Ear pus and pain and itching
Reading File
Finding Sources
Finding Sources
Searching PubMed
otitis externa treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive clinical overview of ear pus, pain, and itching:
Ear Pus (Otorrhea) + Pain (Otalgia) + Itching (Pruritus)
The triad of ear discharge, pain, and itching points to otitis externa (OE) as the most common diagnosis, though otitis media with perforation must also be considered. Here is a structured breakdown:
Types of Otitis Externa
The combination of these three symptoms fits the spectrum of otitis externa, which affects up to 10% of all persons during their lifetimes.
| Type | Key Features | Common Pathogen |
|---|---|---|
| Acute Diffuse OE (Swimmer's Ear) | Severe otalgia, itching, purulent discharge, hearing loss | Pseudomonas aeruginosa (most common) |
| Acute Localized OE | Itching, pain, swelling, small pustule/furuncle in canal | Staphylococcus aureus |
| Fungal OE (Otomycosis) | Intense itching, clear/white discharge, "cotton-like" debris, hyphae visible | Aspergillus, Candida |
| Chronic OE | Mild discomfort, flaking, itching, prolonged course | Mixed bacteria + fungi |
| Eczematous OE | Severe itching, scaling, crusting, oozing | Contact/seborrhoeic/atopic dermatitis |
| Malignant (Necrotizing) OE | Progressive pain unresponsive to drops, granulation tissue, cranial nerve palsies | P. aeruginosa (in diabetics, immunocompromised) |
- Cummings Otolaryngology Head and Neck Surgery; Textbook of Family Medicine 9e
Pathophysiology
The external auditory canal (EAC) normally has a slightly acidic pH and a self-cleaning mechanism. Disruption of these defenses leads to infection:
- Moisture (swimming, sweating) raises the canal pH and softens skin
- Trauma (cotton buds, hearing aids, earphones) disrupts the skin barrier
- Predisposing skin conditions: eczema, seborrhoea, psoriasis
- Narrow canal (congenital, exostoses) traps moisture
In acute bacterial OE: early infection causes pruritus and erythema with clear discharge; as it worsens, discharge becomes seropurulent, canal swells, and pain intensifies. Pain is characteristically worsened by pulling the pinna or pressing the tragus.
Microbiology
- Bacterial infections: >90% of acute cases
- Most common organisms: P. aeruginosa > S. epidermidis > S. aureus
- Fungal OE (Aspergillus, Candida): <2% of acute cases, but more likely after antibiotic treatment
- Fungal infection shows "wet newspaper" appearance with Aspergillus (white plug + black dots)
Clinical Images
Chronic otitis externa - showing atrophy and stenosis of canal skin:

Otomycosis (Aspergillus flavus) - florid fungal infection with tufts of fungus and white conidiophores:
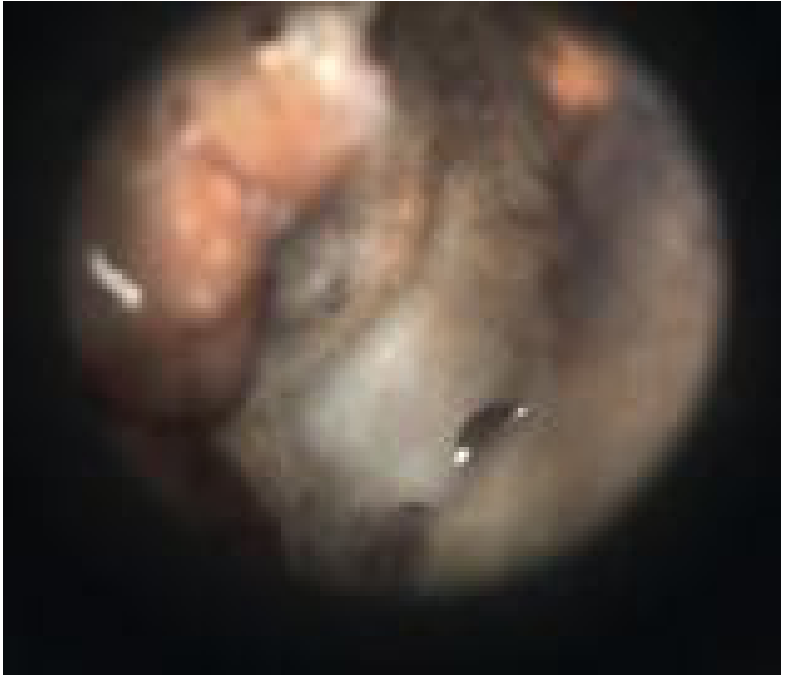
- Cummings Otolaryngology Head and Neck Surgery
Management
General / Preventive
- Occlusive earplugs during swimming
- Stop cotton-tipped applicators - they cause trauma and worsen inflammation
- Keep ears dry; hair dryer on low setting can help
Acute Bacterial OE - First Line
- Topical antibiotic + steroid drops are the treatment of choice
- Fluoroquinolone drops (e.g., ciprofloxacin/ofloxacin): preferred, safe even if TM perforation suspected
- Aminoglycosides (e.g., neomycin/gentamicin): effective but ototoxic - avoid if TM may be perforated; also risk of contact hypersensitivity
- Addition of a corticosteroid to topical antibiotics improves symptoms
- Acetic acid (50% diluted) irrigation can be effective in early/mild AOE
- Debridement of the canal is an important adjunct - removes debris, improves penetration of drops
- If canal is too swollen for drops to penetrate: insert a wick (Merocel sponge or cotton strand)
Systemic Antibiotics
- NOT indicated in immunocompetent patients with uncomplicated OE
- Reserved for: cellulitis extending to the pinna, or immunocompromised patients
Fungal OE (Otomycosis)
- Stop antibiotic drops (they promote fungal overgrowth)
- Meticulous cleaning and debridement
- Antifungal drops (clotrimazole, acetic acid)
- A recent 2026 meta-analysis (PMID: 41373129) reviewed RCTs on otomycosis management and supports this approach
Chronic OE
- Treat the underlying dermatitis
- Remove inciting factors (shampoos, hearing aid molds, ear buds)
- Topical steroids to reduce inflammation
- Meticulous cleaning under microscopy in clinic
- Rosen's Emergency Medicine; Bailey and Love's Surgery 28e; Cummings Otolaryngology
Red Flags - When to Refer Urgently
| Red Flag | Concern |
|---|---|
| Diabetic or immunocompromised patient with persistent OE not responding to drops | Necrotizing (Malignant) OE - skull base osteomyelitis |
| Facial nerve palsy (VII), hoarseness, dysphagia | Cranial nerve involvement in malignant OE |
| Granulation tissue in the canal floor | Malignant OE |
| Previous radiotherapy to head/neck | Compromised healing |
Malignant OE requires CT scanning to assess bony erosion, MRI with gadolinium for soft tissue/intracranial extension, aggressive surgical debridement, and systemic anti-pseudomonal antibiotics (e.g., ciprofloxacin orally or IV). It carries high mortality if missed.
Otitis Media with Perforation - also consider
If there is a central perforation of the tympanic membrane, middle ear discharge will also appear at the ear canal. This is distinguished from OE by:
- Discharge is typically mucoid/mucopurulent rather than seropurulent
- Pain and itching are less prominent compared to OE
- No pain on tragal pressure (unlike OE)
- Visible perforation on otoscopy
Bottom line for practice: Most cases of ear pus + pain + itching are acute bacterial otitis externa managed with topical antibiotic-steroid drops. Avoid aminoglycoside drops if TM perforation is possible. Always check for diabetes or immunocompromise, and refer early if the condition does not respond to topical treatment.
This is a shared conversation. Sign in to Orris to start your own chat.