, infertility
Other sites (by sexual practice):
- Proctitis (rectal gonorrhea)
- Pharyngeal gonorrhea (often asymptomatic)
- Conjunctivitis in adults (from autoinoculation)
2. Pelvic Inflammatory Disease (PID)
Ascending infection in women involving fallopian tubes (salpingitis). Presents with fever, lower abdominal pain, cervical motion tenderness. Long-term consequences: sterility, ectopic pregnancy, chronic pelvic pain.
3. Disseminated Gonococcal Infection (DGI) - "Gonococcemia"
Occurs in 1-3% of infected women, less often in men (due to high rate of asymptomatic women with untreated infection).
Classic triad:
- Fever + migratory arthralgias/polyarthritis
- Suppurative (septic) arthritis - wrists, knees, ankles most common
- Pustular rash on an erythematous base over extremities (not palms/soles)
Blood cultures are often negative in DGI even though bacteremia is present - cervical cultures are more revealing.
4. Ophthalmia Neonatorum
Purulent conjunctivitis in newborns acquired during passage through an infected birth canal. Can lead to blindness if untreated. Prophylaxis: 1% silver nitrate drops (or erythromycin ointment) at birth.
Diagnosis
| Method | Notes |
|---|---|
| Gram stain | Gram-negative diplococci inside PMNs. >95% sensitive and specific in symptomatic men only. Only 50-70% sensitive in women. Acceptable as sole diagnostic in symptomatic men. |
| Culture | Selective media (Martin-Lewis, modified Thayer-Martin, NYC agar) - chocolate agar + antibiotics (vancomycin, colistin, trimethoprim, nystatin) to inhibit competing flora. Oxidase-positive colonies confirmed by glucose oxidation. |
| NAAT (Nucleic Acid Amplification Tests) | Now the diagnostic gold standard. More sensitive than culture. Can be performed on urine, genital swabs. Often combined with Chlamydia detection (same target population). Results are diagnostic from genital sites; may need culture confirmation from non-genital sites. |
Treatment
Resistance evolution:
- Penicillin: no longer used - widespread β-lactamase (PPNG) and chromosomally mediated resistance
- Fluoroquinolones (ciprofloxacin): widespread resistance, no longer recommended
- Azithromycin: high-level resistance emerging; dropped from standard regimens after ~2020
Current standard (as of updated guidelines):
- Ceftriaxone 500 mg IM single dose (or 1g if weight ≥150 kg) - third-generation cephalosporin resistant to prevalent β-lactamases
- Concurrent treatment for Chlamydia is recommended for all patients treated for gonorrhea (doxycycline 100 mg PO BID x 7 days if chlamydia not excluded)
- High-level cephalosporin resistance has been reported (XDR gonorrhea - a WHO priority pathogen)
Ophthalmia neonatorum: Ceftriaxone IV/IM
Prevention and Control
- Condoms provide high-degree protection against acquisition and transmission
- Spermicides/douches are not reliable protection
- Case-contact tracing and partner notification
- No effective vaccine available; antigenic variation of pili and OMPs makes vaccine development challenging
- MenB-4C vaccine (meningococcal B vaccine) has shown cross-protective efficacy against gonorrhea in recent studies - a promising 2024-2025 development (PMID: 39082700)
Comparison: N. gonorrhoeae vs. N. meningitidis
| Feature | N. gonorrhoeae | N. meningitidis |
|---|---|---|
| Capsule | No | Yes |
| Maltose fermentation | No | Yes |
| Disease | Gonorrhea, DGI, PID | Meningitis, meningococcemia |
| Transmission | Sexual contact | Respiratory droplets |
| Carrier state | Common (asymptomatic women) | Nasopharyngeal carriage |
| Vaccine | None effective | Available (serogroups A, C, W, Y, B) |
| Growth on selective media | Yes (Thayer-Martin, NYC) | Yes |
Sources: Medical Microbiology 9e (Murray); Sherris & Ryan's Medical Microbiology 8e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e
Recent evidence update: A 2025 systematic review (PMID 39082700) confirmed the MenB-4C vaccine (4CMenB/Bexsero) offers meaningful cross-protective efficacy against gonorrhea - an important development given the absence of a dedicated gonococcal vaccine and rising antimicrobial resistance.
This is a shared conversation. Sign in to Orris to start your own chat.