Closed circle system
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
I now have comprehensive information to provide a thorough answer. Here it is:
The Closed Circle System in Anesthesia
What Is the Circle System?
The circle system (also called the circle breathing system) is the most widely used breathing system in anesthesia in the United States. It gets its name from its components being arranged in a circular pathway. It prevents rebreathing of CO2 using a CO2 absorbent canister, while allowing partial or complete rebreathing of other exhaled gases.
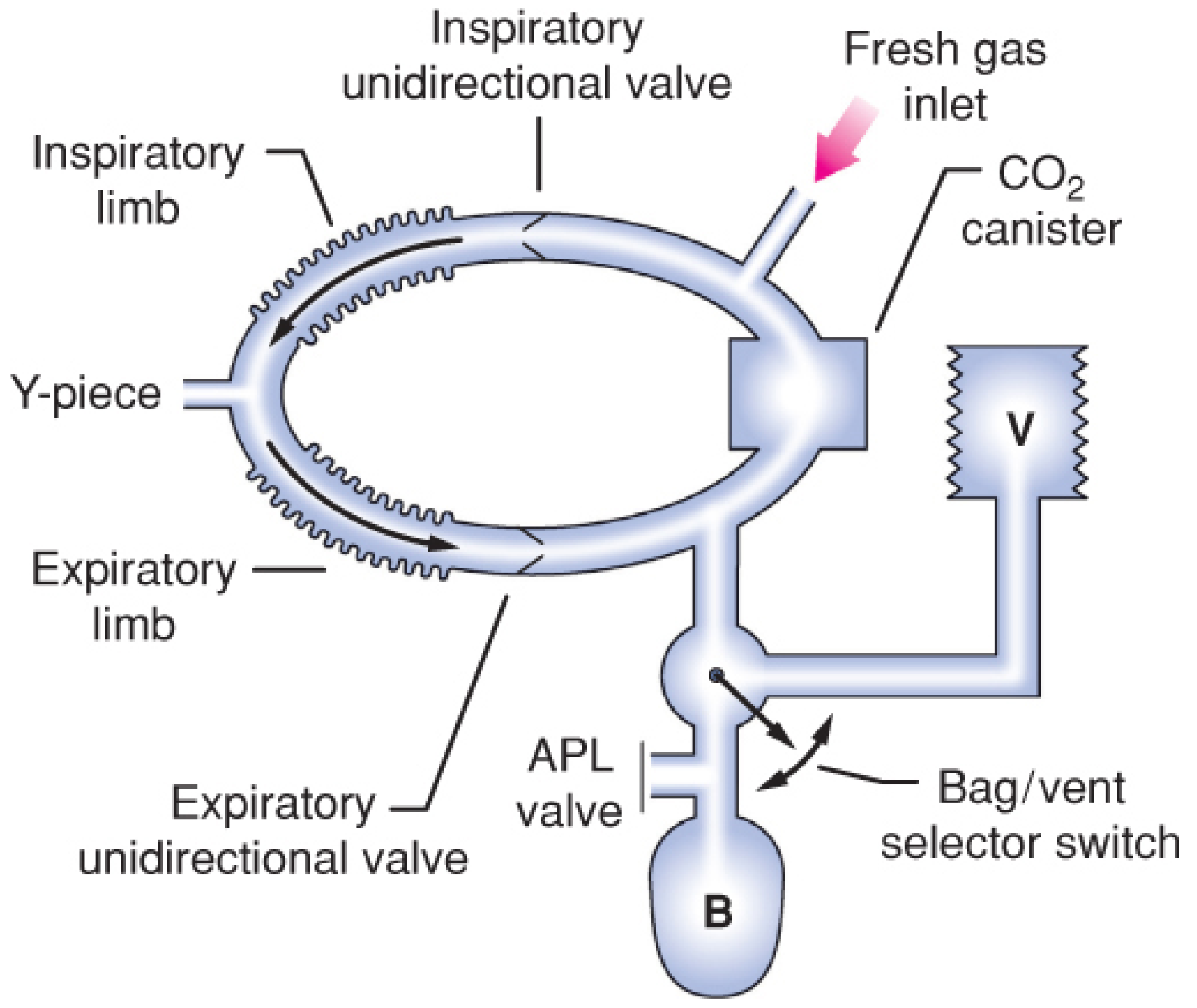
The Seven Primary Components
- Fresh gas inflow source - connects from the common gas outlet of the anesthesia workstation
- Inspiratory and expiratory unidirectional valves - ensure gas flows in one direction only
- Inspiratory and expiratory corrugated tubes - carry gases to and from the patient
- Y-piece connector - connects the circuit to the patient's airway
- APL valve (adjustable pressure-limiting / pop-off valve) - vents excess gas
- Reservoir bag - provides a gas reserve and allows manual ventilation
- CO2 absorbent canister - typically contains soda lime to chemically absorb expired CO2
Open vs. Semi-closed vs. Closed System
The circle system can operate in three modes depending on the fresh gas flow (FGF):
| Mode | FGF | Rebreathing | APL Valve |
|---|---|---|---|
| Semi-open | Very high | None | Open continuously |
| Semi-closed | Intermediate | Partial | Partially open |
| Closed | Equals patient uptake | Complete (after CO2 absorption) | Remains closed |
The closed circle system specifically means the FGF exactly matches what is consumed by the patient (O2 consumed + anesthetic agent taken up). There is complete rebreathing of all exhaled gases after CO2 absorption, and the APL (overflow) valve remains closed - no gas is vented to the scavenging system.
Three Rules to Prevent CO2 Rebreathing
Any circle arrangement must follow these three rules:
- A unidirectional valve must be on both the inspiratory and expiratory limbs, between the patient and the reservoir bag.
- Fresh gas inflow cannot enter the circuit between the expiratory valve and the patient.
- The APL (pop-off) valve cannot be located between the patient and the inspiratory valve.
Key Advantages
- Stable inspired gas concentrations - minimizes fluctuations in anesthetic depth
- Conservation of heat and humidity - exhaled warm, humidified gas is recycled; soda lime generates heat as it absorbs CO2
- Prevention of OR contamination - waste gas is contained rather than vented to the room
- Ability to use very low or closed FGF - reduces anesthetic agent consumption and cost
Performance Characteristics
- Dead space: Limited to the area distal to the Y-piece (where inspiratory and expiratory gases meet). Tube length does NOT increase dead space (unlike Mapleson circuits), but longer tubing does increase heat/moisture loss and circuit compliance.
- Resistance: The unidirectional valves and absorber add resistance, especially at high rates, though even neonates can be ventilated with a circle system.
- FGF and inspired concentration: At FGF > 5 L/min, rebreathing is so minimal a CO2 absorber is not strictly necessary. At low flows, inspired anesthetic concentration diverges significantly from the dialed vaporizer setting.
Hazards
- Complex design - typically 10+ connection sites, creating risk of misconnection, disconnection, or leaks. The ASA closed claims analysis (1997) found 25/72 adverse gas delivery claims resulted from circuit misconnections/disconnections.
- Unidirectional valve malfunction:
- Valve stuck open → CO2 rebreathing → hypercapnia
- Valve stuck closed → total circuit occlusion
- Expiratory valve stuck closed → breath stacking → barotrauma/volutrauma → can cause tension pneumothorax
- Coaxial design risk: A kinked inner tube can mimic bronchospasm (wheezing, elevated peak airway pressures, desaturation)
- Sevoflurane + desiccated soda lime: Exothermic reaction can cause airway burns or even fire/explosion - a significant safety concern
CO2 Absorbents (Soda Lime)
Soda lime is the classic CO2 absorbent. Key points:
- Silica is added to increase hardness, reducing dust inhalation risk and gas flow resistance
- A color indicator changes when the absorbent is exhausted
- Capnography (CO2 monitoring) is the most sensitive indicator of CO2 absorbent depletion
- Desiccated soda lime can react adversely with volatile anesthetics, particularly sevoflurane (produces Compound A) and desflurane
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, Ch. 25; Morgan and Mikhail's Clinical Anesthesiology, 7e, Ch. 3; Miller's Anesthesia, 10e, Ch. 6.
This is a shared conversation. Sign in to Orris to start your own chat.