A pt ckd on mhd from 1 year came after days gap for dialysis today ,was sent for avf surgery,after initiating hd resulting in low oxygen High pulse 150 and high bp recomend medicine and precautions
Acute Management: CKD Patient on MHD - Post-AVF Surgery Presenting with Hypoxia, Tachycardia (HR 150), and Hypertension After Missed Dialysis Sessions
Clinical Picture
- Low SpO2 = pulmonary edema from volume overload
- HR 150 = compensatory sinus tachycardia (or possibly AF/flutter - must check ECG)
- High BP = volume-dependent hypertension in ESRD
STEP 1 - Immediate Priorities (Do Simultaneously)
| Action | Rationale |
|---|---|
| Sit the patient upright | Reduces venous return, decreases pulmonary congestion |
| O2 supplementation - target SpO2 ≥94% | Start with high-flow mask; if worsening, escalate to BiPAP/NIV |
| 12-lead ECG immediately | Differentiate sinus tachycardia vs AF/flutter vs VT; missed dialysis causes hyperkalemia which causes arrhythmia |
| Serum K+, BMP, ABG | Hyperkalemia is the silent killer - must be ruled out/treated before medications |
| Chest X-ray | Confirm pulmonary edema, rule out effusion |
| Bedside echo/US | Rule out cardiac tamponade (common in ESRD, presents with tachycardia + dyspnea) |
STEP 2 - Medications
A. For Pulmonary Edema / Volume Overload
- Dose: Start IV NTG at 5-10 mcg/min, titrate up by 5 mcg/min every 3-5 min to reduce BP
- Acts as a venodilator reducing preload rapidly
- Also has coronary vasodilatory benefit if ACS is a trigger
- Rosen's Emergency Medicine recommends this as a cornerstone of therapy
- Dose: 60-100 mg IV
- Use even in anuric/oligouric ESRD - furosemide has short-lived vasodilatory action beyond diuresis
- Per Tintinalli: "Loop diuretics may aid even in those with minimal urine output because loop diuretics have short-lived vasodilatory actions"
- Doubles up as preload reducer
- If SpO2 not improving on high-flow O2, start BiPAP (IPAP 12-14, EPAP 5-8)
- Reduces work of breathing, improves oxygenation, decreases preload
- Avoids intubation in most cases
B. For Tachycardia (HR 150)
- If sinus tachycardia secondary to hypoxia/pain/anxiety: treat the cause (O2, fluid removal) - rate will come down
- If AF with rapid ventricular rate: rate control needed
- If AF: IV Metoprolol (2.5-5 mg IV, repeat every 5 min, max 15 mg) or IV Diltiazem (0.25 mg/kg IV over 2 min)
- Caution: avoid negative inotropes if LV function is poor (check echo first)
- If hyperkalemia-related arrhythmia: IV Calcium gluconate 10 mL of 10% stat (cardiac membrane stabilization)
C. For Hypertension
- 20 mg IV bolus, can repeat 40-80 mg every 10 min
- Good for ESRD - not renally cleared significantly
- Handles both tachycardia and hypertension
- 10-20 mg IV slowly
- Safe in renal failure
- Reduces afterload
- Long-acting calcium channel blockers are effective for volume-dependent hypertension
Avoid: ACE inhibitors/ARBs IV acutely if K+ unknown (risk of worsening hyperkalemia). Oral ACEI can be continued if already on it, but do not start fresh acutely until K+ confirmed safe.
STEP 3 - Definitive Treatment: Emergency Hemodialysis
"The most common problem requiring emergent dialysis, particularly in the patient with CKD, is pulmonary edema secondary to volume overload...Despite the effectiveness of temporizing measures, many of these patients require immediate dialysis."
- Set ultrafiltration target carefully - do NOT remove fluid too rapidly (risk of dialysis hypotension)
- Lower blood flow rate initially given tachycardia and hemodynamic instability
- Consider sodium profiling and cooling dialysate to improve hemodynamic tolerance
- Monitor BP, HR, SpO2 every 15-30 minutes throughout
STEP 4 - Post-AVF Surgery Precautions (Critical)
- Do NOT use the new AVF arm for BP measurement - this is a hard rule. Use the contralateral arm.
- Do NOT apply tourniquet or compression to the AVF arm.
- Do NOT draw blood or place IV lines in the AVF arm unless absolutely no other option exists.
- Check the AVF for thrill and bruit before and after dialysis - a lost thrill signals thrombosis.
- The new AVF will NOT be mature - access for this emergency dialysis session will be via whatever existing access was used before (tunneled catheter or previous access site).
- Protect the surgical site from bleeding, especially if anticoagulation (heparin) is used during dialysis - consider using minimal heparin or heparin-free dialysis (citrate anticoagulation or saline flushes).
- Watch for high-output cardiac failure from the newly created AVF - this itself can worsen tachycardia and cardiac demand.
STEP 5 - Watch for and Treat Hyperkalemia
| Drug | Dose | Action |
|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 2-3 min | Cardiac membrane stabilization (immediate) |
| Insulin 10 units + 50% Dextrose 50 mL IV | Push | Shifts K into cells (15-30 min) |
| Sodium bicarbonate | 50-100 mEq IV | Shifts K into cells (in metabolic acidosis) |
| Kayexalate (Sodium polystyrene sulfonate) | 15-30g oral | Eliminates K via gut (hours) |
| Dialysis | - | Definitive K removal |
Summary Algorithm
Low SpO2 + HR 150 + High BP in MHD post-AVF
↓
Sit upright → O2 → ECG → K+ → Echo
↓
Treat hyperkalemia if present (Ca gluconate, insulin-dextrose)
+
IV NTG / Furosemide 80-100mg IV for preload reduction
+
BiPAP if SpO2 not improving
+
IV Labetalol for BP + HR (if ECG confirms sinus tach or AF RVR)
↓
Initiate emergency HD - SLOW ultrafiltration
(Use existing catheter access, NOT new AVF)
+
Protect AVF arm at all times
Monitor thrill/bruit before and after
Note: This patient needs immediate nephrologist involvement and likely cardiac monitoring in a step-down or ICU-level setting given post-surgical status and hemodynamic compromise. If tachycardia persists despite treating hypoxia and volume, a formal cardiological evaluation is warranted.
Create a clinical decision tree poster for managing missed-dialysis emergencies
Clinical decision tree poster for managing missed-dialysis emergencies in CKD/ESRD patients on maintenance hemodialysis. Medical infographic style with clean white background and professional healthcare design. Title at top: "MISSED DIALYSIS EMERGENCY MANAGEMENT" with subtitle "CKD Patient on Maintenance Hemodialysis (MHD)". Decision tree flowchart with the following structure and color-coded boxes: TOP BOX (red alert): "MISSED DIALYSIS SESSIONS - Patient Presents with Symptoms" Three symptom branches below in orange boxes: - Branch 1: "LOW SpO2 / Hypoxia" (pulmonary edema) - Branch 2: "TACHYCARDIA HR >100" (compensatory / arrhythmia) - Branch 3: "HIGH BP / Hypertension" (volume-dependent) IMMEDIATE ACTIONS box (dark blue, centered): "SIMULTANEOUS IMMEDIATE ACTIONS: ✓ Sit patient upright ✓ High-flow O2 - target SpO2 ≥94% ✓ 12-lead ECG stat ✓ Serum K+, BMP, ABG, CXR ✓ Bedside Echo - rule out tamponade" Decision diamond (yellow): "HYPERKALEMIA? K+ >6.5 or ECG changes?" YES branch (red box): "TREAT HYPERKALEMIA FIRST: • Calcium Gluconate 10% - 10mL IV (cardiac stabilization) • Insulin 10U + Dextrose 50mL IV (shift K+ into cells) • Sodium Bicarbonate 50mEq IV • Kayexalate 15-30g oral" NO branch continues to: PHARMACOTHERAPY box (green): "MEDICATIONS: • IV Nitroglycerin 5-10mcg/min (preload ↓, BP ↓) • IV Furosemide 80-100mg (vasodilation + diuresis) • IV Labetalol 20mg (HR control + BP) • BiPAP if SpO2 not improving on O2" Decision diamond (yellow): "SpO2 IMPROVING?" NO branch: "ESCALATE: BiPAP → Intubation if needed" YES branch continues to: DEFINITIVE TREATMENT box (purple, large): "EMERGENCY HEMODIALYSIS • Initiate ultrafiltration - remove excess fluid SLOWLY • Use existing catheter (NOT new AVF) • Lower blood flow rate initially • Sodium profiling + cool dialysate • Monitor BP, HR, SpO2 every 15 min" POST-AVF SURGERY PRECAUTIONS box (red border, bottom left): "⚠ AVF ARM PRECAUTIONS: ✗ NO BP measurement on AVF arm ✗ NO tourniquet or compression ✗ NO blood draw or IV lines ✓ Check thrill & bruit before/after dialysis ✓ Minimal heparin anticoagulation ✓ Watch for high-output cardiac failure" MONITORING box (bottom right, teal): "ONGOING MONITORING: • Vitals every 15-30 min during HD • Repeat K+ after 1hr of dialysis • Fluid balance chart • Involve Nephrologist + Cardiologist" Color scheme: Red for alerts, blue for actions, green for medications, purple for dialysis, yellow for decisions, teal for monitoring. Clean medical font, icons/symbols for each section. Professional clinical poster layout.
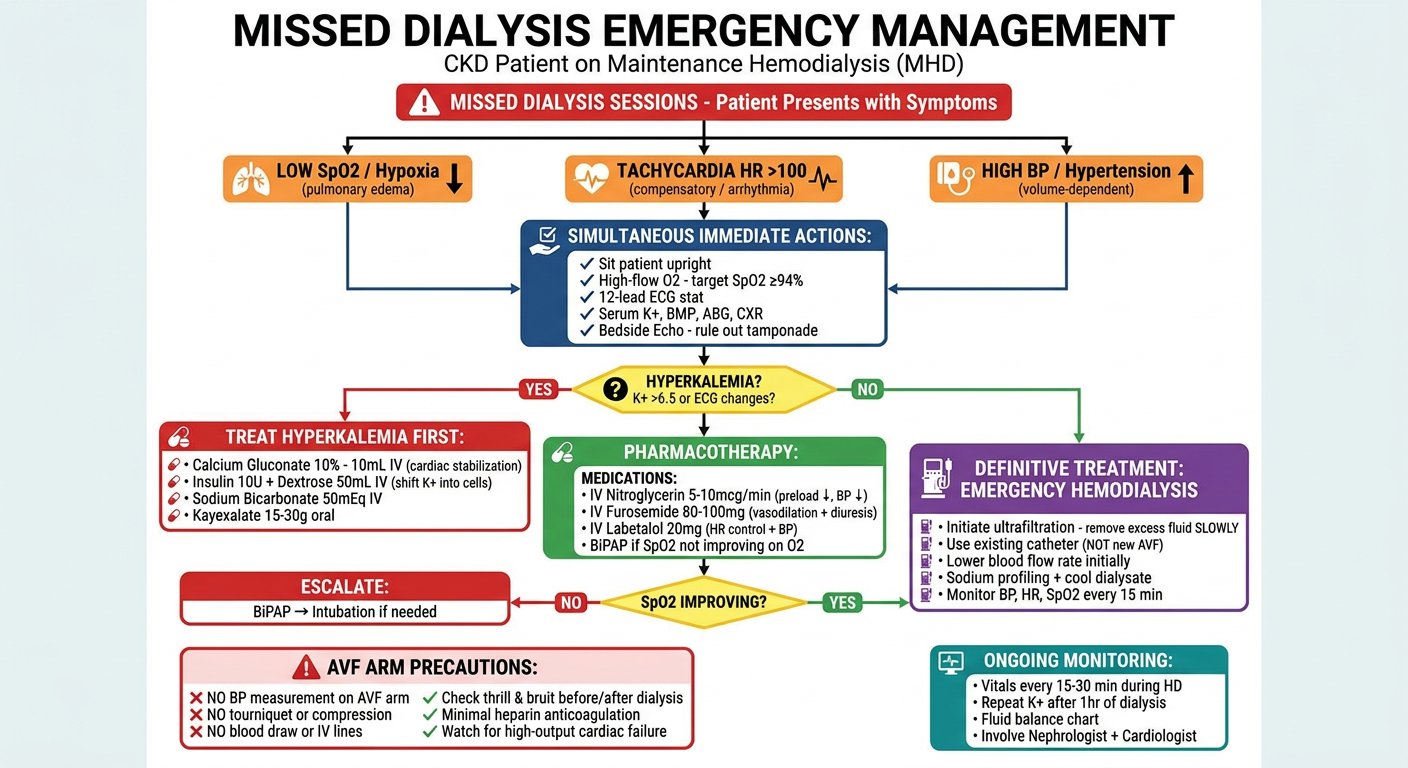
- Red alert at the top for missed dialysis presentation
- Three presenting symptom branches - hypoxia, tachycardia, hypertension
- Immediate simultaneous actions (ECG, O2, labs, echo)
- Hyperkalemia decision point with treatment protocol
- Pharmacotherapy - IV nitrates, furosemide, labetalol, BiPAP
- Emergency HD as definitive treatment with dialysis parameters
- AVF arm precautions (critical for your post-surgical patient)
- Ongoing monitoring reminders