Explain the Every important ECG changes and rhythmias with their treatment and also mark what changes in ECG report
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG changes arrhythmias complete guide treatment 2024
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
ECG rhythm strips arrhythmias labeled
Finding Sources
Finding Sources
Searching Images
normal ECG waveform labeled P wave QRS complex T wave intervals
Reading File
Searching Images
ST elevation myocardial infarction STEMI ECG changes leads
Searching Images
atrial fibrillation ECG irregularly irregular no P waves
Searching Images
ventricular tachycardia ECG wide complex regular rhythm
Searching Images
Wolff-Parkinson-White delta wave ECG pre-excitation
Searching Images
complete heart block third degree AV dissociation ECG
I now have comprehensive information from multiple authoritative sources. Let me compile the complete ECG guide.
Complete Guide to ECG Changes & Arrhythmias: Diagnosis and Treatment
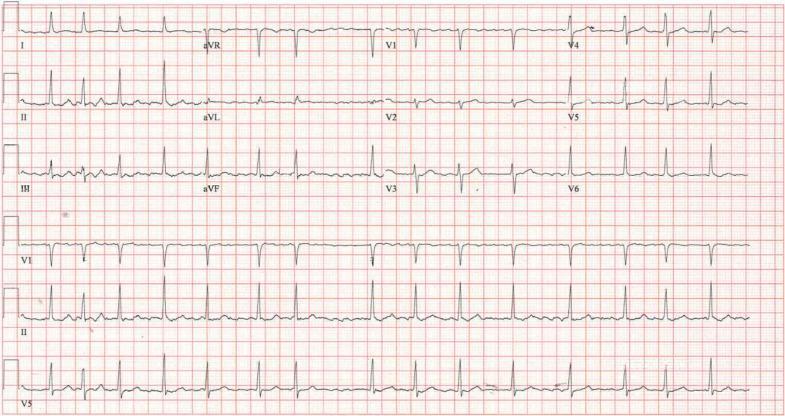
📊 PART 1 — THE NORMAL ECG: Understanding the Baseline
Before identifying abnormalities, you must know what normal looks like.

Normal ECG Components and Intervals
| Component | What It Represents | Normal Value |
|---|---|---|
| P wave | Atrial depolarization | Duration < 120 ms; upright in II, inverted in aVR |
| PR interval | AV conduction time | 120–200 ms (3–5 small squares) |
| QRS complex | Ventricular depolarization | < 120 ms (< 3 small squares) |
| QT interval | Ventricular depolarization + repolarization | < 440 ms (men), < 460 ms (women) |
| ST segment | Plateau of ventricular action potential | Isoelectric (at baseline) |
| T wave | Ventricular repolarization | Upright in I, II, V3–V6; may be inverted in aVR, V1 |
Normal Sinus Rhythm Criteria
- Rate: 60–100 bpm
- Regular P waves precede every QRS
- PR interval 120–200 ms
- Narrow QRS < 120 ms
- Normal axis: −30° to +90°
⚡ PART 2 — ARRHYTHMIAS: ECG Changes & Treatment
1. SINUS TACHYCARDIA
ECG Changes:
- Rate > 100 bpm
- Normal P waves before every QRS
- All intervals normal
Causes: Hypovolemia, fever, pain, anxiety, CHF, thyrotoxicosis, sepsis
Treatment:
- Treat the underlying cause — do NOT directly suppress the rate
- Temporary rates up to 180–200 bpm are tolerated if no underlying structural heart disease
- Miller's Anesthesia, 10e: "The goal is to treat the underlying disease state, not tachycardia"
2. SINUS BRADYCARDIA
ECG Changes:
- Rate < 60 bpm
- Normal P-QRS-T morphology
- All intervals normal
Causes: Vagal tone (athletes), hypothyroidism, hyperkalemia, hypothermia, elevated ICP, beta-blockers, digoxin, dexmedetomidine
Treatment:
- Asymptomatic: no treatment needed
- Symptomatic: Atropine 0.5–1 mg IV
- If refractory: transcutaneous or transvenous pacing
- Identify and reverse reversible causes
3. ATRIAL FIBRILLATION (AF)
ECG Changes — Mark These on Report:
- ✅ Absent P waves — replaced by chaotic fibrillatory (f) waves
- ✅ Irregularly irregular R-R intervals (hallmark feature)
- ✅ Narrow QRS (unless aberrant conduction)
- ✅ f waves most visible in V1 and inferior leads
- Rate: typically 100–160 bpm (uncontrolled)
Treatment:
| Goal | Options |
|---|---|
| Rate control | Beta-blockers (metoprolol), calcium channel blockers (diltiazem, verapamil), digoxin |
| Rhythm control | Electrical cardioversion (synchronized DC shock); pharmacologic: flecainide, amiodarone, sotalol |
| Anticoagulation | Warfarin (INR 2–3) or DOACs (rivaroxaban, apixaban) — use CHA₂DS₂-VASc score |
| Cardioversion timing | If AF < 48 hrs → cardiovert; if > 48 hrs → anticoagulate ≥ 3 weeks first or TEE-guided |
4. ATRIAL FLUTTER
ECG Changes — Mark These on Report:
- ✅ Saw-tooth flutter waves at ~300 bpm (best seen in II, III, aVF)
- ✅ Regular atrial rate (~300 bpm) with 2:1, 3:1, or 4:1 AV block
- ✅ Ventricular rate typically 150 bpm (2:1 block)
- ✅ Narrow QRS complexes
Treatment:
- Same principles as AF (rate control, rhythm control, anticoagulation)
- Radiofrequency catheter ablation is the definitive and preferred treatment (high success rate)
- Electrical cardioversion effective with lower energy than AF
- Fuster and Hurst's The Heart, 15e: "Treatment of atrial flutter is generally handled the same as for AF"
5. SUPRAVENTRICULAR TACHYCARDIA (SVT) / AVNRT
ECG Changes — Mark These on Report:
- ✅ Narrow QRS tachycardia (unless aberrant)
- ✅ Rate 150–250 bpm
- ✅ Regular rhythm
- ✅ P waves may be absent, retrograde (inverted in II), or buried in QRS
- ✅ Abrupt onset and termination ("paroxysmal")
Treatment:
| Situation | Treatment |
|---|---|
| Stable | Vagal maneuvers (Valsalva, carotid sinus massage) → Adenosine 6 mg IV rapid push (repeat 12 mg if needed) |
| Hemodynamically unstable | Synchronized cardioversion |
| Long-term prevention | Beta-blockers, calcium channel blockers, or catheter ablation |
| Pediatric | Adenosine first-line; ice to face in infants |
6. WOLFF-PARKINSON-WHITE (WPW) SYNDROME

ECG Changes — Mark These on Report:
- ✅ Short PR interval < 120 ms
- ✅ Delta wave — slurred upstroke of QRS complex (initial QRS broadening)
- ✅ Widened QRS > 120 ms
- ✅ Secondary ST-T wave changes
- ✅ Pseudo-infarct Q waves possible in inferior leads
Treatment:
- Avoid AV-nodal blocking agents (adenosine, digoxin, verapamil) in AF/flutter with WPW — risk of ventricular fibrillation via accessory pathway
- Acute tachycardia: Procainamide or electrical cardioversion
- Definitive: Radiofrequency catheter ablation of accessory pathway
7. VENTRICULAR TACHYCARDIA (VT)
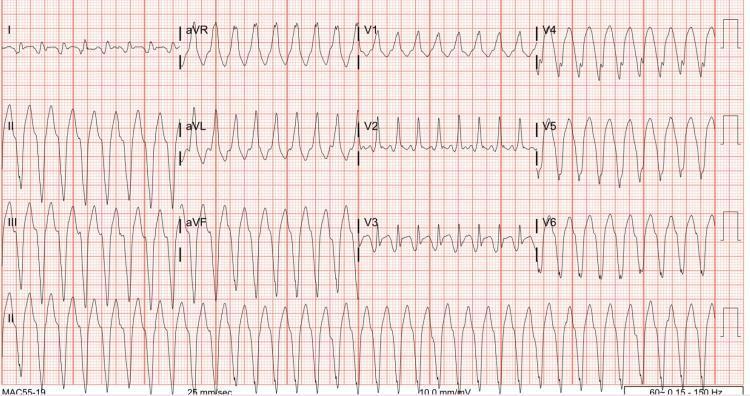
ECG Changes — Mark These on Report:
- ✅ Wide QRS > 120 ms (often > 160 ms)
- ✅ Rate 100–250 bpm, regular
- ✅ AV dissociation — P waves independent of QRS (diagnostic of VT)
- ✅ Fusion beats and capture beats (pathognomonic)
- ✅ Concordance — all precordial leads positive or negative
- ✅ Absence of typical RBBB/LBBB morphology favors VT
- Monomorphic VT: consistent QRS morphology; Polymorphic VT: changing morphology
Treatment:
| Situation | Treatment |
|---|---|
| Pulseless VT | CPR → Defibrillation (unsynchronized) → Epinephrine 1 mg IV → Amiodarone 300 mg IV |
| Stable monomorphic VT | Amiodarone 150 mg IV over 10 min; or synchronized cardioversion |
| Torsades de Pointes | IV Magnesium sulfate 2 g; correct electrolytes; overdrive pacing |
| Recurrent VT | ICD implantation; catheter ablation; antiarrhythmics (amiodarone, sotalol) |
8. VENTRICULAR FIBRILLATION (VF)
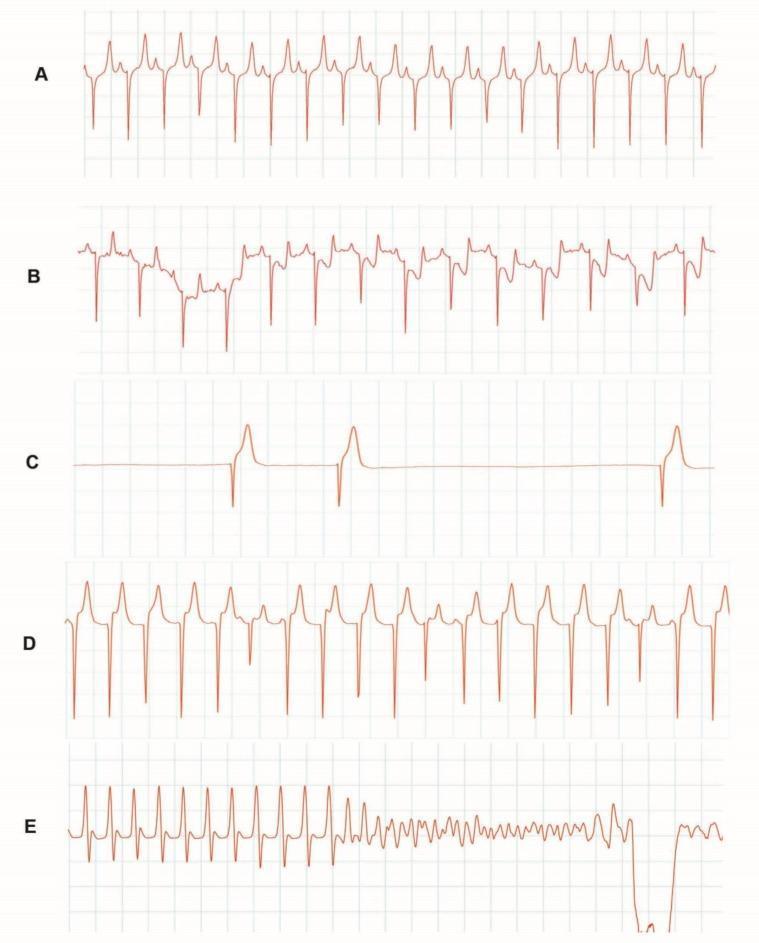
ECG Changes — Mark These on Report:
- ✅ Chaotic, irregular deflections — no organized QRS complexes
- ✅ No identifiable P waves, QRS, or T waves
- ✅ Variable amplitude and frequency of fibrillatory waves
- ✅ Coarse VF (large amplitude) vs Fine VF (small amplitude, worse prognosis)
Treatment (ACLS):
- Immediate CPR (high-quality, 100–120/min)
- Defibrillation ASAP — biphasic 200 J (monophasic 360 J)
- Epinephrine 1 mg IV every 3–5 min
- Amiodarone 300 mg IV after 3rd shock
- Treat reversible causes (4 H's and 4 T's)
9. AV HEART BLOCKS
ECG from Washington Manual showing AV block examples:
(From Washington Manual of Medical Therapeutics: PR > 200 ms = 1°, progressive PR prolongation = Mobitz I, sudden dropped beat without PR change = Mobitz II, complete dissociation = 3°)
🔹 First-Degree AV Block
ECG Changes:
- ✅ PR interval > 200 ms (> 1 large square)
- ✅ Every P wave conducts — no dropped beats
- ✅ Normal QRS
Treatment: Usually none required; investigate cause (inferior MI, increased vagal tone, digoxin)
🔹 Second-Degree AV Block — Mobitz Type I (Wenckebach)
ECG Changes — Mark These on Report:
- ✅ Progressive PR prolongation with each beat
- ✅ Dropped QRS (non-conducted P wave) after longest PR
- ✅ Group beating — periodic clustering of QRS complexes
- ✅ Shortening of RR intervals before the dropped beat
- Block usually within AV node → benign course
Treatment: Usually no treatment if asymptomatic; atropine for symptoms; rarely pacing needed
🔹 Second-Degree AV Block — Mobitz Type II
ECG Changes — Mark These on Report:
- ✅ Fixed PR interval (does not change)
- ✅ Sudden, unpredicted dropped beat (non-conducted P wave)
- ✅ Often associated with bundle branch block
- ✅ More distal block (infranodal) → higher risk of progression to complete block
Treatment: Pacemaker implantation indicated (high risk of progression to 3° block) — Harrison's Principles of Internal Medicine, 22e: "Pacemaker implantation should be performed in any patient with symptomatic bradycardia and irreversible second- or third-degree AV block"
🔹 Third-Degree (Complete) AV Block

ECG Changes — Mark These on Report:
- ✅ Complete AV dissociation — P waves and QRS march independently
- ✅ P-P intervals regular at their own rate; R-R intervals regular at slower escape rate
- ✅ Atrial rate > Ventricular rate (e.g., P at 80 bpm, QRS escape at 30–45 bpm)
- ✅ Escape QRS: narrow (junctional) or wide (ventricular)
- ✅ No PR relationship anywhere on the strip
Treatment: Permanent pacemaker (urgent); atropine or temporary pacing as bridge — Washington Manual: all atrial impulses fail to conduct to ventricles
🔴 PART 3 — ISCHEMIA & INFARCTION ECG CHANGES
ST-Elevation MI (STEMI)

ECG Changes — Mark These on Report:
- ✅ ST elevation ≥ 1 mm in ≥ 2 contiguous limb leads
- ✅ ST elevation ≥ 2 mm in ≥ 2 contiguous precordial leads
- ✅ Reciprocal ST depression in opposite leads
- ✅ Hyperacute T waves (early sign — tall, peaked, symmetric)
- ✅ Q waves develop (pathologic: > 40 ms wide or > 25% of QRS amplitude) — indicate necrosis
- ✅ T-wave inversion in evolutionary phase
Infarct Localization:
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD |
| Inferior | II, III, aVF | RCA (or LCx) |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V3 + tall R in V1 | RCA or LCx |
Treatment: Reperfusion is the priority
- Primary PCI within 90 min (preferred)
- Thrombolysis if PCI not available within 120 min
- Antiplatelet therapy (aspirin + P2Y12 inhibitor), anticoagulation, oxygen if SpO₂ < 94%
NSTEMI / Unstable Angina
ECG Changes — Mark These on Report:
- ✅ ST depression (horizontal or downsloping)
- ✅ T-wave inversions (Wellens' syndrome: deep symmetric T-wave inversion in V2–V3 = critical LAD stenosis)
- ✅ No ST elevation; troponin elevated in NSTEMI
- ✅ de Winter T waves: upsloping ST depression + tall T waves in precordials (=LAD occlusion equivalent)
🔑 PART 4 — OTHER CRITICAL ECG CHANGES
Long QT Syndrome
ECG Changes:
- ✅ QTc > 440 ms (men) or > 460 ms (women)
- ✅ Risk of Torsades de Pointes (polymorphic VT with rotating QRS axis)
- Causes: Congenital (LQTS 1–3), drugs (antiarrhythmics, antibiotics, antipsychotics), hypokalemia, hypomagnesemia
Treatment: Remove offending drugs, correct electrolytes, IV magnesium, beta-blockers (congenital), ICD
Bundle Branch Blocks
| Feature | RBBB | LBBB |
|---|---|---|
| QRS duration | > 120 ms | > 120 ms |
| V1 morphology | RSR' pattern ("rabbit ears") | Broad, notched S wave (QS or rS) |
| V6 morphology | Broad, slurred S wave | Tall, notched R wave (no Q, no S) |
| T-wave | Inverted in V1–V3 | Discordant (opposite to QRS) |
| Clinical significance | Often incidental | Suggests significant LV disease; new LBBB = treat as STEMI |
Hyperkalemia
ECG Changes (progressive with rising K⁺):
- ✅ K⁺ > 5.5: Tall, peaked, narrow T waves (tenting)
- ✅ K⁺ > 6.5: Widened PR, flattened P waves
- ✅ K⁺ > 7.0: Wide QRS, "sine-wave" pattern
- ✅ K⁺ > 8.0: VF or asystole
Treatment: Calcium gluconate (membrane stabilization) → insulin + dextrose → sodium bicarbonate → dialysis
Hypokalemia
ECG Changes:
- ✅ Flattened or inverted T waves
- ✅ Prominent U waves (after T wave)
- ✅ ST depression
- ✅ Risk of VT/VF
Pericarditis
ECG Changes (diffuse, all leads):
- ✅ Diffuse concave (saddle-shaped) ST elevation in most leads
- ✅ PR depression (especially in II and V4–V6) — key distinguishing feature from STEMI
- ✅ No reciprocal changes (unlike STEMI)
- ✅ No Q waves
Pulmonary Embolism (PE)
ECG Changes:
- ✅ S1Q3T3 pattern — S wave in I, Q wave and T-wave inversion in III
- ✅ New RBBB (right heart strain)
- ✅ Sinus tachycardia (most common finding)
- ✅ T-wave inversions V1–V4 (right heart strain)
📋 QUICK REFERENCE: ECG Report Annotations
| Finding | What to Mark on Report |
|---|---|
| PR > 200 ms | "1st degree AV block — prolonged PR" |
| Dropped beats with progressive PR | "2nd degree AV block — Mobitz I (Wenckebach)" |
| Sudden dropped beats, fixed PR | "2nd degree AV block — Mobitz II — pacing consult" |
| AV dissociation, slow escape | "3rd degree (complete) AV block — urgent pacing" |
| Absent P waves, irregular RR | "Atrial fibrillation — rate XXX bpm" |
| Saw-tooth at 300 bpm | "Atrial flutter — 2:1 block" |
| Short PR + delta wave | "WPW pattern — accessory pathway" |
| Wide QRS tachycardia | "Wide complex tachycardia — rule out VT" |
| Chaotic baseline, no QRS | "Ventricular fibrillation — code blue" |
| ST elevation ≥ 1 mm, 2 leads | "STEMI — [territory] — activate cath lab" |
| New LBBB with chest pain | "Presumed STEMI equivalent — activate cath lab" |
| QTc > 500 ms | "Prolonged QT — risk of TdP — review medications" |
| RSR' in V1 | "RBBB pattern" |
| Peaked narrow T waves | "Hyperkalemia — check K⁺ urgently" |
| Diffuse saddle ST + PR depression | "Pericarditis pattern" |
| S1Q3T3 + sinus tach | "Possible PE pattern — clinical correlation" |
Sources: Washington Manual of Medical Therapeutics, Miller's Anesthesia 10e, Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine 22e, Fuster and Hurst's The Heart 15e, Katzung's Basic and Clinical Pharmacology 16e
This is a shared conversation. Sign in to Orris to start your own chat.